2.tension Pneumothorax
2.tension Pneumothorax
Download as pptx, pdf, or txt
You might also like
- FRCPath OSPE 25042014Document11 pagesFRCPath OSPE 25042014monday125No ratings yet
- Disorders Involving Gender and Sexuality EditedDocument10 pagesDisorders Involving Gender and Sexuality EditedMike ChavezNo ratings yet
- Discharge SummaryDocument2 pagesDischarge SummaryRoshan Lewis0% (1)
- Chest TraumaDocument115 pagesChest TraumaЕвгений ХанькоNo ratings yet
- PneumothoraxDocument30 pagesPneumothoraxsanjivdas100% (1)
- Tension PneumothoraxDocument18 pagesTension PneumothoraxmeviraNo ratings yet
- Chest Trauma ManagementDocument78 pagesChest Trauma ManagementHassan Shoukat100% (1)
- SplintsDocument3 pagesSplintsmuhammad naeem33% (3)
- PNEUMOTHORAXDocument33 pagesPNEUMOTHORAXRAMJIBAN YADAVNo ratings yet
- Penumothorax 2024Document73 pagesPenumothorax 2024mohamadfarid6666No ratings yet
- CSS Trauma ThoraxDocument50 pagesCSS Trauma ThoraxNurmalia PutriNo ratings yet
- An Overview of The Pulmonary SystemDocument44 pagesAn Overview of The Pulmonary SystemyormahdNo ratings yet
- Surgical Radiology Chest TraumaDocument24 pagesSurgical Radiology Chest Traumaraybiley8No ratings yet
- CPGPCCN Respiratory System Adult PneumothoraxDocument2 pagesCPGPCCN Respiratory System Adult PneumothoraxXxmhdixXNo ratings yet
- Trauma Thorax: Disusun Oleh: Uray Ria ApriniDocument22 pagesTrauma Thorax: Disusun Oleh: Uray Ria ApriniUray RiaNo ratings yet
- Tension Pneumothorax 170102133730Document21 pagesTension Pneumothorax 170102133730novelraaaNo ratings yet
- Torso TraumaDocument37 pagesTorso TraumaFiza MushtaqNo ratings yet
- Tension Pneumothorax: Anak Agung Istri Intan YuniariDocument19 pagesTension Pneumothorax: Anak Agung Istri Intan Yuniarifaris nagibNo ratings yet
- Pneumothorax: Narmada Kasuni Group 25 5 Year 1 SemesterDocument18 pagesPneumothorax: Narmada Kasuni Group 25 5 Year 1 SemesterNarmada PemathilakaNo ratings yet
- Chest InjuriesDocument25 pagesChest InjuriesMariya DantisNo ratings yet
- SESSION 12 - Tension PneumothoraxDocument22 pagesSESSION 12 - Tension PneumothoraxLinux KaikaNo ratings yet
- 766 - HPS - Emergency TKVDocument82 pages766 - HPS - Emergency TKVAdistyDWNo ratings yet
- Spontaneous Pneumothorax For General Surgical Residents: Facebook: Happy Friday Knight January, 12, 2018 ThailandDocument64 pagesSpontaneous Pneumothorax For General Surgical Residents: Facebook: Happy Friday Knight January, 12, 2018 ThailandGrace SomsirivattanaNo ratings yet
- Chest TraumaDocument39 pagesChest Traumayared getachewNo ratings yet
- Chest Trauma Leading To Surgery: Surgeons DemandDocument55 pagesChest Trauma Leading To Surgery: Surgeons Demandmark chrisatyaNo ratings yet
- Airway Ventilation and Chest TraumaDocument12 pagesAirway Ventilation and Chest Traumatunde adeniranNo ratings yet
- Chest Trauma and Thorocic InjuriesDocument17 pagesChest Trauma and Thorocic Injuriespreet kaurNo ratings yet
- Surgery TCVS SGD Guide KKDocument7 pagesSurgery TCVS SGD Guide KKFu Xiao ShanNo ratings yet
- HemothoraxDocument27 pagesHemothoraxShreyasi AnkushNo ratings yet
- Chest Trauma: Annet Mary Mathew Anu Krishna Arathi.KDocument60 pagesChest Trauma: Annet Mary Mathew Anu Krishna Arathi.KAsif AbbasNo ratings yet
- PneumothoraxDocument30 pagesPneumothoraxnorhazirah hassanNo ratings yet
- DR Ahmed..thorasic SurgeryDocument20 pagesDR Ahmed..thorasic Surgeryمحمد رافد لطيفNo ratings yet
- Trauma Thorax Atls 9 Edition: Amatillah RaifahDocument20 pagesTrauma Thorax Atls 9 Edition: Amatillah RaifahAnnifa RaifaNo ratings yet
- Trauma Thorax Atls 9 Edition: Amatillah RaifahDocument20 pagesTrauma Thorax Atls 9 Edition: Amatillah RaifahAnnifa RaifaNo ratings yet
- Chest TraumaDocument62 pagesChest TraumaayouNo ratings yet
- Pneumothorax 1Document53 pagesPneumothorax 1Tara BasnetNo ratings yet
- AtelectasisDocument30 pagesAtelectasisashoaib0313No ratings yet
- HematotoraksDocument15 pagesHematotorakssafanj12No ratings yet
- Pneumothorax: - Hitesh Rohit (3 Year B.P.T.)Document22 pagesPneumothorax: - Hitesh Rohit (3 Year B.P.T.)Hitesh RohitNo ratings yet
- Pneumothorax: - Hitesh Rohit (3 Year B.P.T.)Document22 pagesPneumothorax: - Hitesh Rohit (3 Year B.P.T.)Hitesh RohitNo ratings yet
- Chest TraumaDocument41 pagesChest TraumaSharfuddin ChowdhuryNo ratings yet
- Pneumothorax AmierDocument7 pagesPneumothorax Amieramier90No ratings yet
- 5-Thoracic Surgery PT &ot 2023-2024-1Document114 pages5-Thoracic Surgery PT &ot 2023-2024-1MUGISHA GratienNo ratings yet
- Chest Trauma BCECDocument25 pagesChest Trauma BCECTandin SonamNo ratings yet
- Chest TraumaDocument9 pagesChest Traumaapi-3838240100% (7)
- Nursing Care of Patients With Pneumothorax: Prepared By: N. WadeDocument33 pagesNursing Care of Patients With Pneumothorax: Prepared By: N. WadeokaciaNo ratings yet
- DR M Abdur Rahim M.D.:, Asst. Professor of MedicineDocument43 pagesDR M Abdur Rahim M.D.:, Asst. Professor of Medicinedr_abdurNo ratings yet
- RADPATHO Module 5Document140 pagesRADPATHO Module 5daphne09tayagNo ratings yet
- Pneumothorax, Tension and TraumaticDocument24 pagesPneumothorax, Tension and TraumaticSatria WibawaNo ratings yet
- Macro PneumohemoDocument28 pagesMacro PneumohemoSiti AishahNo ratings yet
- Advanced Trauma Life Support (Atls) : DR Eko Setiawan, SpotDocument67 pagesAdvanced Trauma Life Support (Atls) : DR Eko Setiawan, Spotyuliana khairiNo ratings yet
- Chest Tube Insertion: Prepare By: Amrita:Thapa Roll No. 7Document39 pagesChest Tube Insertion: Prepare By: Amrita:Thapa Roll No. 7sushma shresthaNo ratings yet
- Approach To Spontaneous PneumothoraxDocument25 pagesApproach To Spontaneous PneumothoraxMohdGhazaliAcoyNo ratings yet
- Anaesthesia ENT SurgeryDocument61 pagesAnaesthesia ENT Surgeryakanksha singhNo ratings yet
- Hemopneumothorax: Iskander Al-GithmiDocument21 pagesHemopneumothorax: Iskander Al-GithmiArithaNo ratings yet
- BST (DR M)Document30 pagesBST (DR M)Elsa Yosephine -Co-AsstNo ratings yet
- 31-Chest TraumaDocument46 pages31-Chest TraumaYosra —No ratings yet
- Torso TraumaDocument58 pagesTorso TraumaAbidisHereNo ratings yet
- Unit V (E) Management of Patients With Obstructive Lung DiseasesDocument25 pagesUnit V (E) Management of Patients With Obstructive Lung DiseasesArooj FatimaNo ratings yet
- What Is Ultrasound?Document15 pagesWhat Is Ultrasound?Al-Mukashfi TahaNo ratings yet
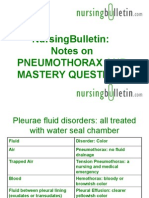
- NursingBulletin Notes On PneumothoraxDocument27 pagesNursingBulletin Notes On Pneumothoraxseigelystic100% (11)
- Empyema Thoracis: Ain Najwa BT Abd Rahim (090100457) MARDHIAH BT MARZUKI (090100470)Document22 pagesEmpyema Thoracis: Ain Najwa BT Abd Rahim (090100457) MARDHIAH BT MARZUKI (090100470)Dumora FatmaNo ratings yet
- Truma Slide 4 Chest TrumaDocument38 pagesTruma Slide 4 Chest TrumaadnanreshunNo ratings yet
- 26. Typhoid Fever (Enteric Fever)Document19 pages26. Typhoid Fever (Enteric Fever)patriciacharles096No ratings yet
- 27.Viral and Preotozal DiarrheaDocument17 pages27.Viral and Preotozal Diarrheapatriciacharles096No ratings yet
- 3.TAKING PATIENT HISTORYDocument56 pages3.TAKING PATIENT HISTORYpatriciacharles096No ratings yet
- 02_Principles_of_Antimicrobials-convertedDocument23 pages02_Principles_of_Antimicrobials-convertedpatriciacharles096No ratings yet
- Session23_BronchiolitisDocument21 pagesSession23_Bronchiolitispatriciacharles096No ratings yet
- 25.pyodermaDocument43 pages25.pyodermapatriciacharles096No ratings yet
- Gyconological Examination ExampleDocument34 pagesGyconological Examination Examplepatriciacharles096No ratings yet
- DMDocument44 pagesDMpatriciacharles096No ratings yet
- PROCEDURES FOR MEDICINE STORAGE(0)Document24 pagesPROCEDURES FOR MEDICINE STORAGE(0)patriciacharles096No ratings yet
- Basics of Pharm & Rule of DispensingDocument25 pagesBasics of Pharm & Rule of Dispensingpatriciacharles096No ratings yet
- 25. AntidotesDocument26 pages25. Antidotespatriciacharles096No ratings yet
- PrescriptionsDocument15 pagesPrescriptionspatriciacharles096No ratings yet
- 17. AntihypertensiveDocument35 pages17. Antihypertensivepatriciacharles096No ratings yet
- 14. Cough RemediesDocument20 pages14. Cough Remediespatriciacharles096No ratings yet
- 1.hemorrhagic and Haemolytic Disease of The NewbornDocument12 pages1.hemorrhagic and Haemolytic Disease of The Newbornpatriciacharles096No ratings yet
- Intestinal ObstructionDocument92 pagesIntestinal Obstructionpatriciacharles096No ratings yet
- Beta-Lactam_AntibioticsDocument30 pagesBeta-Lactam_Antibioticspatriciacharles096No ratings yet
- Erythroblastic SynartesisDocument11 pagesErythroblastic SynartesisKata TölgyesiNo ratings yet
- شرح ميكروبيولوچي كاملDocument35 pagesشرح ميكروبيولوچي كاملslmylwkaaNo ratings yet
- Context CluesDocument26 pagesContext CluesEstrella manzanoNo ratings yet
- Burn Injuries FdneDocument25 pagesBurn Injuries FdneRonit ChandNo ratings yet
- NP1 NotesDocument59 pagesNP1 NotesBrianMarBeltran100% (1)
- SocioEnvironmental ApproachDocument4 pagesSocioEnvironmental ApproachMARVIN GROUPNo ratings yet
- Skin Integrity and Wound CareDocument38 pagesSkin Integrity and Wound CareMiu MiuNo ratings yet
- Session 1 - Hasanudin - Breathing Exercises Asthma With CommentsDocument25 pagesSession 1 - Hasanudin - Breathing Exercises Asthma With Commentsrenata JeslynNo ratings yet
- Lecture Notes On PsychiatryDocument38 pagesLecture Notes On PsychiatrysrossgellNo ratings yet
- Neonatal Respiratory System Updates 2020Document824 pagesNeonatal Respiratory System Updates 2020link_wolfloboNo ratings yet
- Critical Care Environment - Design Stucture and FacilitiesDocument22 pagesCritical Care Environment - Design Stucture and FacilitiesProf. Ramsharan MehtaNo ratings yet
- Aubf Midterm Microscopic ExaminationsDocument10 pagesAubf Midterm Microscopic Examinationsrosalyn.asaniNo ratings yet
- Temperature Record: Patient'S Name: Age: Sex: Attending PhysicianDocument2 pagesTemperature Record: Patient'S Name: Age: Sex: Attending PhysicianAina HaravataNo ratings yet
- Neural Tube DefectsDocument5 pagesNeural Tube DefectsAnjesh100% (1)
- Ot Role BurnsDocument2 pagesOt Role BurnsgelbernalotrpNo ratings yet
- Post Stroke WritingDocument9 pagesPost Stroke WritingAdi ParamarthaNo ratings yet
- Cardiac Monitoring and ECG Lesson PlanDocument8 pagesCardiac Monitoring and ECG Lesson PlanIshfaq RatherNo ratings yet
- Doctors ListDocument17 pagesDoctors ListRikke LegarthNo ratings yet
- BASIC HOSPITAL PROCEDURES_1Document76 pagesBASIC HOSPITAL PROCEDURES_1vitalisbekko100% (1)
- α-Synuclein in Lewy bodiesDocument2 pagesα-Synuclein in Lewy bodiesCsalok EzfragNo ratings yet
- Atrioventricular Block (Heart Block) : Causes of Atrio-Ventricular BlockDocument10 pagesAtrioventricular Block (Heart Block) : Causes of Atrio-Ventricular BlockLiza M. PurocNo ratings yet
- Mycobacterium Tuberculosis and Tuberculosis - TodarDocument18 pagesMycobacterium Tuberculosis and Tuberculosis - TodarTanti Dewi WulantikaNo ratings yet
- Wang 2017Document10 pagesWang 2017vania adheliaNo ratings yet
- CHED2 0104498631190COIN V3 enDocument4 pagesCHED2 0104498631190COIN V3 enARIF AHAMMED PNo ratings yet
- L 1 Introduction and Types of ImmunityDocument13 pagesL 1 Introduction and Types of ImmunityaugustongoviNo ratings yet
- Poultry Medication: Product Indication Composition Reg No G979 G1305Document1 pagePoultry Medication: Product Indication Composition Reg No G979 G1305irfan syuhada100% (1)