Download as pptx, pdf, or txt
You might also like
- Myles Textbook For Midwives 16th Edition 2014 PDFDocument799 pagesMyles Textbook For Midwives 16th Edition 2014 PDFRayan Abu Hammad85% (26)
- Introduction To Clinical TrialsDocument31 pagesIntroduction To Clinical Trialsmuhammad murtaza89% (9)
- Iran - Geert HofstedeDocument2 pagesIran - Geert Hofstedemoro1381No ratings yet
- Good Clinical Practice PrinciplesDocument20 pagesGood Clinical Practice Principlesrajneesh kumarNo ratings yet
- Nurses Group Paediatric Committee Chemotherapy Safe Preparation and Administration - M. Stenvall - May 2015Document26 pagesNurses Group Paediatric Committee Chemotherapy Safe Preparation and Administration - M. Stenvall - May 2015Vinitha SekaranNo ratings yet
- Dhyg 415 Study Guide Yezi Pang - 1Document117 pagesDhyg 415 Study Guide Yezi Pang - 1api-473128642No ratings yet
- International Regulatory Requirements On Clinical Trails and Data ManagementDocument19 pagesInternational Regulatory Requirements On Clinical Trails and Data ManagementJay PraveenNo ratings yet
- BupivacaínaDocument13 pagesBupivacaínaDiana RuizNo ratings yet
- Journal IkgaDocument8 pagesJournal IkgaMisshaNo ratings yet
- Mesa Redonda Anestesia Local en OdontopediatríaDocument10 pagesMesa Redonda Anestesia Local en OdontopediatríaLeticia Quiñonez VivasNo ratings yet
- Good Clinical Practices Concepts and Case Studies Kim IsaacsDocument21 pagesGood Clinical Practices Concepts and Case Studies Kim IsaacsChandra Shekar GNo ratings yet
- Anesthetic Efficacy of Buccal Infiltration Articaine Versus Lidocaine For Extraction of Primary Molar TeethDocument5 pagesAnesthetic Efficacy of Buccal Infiltration Articaine Versus Lidocaine For Extraction of Primary Molar TeethFabro BianNo ratings yet
- 1063 FullDocument10 pages1063 FullJavier Farias VeraNo ratings yet
- Jurnal 2 (Bing)Document6 pagesJurnal 2 (Bing)Vito OeiNo ratings yet
- Pediatrics & TherapeuticsDocument7 pagesPediatrics & TherapeuticsAmit PasiNo ratings yet
- Journal Neonatal Skin CareDocument22 pagesJournal Neonatal Skin CareNia Ratna RukhiaNo ratings yet
- Highlight Bubu 2Document7 pagesHighlight Bubu 2soniNo ratings yet
- Proposal PresentationDocument37 pagesProposal PresentationAnkana BhowmikNo ratings yet
- General Anathesia MSCDocument48 pagesGeneral Anathesia MSCNahla OthmanNo ratings yet
- Nonfluoride Caries-Preventive Agents New GuidelinesDocument6 pagesNonfluoride Caries-Preventive Agents New GuidelinesCarmen Iturriaga GuajardoNo ratings yet
- Treatment of Anal Fissure by Lidocaine, Emla, GTNDocument34 pagesTreatment of Anal Fissure by Lidocaine, Emla, GTNHendra AjahNo ratings yet
- Anesthesia Onset Time and Injection Pain Between Buffered and Unbuffered Lidocaine Used As Local Anesthetic For Dental Care in ChildrenDocument4 pagesAnesthesia Onset Time and Injection Pain Between Buffered and Unbuffered Lidocaine Used As Local Anesthetic For Dental Care in ChildrenFernando MenesesNo ratings yet
- Lidocaina Versus Articaina 2021Document7 pagesLidocaina Versus Articaina 2021Francisca Abarca CifuentesNo ratings yet
- By: Kris Traver and Nitin JainDocument14 pagesBy: Kris Traver and Nitin JainMahesh BhagwatNo ratings yet
- Embedded R D China Interv Trial AMR 29.05.2019 V1aDocument17 pagesEmbedded R D China Interv Trial AMR 29.05.2019 V1aAnonymous gVgLS4No ratings yet
- Complicaciones en Sedacion Endovenosa en Tratamientos Dentales en Pacientes Con Discapacidad Mental 2015Document6 pagesComplicaciones en Sedacion Endovenosa en Tratamientos Dentales en Pacientes Con Discapacidad Mental 2015Carlos AlfaroNo ratings yet
- Cost Consequences StudyDocument4 pagesCost Consequences StudySankita SandalNo ratings yet
- Update On ART-2010Document30 pagesUpdate On ART-2010danayanto sumbungNo ratings yet
- Nonpharmacologic Intervention On The Prevention of Pain and Anxiety During Pediatric Dental Care: A Systematic ReviewDocument11 pagesNonpharmacologic Intervention On The Prevention of Pain and Anxiety During Pediatric Dental Care: A Systematic ReviewJorge Luis Ramos MaqueraNo ratings yet
- Scms 6s 6-16 Hawaiisppl v9Document28 pagesScms 6s 6-16 Hawaiisppl v9Michele CarvalhoNo ratings yet
- Drug Discovery - New Drug Development Process: Dr. Vikram Kumar (Yadav), M.Pharm PHD PharmacologyDocument42 pagesDrug Discovery - New Drug Development Process: Dr. Vikram Kumar (Yadav), M.Pharm PHD PharmacologyPranav NakhateNo ratings yet
- Lidocaine Lozenges For Pharyngeal Anesthesia DurinDocument6 pagesLidocaine Lozenges For Pharyngeal Anesthesia DurinpaulaNo ratings yet
- Early Analgesia For Children With Acute Abdominal Pain: ObjectivesDocument8 pagesEarly Analgesia For Children With Acute Abdominal Pain: Objectivescrizt tyanNo ratings yet
- Intranasal Ketamine For Procedural Sedation and Analgesia in Children: A Systematic ReviewDocument15 pagesIntranasal Ketamine For Procedural Sedation and Analgesia in Children: A Systematic ReviewNADIA VICUÑA CRIADONo ratings yet
- 2019 - Postoperative Healing Assessment Using Cannabinoids in Oral SurgeryDocument7 pages2019 - Postoperative Healing Assessment Using Cannabinoids in Oral SurgerycorcarolNo ratings yet
- Wa0012.Document4 pagesWa0012.Sreeja ReddyNo ratings yet
- Statement:: INT0038 Academic English For Engineering and ScienceDocument31 pagesStatement:: INT0038 Academic English For Engineering and ScienceRamsey MakeriNo ratings yet
- Clinical Trial Regulation in NepalDocument7 pagesClinical Trial Regulation in NepalB.pharm 16th BatchNo ratings yet
- SOPs For Medical Doctors For POCSO ImplementationDocument26 pagesSOPs For Medical Doctors For POCSO ImplementationKaran KaushikNo ratings yet
- 4417-Article Text-13279-1-10-20210917Document6 pages4417-Article Text-13279-1-10-20210917Lamessa MessiNo ratings yet
- I Reason For Choosing The Topic: Intervention (CNPG)Document3 pagesI Reason For Choosing The Topic: Intervention (CNPG)ErikaCacatianNo ratings yet
- Notes - Up Till September 9, 2021Document40 pagesNotes - Up Till September 9, 2021vedant wakankarNo ratings yet
- Evidence Based MedicineDocument55 pagesEvidence Based MedicinePutri IntanNo ratings yet
- Clinical Trial Gadavala SarahDocument60 pagesClinical Trial Gadavala SarahSejal khuman100% (1)
- Clinical TrialsDocument16 pagesClinical TrialsAndrewTiamoNo ratings yet
- Aao-Hnsf Dysphonia CPG Slideset March2018 New Template 1-1Document53 pagesAao-Hnsf Dysphonia CPG Slideset March2018 New Template 1-1Dinne QuindipanNo ratings yet
- 01 Drug Development ProcessDocument37 pages01 Drug Development ProcessDrvinay GoudNo ratings yet
- Rational Prescribing and Dispensing GNK585 - 18C - 2024 - Reading MaterialDocument67 pagesRational Prescribing and Dispensing GNK585 - 18C - 2024 - Reading Materialu20433621No ratings yet
- Bioethics 3rd 4rth Week TopicsDocument21 pagesBioethics 3rd 4rth Week TopicsWendell Gian GolezNo ratings yet
- Thin Layr ChromatographyDocument9 pagesThin Layr ChromatographySurbhi BattaNo ratings yet
- Study DesignsDocument36 pagesStudy Designsz6f9cw8vwvNo ratings yet
- Comparison of Long-Term Outcomes Between Ferric Sulfate Pulpotomy and Indirect Pulp Therapy in Primary MolarsDocument4 pagesComparison of Long-Term Outcomes Between Ferric Sulfate Pulpotomy and Indirect Pulp Therapy in Primary MolarsEstaf EmkeyzNo ratings yet
- Medicine (Pharmaceutical Chemistry)Document33 pagesMedicine (Pharmaceutical Chemistry)Crizaldo MempinNo ratings yet
- NQB Hum Fact ConcordDocument22 pagesNQB Hum Fact ConcordSophia RoseNo ratings yet
- Evidence Based Medicine: Jan Baptist Van HelmontDocument4 pagesEvidence Based Medicine: Jan Baptist Van HelmontKabirNo ratings yet
- A Comparison of The Efficacy and Safety of Incobotulin - 2013 - Journal of The ADocument1 pageA Comparison of The Efficacy and Safety of Incobotulin - 2013 - Journal of The ADuy Nguyễn ĐứcNo ratings yet
- Infection Control PracticeDocument6 pagesInfection Control PracticeMia AmeliaNo ratings yet
- Bioethicshxcare Issues TopicsDocument22 pagesBioethicshxcare Issues TopicsJan Oliver Yares100% (1)
- Comparative Efficacy of Anti-Epileptic Drugs For Neonatal Seizures: A Network Meta - AnalysisDocument8 pagesComparative Efficacy of Anti-Epileptic Drugs For Neonatal Seizures: A Network Meta - AnalysisSultan Rahmat SeptianNo ratings yet
- Satisfaction With Orthodontic Treatment Outcome: Original ArticleDocument7 pagesSatisfaction With Orthodontic Treatment Outcome: Original ArticleVANESA REYESNo ratings yet
- Articulo DentalDocument7 pagesArticulo DentalV DreamerNo ratings yet
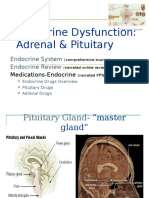
- Endocrine Dysfunction: Adrenal & Pituitary: Endocrine System Endocrine ReviewDocument102 pagesEndocrine Dysfunction: Adrenal & Pituitary: Endocrine System Endocrine ReviewCalimlim KimNo ratings yet
- TIPqc CAPSTONE MANUAL ArchDesign 9Document26 pagesTIPqc CAPSTONE MANUAL ArchDesign 9Cheska ChangcoNo ratings yet
- Astrero - 5070 - Activity ViiDocument17 pagesAstrero - 5070 - Activity ViiAstrero Kristle Jeian V.No ratings yet
- Session 5 DASS 21 Knowing Myself Through Psychological Testing PDF Lecture Notes-1Document14 pagesSession 5 DASS 21 Knowing Myself Through Psychological Testing PDF Lecture Notes-1Ika PinkNo ratings yet
- Time Table & Candidates Instruction - October November 2023Document11 pagesTime Table & Candidates Instruction - October November 2023Abdullah Mohamed ZakariahNo ratings yet
- The Importance of Antenatal CareDocument3 pagesThe Importance of Antenatal CareChennulNo ratings yet
- What Is Ecotherapy - Nature Therapy For Beginners - Everyday HealthDocument19 pagesWhat Is Ecotherapy - Nature Therapy For Beginners - Everyday HealthAntonio ZafraNo ratings yet
- FAMSA MSA ListDocument17 pagesFAMSA MSA ListMiracle BeedeNo ratings yet
- Basic Facial With MusicDocument4 pagesBasic Facial With Musicapi-305903882No ratings yet
- Hair Care and Oral CareDocument8 pagesHair Care and Oral Care22 - Fernandez, Lyza Mae D.No ratings yet
- Spartan Growth Natural Testosterone AscendancyDocument9 pagesSpartan Growth Natural Testosterone Ascendancynikolaaaaa33No ratings yet
- Class XII Physical Education 100 Viva Questions With AnswersDocument6 pagesClass XII Physical Education 100 Viva Questions With AnswersjineditingtutorialsNo ratings yet
- Screenshot 2023-03-28 at 8.22.35 PMDocument5 pagesScreenshot 2023-03-28 at 8.22.35 PMRitika PrakashNo ratings yet
- R.A. 9710 Magna Carta On WomenDocument17 pagesR.A. 9710 Magna Carta On WomenYappie YappieNo ratings yet
- 3 PeDocument2 pages3 PeJerwin GritNo ratings yet
- The Code On Sanitation of The PhilippinesDocument66 pagesThe Code On Sanitation of The PhilippinesJhoanne DelloroNo ratings yet
- 2023 Advantage: Drug ListDocument159 pages2023 Advantage: Drug ListPatrick StalterNo ratings yet
- Grand Nursing Theory Assignment FormDocument2 pagesGrand Nursing Theory Assignment Formapi-488538030No ratings yet
- Ethics: Bachelor of Elementary Education 2A First Semester A.Y 2021-2022 Challenges To Ethical Behavior (Outline)Document7 pagesEthics: Bachelor of Elementary Education 2A First Semester A.Y 2021-2022 Challenges To Ethical Behavior (Outline)Dale Francis Dechavez RutagenesNo ratings yet
- Summer Capital of Cebu Vegetable Basket of Central VisayaDocument27 pagesSummer Capital of Cebu Vegetable Basket of Central VisayaDatus AlonsoNo ratings yet
- Ankle-Foot Orthosis Made by 3D Printing TechniqueDocument7 pagesAnkle-Foot Orthosis Made by 3D Printing Techniquejose diazNo ratings yet
- Cancer Screening and Prevention:: Eliminating Deaths From Cervical CancerDocument45 pagesCancer Screening and Prevention:: Eliminating Deaths From Cervical CancerYingting ZooNo ratings yet
- New Rosevale Application For Admission 1Document4 pagesNew Rosevale Application For Admission 1Verscel Malalis GuisadioNo ratings yet
- PECs Self Rating Questionnaire Scoring Sheet 1Document2 pagesPECs Self Rating Questionnaire Scoring Sheet 1Rodrigo SuarezNo ratings yet
- Nursing Care Plan Cues Nursing Diagnosis Objectives Interventions Rationale EvaluationDocument2 pagesNursing Care Plan Cues Nursing Diagnosis Objectives Interventions Rationale EvaluationLi Luren Raphaelle TanNo ratings yet
- Khagarajpoudel 2Document3 pagesKhagarajpoudel 2Apex BasnetNo ratings yet
- Applied Linguistics: Assignment ofDocument12 pagesApplied Linguistics: Assignment ofHoa Hải Đường100% (1)
- Module 6Document22 pagesModule 6Jhoanna Lovely OntulanNo ratings yet