JNM
J Neurogastroenterol Motil, Vol. 27 No. 3 July, 2021
pISSN: 2093-0879 eISSN: 2093-0887
https://doi.org/10.5056/jnm19195
Journal of Neurogastroenterology and Motility
Original Article
Gastric Emptying Time and Volume of the Small
Intestine as Objective Markers in Patients With
Symptoms of Diabetic Enteropathy
Mette W Klinge,1* Nanna Sutter,1 Esben B Mark,2 Anne-Mette Haase,1 Per Borghammer,3,4 Vincent Schlageter,5 Sten Lund,6,7
Jesper Fleischer,7,8 Karoline Knudsen,3 Asbjørn M Drewes,2 and Klaus Krogh1,7
1
Department of Hepatology and Gastroenterology, Aarhus University Hospital, Denmark; 2Mech-Sense, Department of Hepatology and
Gastroenterology, and Department of Clinical Medicine, Aalborg University Hospital, Denmark; 3Department of Nuclear Medicine and
PET, Aarhus University Hospital, Denmark; 4Department of Clinical Medicine, Aarhus University, Denmark; 5Motilis Medica SA, Lausanne,
Switzerland; 6Department of Internal Medicine and Endocrinology, Aarhus University Hospital, Denmark; 7Steno Diabetes Center Aarhus,
Denmark; and 8Steno Diabetes Center Copenhagen, Denmark
Background/Aims
Patients with diabetes mellitus (DM) often suffer from gastrointestinal (GI) symptoms, but these correlate poorly to established
objective GI motility measures. Our aim is to perform a detailed evaluation of potential measures of gastric and small intestinal motility
in patients with DM type 1 and severe GI symptoms.
Methods
Twenty patients with DM and 20 healthy controls (HCs) were included. GI motility was examined with a 3-dimensional-Transit capsule,
while organ volumes were determined by CT scans.
Results
Patients with DM and HCs did not differ with regard to median gastric contraction frequency (DM: 3.0 contractions/minute
[interquartile range {IQR}, 2.9-3.0]; HCs: 2.9 [IQR, 2.8-3.1]; P = 0.725), amplitude of gastric contractions (DM: 9 mm [IQR, 8-11];
HCs: 11 mm (IQR, 9-12); P = 0.151) or fasting volume of the stomach wall (DM: 149 cm3 [IQR, 112-187]; HCs: 132 cm3 [IQR, 107-154];
P = 0.121). Median gastric emptying time was prolonged in patients (DM: 3.3 hours [IQR, 2.6-4.6]; HCs: 2.4 hours [IQR, 1.8-2.7];
P = 0.002). No difference was found in small intestinal transit time (DM: 5 hours [IQR, 3.7-5.6]; HCs: 4.8 hours [IQR, 3.9-6.0]; P =
0.883). However, patients with DM had significantly larger volume of the small intestinal wall (DM: 623 cm3 [IQR, 487-766]; HCs: 478
cm3 [IQR, 393-589]; P = 0.003). Among patients, 13 (68%) had small intestinal wall volume and 9 (50%) had gastric emptying time
above the upper 95% percentile of HCs.
Conclusion
In our study, gastric emptying time and volume of the small intestinal wall appeared to be the best objective measures in patients with
DM type 1 and symptoms and gastroenteropathy.
(J Neurogastroenterol Motil 2021;27:390-399)
Key Words
Diabetes mellitus; Diabetic neuropathies; Gastric emptying; Gastrointestinal motility; Organ size
Received: October 10, 2019 Revised: March 13, 2020 Accepted: December 19, 2020
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.
org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work
is properly cited.
*Correspondence: Mette W Klinge, MD, PhD
Department of Hepatology and Gastroenterology, Aarhus University Hospital, Palle Juul-Jensens Boulevard 99, C117, 8200 Aarhus
N, Denmark
Tel: +45-78450000, Fax: +45-78450000, E-mail: meteader@rm.dk
ⓒ 2021 The Korean Society of Neurogastroenterology and Motility
390
J Neurogastroenterol Motil, Vol. 27 No. 3 July, 2021
www.jnmjournal.org
�Objective Measures of Diabetic Gastroenteropathy
Introduction
Gastrointestinal (GI) symptoms are common in patients with
diabetes mellitus (DM).1 Their severity ranges from mild discomfort to recurrent vomiting, chronic nausea, abdominal pain,
diarrhea, or constipation.1,2 Severe GI symptoms are associated
with reduced quality of life and cause significant burden on the
healthcare system.3 Diabetic dysmotility can affect all segments of
the GI tract and specific symptoms do not correlate well with the
underlying pathophysiology.4 Autonomic neuropathy of the extrinsic
vagal fibers and the intrinsic enteric nervous system is considered
the primary cause of dysmotility in DM. Unfortunately, the autonomic and enteric nervous systems are difficult to evaluate in vivo.
Although tests of cardiovascular function are used as proxy for GI
neuropathy, results correlate poorly with GI symptoms.5,6
Patients with symptoms attributed to the upper GI tract will
usually undergo gastric emptying tests. The gold standard is gastric
emptying scintigraphy, in which a standardized radiolabeled meal is
tracked 30 minutes after ingestion and then every hour for at least
4 hours.7 Limitations of this method include: high cost, radiation
exposure, and poor correlation to symptoms.8,9 The wireless motility capsule (WMC) overcomes some of these limitations. It allows
minimally invasive, ambulatory, radiation-free, and pan-enteric
assessment of total and regional GI transit times.4,10-12 However,
symptoms of gastroparesis, such as nausea, vomiting, bloating, and
early satiety, show uncertain correlation to transit times found with
the WMC.11,12 It is therefore plausible that other parameters than
gastric emptying time and intestinal transit times should be considered as future diagnostic tests of GI dysfunction in DM.
With the Motilis 3-dimensional (3D)-Transit system (Motilis
Medica SA, Lausanne, Switzerland) an electromagnetic capsule
is followed as it traverses the GI tract. Like the WMC, the 3DTransit provides ambulatory assessment of gastric emptying, small
intestinal transit time, and colonic transit time.13-15 Because the 3DTransit detects the exact anatomical position and orientation of the
capsule at a sampling rate of 5-10 per second, the method allows
detailed description of contraction parameters. Recent development
of the software for post processing of data now provides information not only on the frequency, but also on the amplitude of gastric
contractions.
Earlier studies have found increased small intestinal volume in
diabetic rats.16-18 In humans, small intestinal volume can be measured from a low-dose CT scan or by MRI. In spite of this, gastric
and small intestinal volumes have received little attention as mea-
sures of diabetic enteropathy.
In the present explorative study, we aim at comparing (1) the
basic gastric contraction rate, (2) the amplitude of gastric contractions, (3) gastric emptying time, (4) volume of the stomach, (5)
small intestinal transit time, and (6) volume of the small intestine in
patients with DM and GI symptoms with those of healthy controls
(HCs).
Materials and Methods
Subjects
Between September 2015 and May 2019, 20 adult patients (11
males; mean age, 46.5 [standard deviation {SD}, 12.2]) with DM
type 1 and severe GI symptoms and 20 age and sex-matched HCs
(11 males; mean age, 45.0 [SD, 10.6]) were enrolled. The patients
had been referred to our tertiary clinic because of chronic GI symptoms attributed to long-term diabetes. No formal symptom-based
definition of diabetic gastroenteropathy exists, but all patients were
evaluated by an experienced specialized neurogastroenterologist
(M.W.K.) and screened for the present study if their symptoms
were considered severe enough to warrant further clinical evaluation. All patients had symptoms which could be attributed to the
upper GI tract but most also had symptoms usually originating
from the colon. All participants signed a written informed consent
before enrollment and all patients had a total score in Gastroparesis
Cardinal Symptom Index (GCSI) above 10.19,20
Exclusion criteria were: previous intestinal resection or other
major abdominal surgery, other diseases affecting GI function, and
severely reduced kidney or cardiac function. Due to radiation exposure incurred by CT scans, fertile women had to present a negative
pregnancy test before participating. All medications affecting the
GI function were paused at least 48 hours before each investigation. As a part of the standard diagnostic workup, all patients had
been evaluated with gastroscopy, standard blood and stool tests
for inflammatory bowel disease, celiac disease, lactose intolerance,
thyroid disease, malabsorption, and GI infection. Also, on clinical
indication, gastric emptying scintigraphy had been performed in 14
patients.
The study was conducted according to the Helsinki declaration
and European Community rules of good clinical practice. Approval
was obtained from the scientific ethics committee (reference: 1-1072-54-15) and the medical authorities (reference: 2016101143).
Vol. 27, No. 3 July, 2021 (390-399)
391
�Mette W Klinge, et al
Assessment of Diabetic Autonomic Neuropathy
Cardiac autonomic neuropathy (CAN) was assessed using the
handheld medical device Vagus (Medicus Engineering, Aarhus,
Denmark). CAN is routinely used as a surrogate marker of autonomic neuropathy in patients with diabetes. CAN was defined by
using gold standard cardiovascular reflex tests including the heart
response: to standing from a supine position, to deep breathing, and
to forceful expiration (normal cardiovascular reflex tests, no CAN;
one abnormal cardiovascular reflex test, early CAN; and autonomic
dysfunction, 2 or 3 abnormal cardiovascular reflex tests, manifest
CAN). Age-dependent cutoffs were used to define abnormal
results.21 Twenty-four hour blood pressure had been recorded on
clinical request. Attenuated decrease (dip) in the nocturnal blood
pressure of less than 10% was considered abnormal. Periphery neuropathy was assessed with monofilament according to international
guidelines.22 Furthermore, patients were asked about their sensation
of hypoglycemia. The answers were categorized as “preserved,”
“poor,” or “no sensation.”
Assessment of Gastric Contraction Frequency,
Amplitude, and Emptying Time
The 3D-Transit system is a wireless electromagnetic capsule
system used for detailed assessment of GI motility patterns and
transit times.13-15,23,24 After an overnight fast, the extracorporeal detector was mounted and the electromagnetic capsule (21.5 mm ×
8.3 mm, 1.6 g/cm3) ingested with a standardized meal (2 granola
bars: total 250 kcal; protein 3.8 g, fat 7.4 g, and carbohydrate 42 g;
and 300 mL of water). The detector belt was worn from ingestion until capsule expulsion from the body or end of battery power.
However, subjects under study were allowed to remove the detector
briefly when showering. They were not allowed to do heavy exercise, or stay closer than 40 cm to a computer during the study. Otherwise, all normal daily routines could be followed. Patients wearing
an insulin pump or blood glucose sensor were hospitalized and had
the device removed the day before starting the 3D-Transit examination. This precaution was taken to avoid interaction between the
3D-Transit system and the medical devices. Blood glucose was adjusted with manual insulin injections supervised by an experienced
endocrinologist (S.L.). The blood glucose was targeted to be within
the interval of 5-10 mmol/mL.
With 3D-Transit, the electromagnetic field emitted by the
capsule is registered by the detector and data is converted into coordinates (x, y, z, ɸ, and q) via an iterative algorithm. The x, y, and
z coordinates define spatial 3D position while ɸ, and q express the
392
angular position of the capsule to the detector. The lifetime of the
battery within the capsule is approximately 60 hours.
Recordings were analyzed in a custom developed software
to calculate regional transit times and contractility patterns.13 As
previously described in detail, gastric emptying and small intestinal
transit times were defined from region-specific contraction frequencies and the changes in position of the capsule on 2D plots.13 All
gastric contractions were manually marked to calculate frequency,
amplitude, and percentage of time with visible gastric contractions.
Analysis of gastric contractions was restricted to the first 6 hours
after the index meal because subjects were allowed to eat after this
period of time. All analyses were independently made by 2 investigators (M.W.K. and A.M.H.). In case of disagreement, the mean
value was used.
Volumes of the Stomach and Small Intestine
A low-dose high-resolution CT scan with intravenous contrast
(Visipaque 270 mg/mL; 2 mL/kg body weight with a maximum
of 180 mL) was performed after a minimum of 6 hours fasting for
food and a minimum of 2 hours for liquids. The scan field covered
an area from the left cardiac ventricle to the lower part of the anal
canal allowing assessment of abdominal organ volumes as well as
gas and fluid volumes within the gut. Data analysis was performed
in PMOD version 3.6 (PMOD Technologies, Zurich, Switzerland). Regions of interest were manually defined on each slice of
the CT scan. Volumes-of-interest were computed by fusing all the
regions of interest. Water/fluid was defined by Hounsfield unit < 30
for water and < –200 Hounsfield units for gas.25 The investigator
making all analyses (M.W.K.) was blinded to clinical category of
the test subjects. Part of the volume data will be presented elsewhere.26
Assessment of Gastrointestinal Symptoms
GI symptoms were assessed by the following 3 validated questionnaires: (1) Symptoms from the upper GI tract were quantified by the 20 item Patient Assessment of Upper Gastrointestinal
Symptom Severity Index (PAGI-SYM) questionnaire.20 The
PAGI-SYM questionnaires consists of 6 subscales: heartburn/regurgitation, nausea/vomiting, fullness/early satiety, bloating, upper
abdominal pain, and lower abdominal pain, each ranging from 0
(minimum) to 5 (maximum severity). (2) Symptoms of gastroparesis were rated by the GCSI, which is a 9-item score derivate from
PAGI-SYM.19 (3) The severity of constipation was quantified by
the 8 item Constipation Score System.27
Journal of Neurogastroenterology and Motility
�Objective Measures of Diabetic Gastroenteropathy
Table 1. Demographics and Clinical Characteristics of Patients and Healthy Controls Included in the Study
Demographics
Patients with DM type 1
Participants (M/F)
Age (yr)
Duration of GI symptoms (mo)
Duration of diabetes (yr)
BMI (kg/m2)
Glomerular filtration rate (mL/min/1.73 m2)
Urine albumine-creatinine ratio
Hemoglobin A1C (%)
Fast acting insulin (IU/kg per day)
Slow-acting insulin (IU/kg per day)
Insulin pump
Insulin sensor
Diabetic eye disease
Heart disease
Lack of noctunal blood pressure dip
Healthy controls
11/9
46.5 (12.2)
42.0 (30.7)
27.3 (12.7)
23.3 (22.1-26.9)
89.4 (25.6)
10.5 (5.0-33.0)
8.4 (1.8)
24.3 (8.9)
25.2 (14.9)
5 (25%)
6 (30%)
12 (60%)
2 (11%)
4 (20%)
P -values
11/9
45.0 (10.6)
1.000
0.675
26.3 (24.2-27.1)
97.3 (18.8)
0.083
0.304
DM, diabetes mellitus; M, male; F, female; GI, gastrointestinal; BMI, body mass index; IQR, interquartile range.
Data are presented as mean (SD), medians (interquartile range [IQR]), or n (%).
Table 2. Clinical Characteristics of the Questionnaires Patients and Healthy Controls Included in the Study
Clinical questionnaires
PAGI-SYM
GCSI
Sub-score
Bloating
Nausea/vomiting
Fulness/early satiety
CSS
Patients with DM type 1
Healthy controls
35.6 (22.9)
17.85 (9.27)
6 (4.5-7.5)
2 (0.0-4.0)
9 (4.5-14.5)
10 (4.9)
P -values
5.6 (6.6)
3.1 (3.8)
< 0.001
< 0.001
1 (0.0-2.5)
0 (0.0-0.0)
0.5 (0.0-2.0)
4.4 (3.2)
< 0.001
< 0.001
< 0.001
< 0.001
DM, diabetes mellitus; PAGI-SYM, patient assessment of upper gastrointestinal symptom severity index; GCSI, gastroparesis cardinal symptom index; CSS, constipation scoring system.
Data are presented as mean (SD) or medians (interquartile range [IQR]).
Statistical Methods
Three-dimensional Transit data were prepared for analysis by a
custom-made file in MATLAB version 2018b (MathWorks Inc,
Natick, MA, USA). Statistical analysis was performed in Stata
statistical software version 2013 (StataCorp LLC, College Station,
TX, USA). Graphic illustrations were performed using Prism 8
(GraphPad Software, San Diego, CA, USA). Parametric data were
compared with two-way unpaired Student’s t test with Welch correction for unequal variance. Nonparametric data were compared
by means of Wilcoxon Mann-Whitney U test. P < 0.05 was considered significant.
Results
Among 128 patients with DM referred to our unit because of
GI symptoms, 20 fulfilled the inclusion criteria and were willing to
participate. Reasons for non-participation were: concomitant disease
(n = 65), concomitant medication (n = 27), previous surgery (n = 4),
uncertain symptoms (n = 7), declined study participation (n = 8),
and non-compliance (n = 4). A few patients had more than one
reason for non-participation. Patients’ demography is displayed in
Table 1 and clinical characteristics obtained from the questionnaires
in Table 2. Results from the diabetes neuropathy test are shown in
Tables 1 and 3.
Vol. 27, No. 3 July, 2021 (390-399)
393
�Mette W Klinge, et al
Table 3. Diagnostic Tests From Each Patient
Small intestinal
Gastric emptying Gastric wall volume
wall volume > 95%
Duration of
> 95% percentile > 95% percentile
DM (yr)
percentile of
of healthy
of healthy
healthy
5
11
12
15
15
18
19
21
22
28
28
32
33
34
36
37
40
45
45
49
No
Yes
Yes
Yes
No
No
No
Yes
No
Yes
Yes
No
Yes
Yes
No
Yes
No
No
9 (50%)
Yes
No
No
Yes
No
No
No
Yes
Yes
No
No
No
No
No
Yes
Yes
No
Yes
No
7 (37%)
Yes
No
Yes
Yes
Yes
No
Yes
Yes
Yes
Yes
No
Yes
No
No
Yes
Yes
Yes
Yes
No
13 (68%)
Prolonged
gastric emptying
(scintigraphy)
Cardiac autonomic
neuropathy score
≥2
Periphery
neuropathy
Sensation of
hypoglycemia
Normal
Prolonged
Normal
Normal
Prolonged
Normal
Normal
Normal
Normal
Normal
Normal
Prolonged
Prolonged
Normal
4 (29%)
No
Yes
No
No
No
No
No
Yes
Yes
No
No
No
No
No
Yes
No
Yes
5 (29%)
Yes
No
No
No
No
No
No
Yes
No
Yes
No
No
Yes
Yes
Yes
No
Yes
7 (41%)
No
Poor
Yes
Yes
Yes
Yes
Yes
No
Poor
Yes
No
Poor
Yes
Poor
Yes
Yes
No
8 (47%)
DM, diabetes mellitus.
Normal values are highlighted in gray. “-” marks missing value. All patients with prolonged gastric emptying at scintigraphy also had abnormally large small intestine.
A
180
160
160
140
140
120
120
100
100
80
60
Duodenal
passage
80
Duodenal
passage
60
40
40
20
Corpus
Corpus
20
0
0
20
20
Antrum
Antrum
Length in y-direction (mm)
Length in y-direction (mm)
B
Fundus
Fundus
40
40
0
50
100
150
0
Length in x-direction (mm)
50
100
150
Length in x-direction (mm)
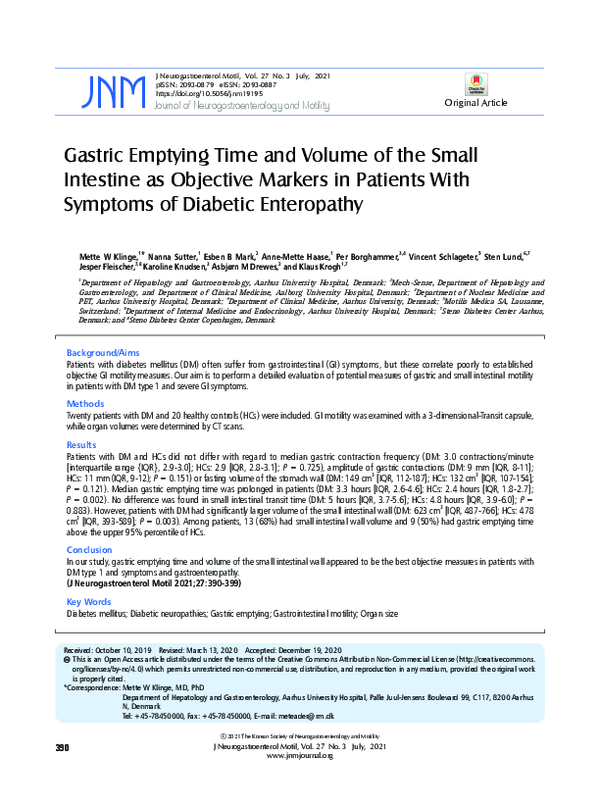
Figure 1. Intragastric movements of the 3-dimensional Transit electromagnetic capsule. Recordings from a healthy volunteer (A) and a patient
with diabetes (B). Red dots show every 30 minute intervals position in the stomach.
394
Journal of Neurogastroenterology and Motility
�Objective Measures of Diabetic Gastroenteropathy
Gastric Contractions
Gastric Emptying Time
Median time with recognizable contractions of the stomach
was 92% (interquartile range [IQR], 79-94) in patients with
DM and 92% (IQR, 78-97) in HCs (P = 0.501). The median
frequency of gastric contractions was 3.0 contractions per minute
(CPM) (IQR, 2.9-3.0) in patients with DM and 2.9 CPM (IQR,
2.8-3.1) in HCs (P = 0.725). The median amplitude of capsule
rotation was 27 degrees (IQR, 19-41) in patients with DM and 31
degrees (IQR, 23-42) in HCs (P = 0.736). The median amplitude of change in position of the capsule was 9 mm (IQR, 8-11) in
patients with DM and 11 mm (IQR, 9-12) in HCs (P = 0.151).
In 2 (10%) patients with DM the amplitude (position) of gastric
contractions was below the lower 5% limit of HCs. Examples of intragastric movements in a patient with DM and in a HC are shown
in Figure 1.
Median gastric emptying time was 3.3 hours (IQR, 2.6-4.6)
in patients with DM and 2.4 hours (IQR, 1.8-2.7) in HCs (P =
0.002). In 9 (50%) of 18 patients, gastric emptying time was beyond the upper 95% limit of the HC group (Table 3).
Gastric Volume
There was no difference in gastric wall volume between patients
with DM and HCs (Fig. 2 and Table 4). In 7 of 19 patients (37%),
the volume of the gastric wall was above the upper 95% percentile
of HCs. The amount of fluid in the stomach and the total volume
of the stomach including both the wall and luminal content did not
differ significantly between the 2 groups (Table 4).
Small Intestinal Transit Time
Median small intestinal transit time was 5.0 hours (IQR, 3.75.6) in patients with DM and 4.8 hours (IQR, 3.9-6.0) in HCs
(P = 0.883). In 2 of 19 patients (11%), small intestinal transit time
was above the upper 95% limit of the HC group.
Volume of the stomach
400
B
Volume of the small intestine
1000
800
300
3
Volume (cm )
3
Volume (cm )
A
200
100
600
400
200
0
0
HCs
DM
HCs
DM
Volume of the Small Intestine
As illustrated in Figure 2 and seen in Table 4, patients with
DM had significantly larger volume of the small intestinal wall.
In 13 of 19 patients (68%), the small intestinal wall volume was
above the upper 95% limit of that in HCs (Table 3). The total small
intestinal volume including both the wall and luminal content was
likewise significantly larger in patients with diabetes. DM patients
had more fluid in the small intestine compared to HCs, but the difference did not reach statistical significance (Table 4).
Figure 2. Volumes of the gastric (A) and small intestinal walls (B) as-
sesses with CT scans. The horizontal line shows the median. Diabetes
patients had a significantly larger volume of the small intestinal wall
(P = 0.003) but not of the stomach (P = 0.121). HCs, healthy controls; DM, patients with diabetes mellitus.
Questionnaires
In all questionnaires, patients with DM scored significantly
higher than HCs (Table 2). Within the group of patients with DM,
Table 4. Gastric and Small Intestinal Volumes
Gastrointestinal volumes (cm3)
Volume of the stomach including luminal content
Volume of the gastric wall
Volume of fluid in the stomach
Volume of the small intestine including gas and luminal content
Volume of the small intestine wall
Volume of fluid in the small intestine
Volume of gas in the small intestine
Healthy controls
Patients with diabetes
P -value
182 (151-246)
131 (107-154)
31 (17-56)
713 (639-899)
478 (393-589)
209 (165-236)
95 (40-150)
162 (138-193)
149 (112-187)
37 (24-84)
927 (829-1051)
623 (487-766)
227 (191-288)
83 (56-139)
0.078
0.121
0.293
0.002
0.003
0.082
0.872
Among patients with diabetes, 7 (37%) had a total small intestinal volume and 4 (21%) had a total gastric volume above the upper 95% percentile of healthy controls.
Data are presented as medians (interquartile range [IQR]).
Vol. 27, No. 3 July, 2021 (390-399)
395
�Mette W Klinge, et al
there was no association between any of the scores and the objective
measures described above.
Discussion
Symptoms of gastric and small intestinal dysfunction are common among patients with DM. In the present explorative study,
we found no differences in basic gastric contraction frequency or
the amplitude of gastric contractions when comparing patients with
DM and HCs. Gastric emptying time, but not small intestinal
transit time, was longer in patients with DM than in HCs. The
volume of the small intestine was significantly larger in patients than
in HCs. Hence, the main implications of our study are that gastric
emptying time and small intestinal wall volume seem to be the most
sensitive objective measures in patients with DM type 1 and symptoms of dysmotility within the upper GI tract.
Diabetic Enteropathy
Because of the non-specific symptoms, diagnosis of diabetic
gastroenteropathy is difficult. The pathophysiology behind diabetic
gastroenteropathy is incompletely understood. Enteric and vagal
neuropathy, depletion of interstitial cells of Cajal, reduced function
of smooth muscle cells, and hyperglycemia may all contribute to
gastroenteropathy.28-32 The GI tract is innervated by sympathetic,
parasympathetic, and enteric nerves. Animal studies have found
morphological changes in the vagal nerve and segmental demyelination as well as axonal degeneration of the myenteric and submucosal plexus.29-31 Products of glycation may cause neural damage and
reduce neuronal nitric oxide synthase.33 Since neuronal nitric oxide
synthase is reduced in early stage diabetic rats while cholinergic
nerves are affected later, it has been suggested that inhibitory neurons are affected by DM before excitatory.34 Both factors increase
the risk of GI complications. Diabetic gastroparesis is usually diagnosed after 10 years of disease.35 In our study population, the mean
duration of diabetes was more than 20 years and hemoglobin A1C
was relatively high.
Standard Tests of Autonomic and Peripheral
Neuropathy
Earlier studies have shown that autonomic, but not peripheral
somatic neuropathy correlates with prolonged gastric emptying.8,36
Hence, CAN is commonly used as a surrogate for enteric neuropathy in patients with DM. CAN is easily assessed with 3 different
cardiovascular reflex tests sometimes in combination with a 24-hour
blood pressure measurement, but unfortunately the correlation with
396
GI symptoms remains poor.5,8 In the present study, 29% patients
with symptoms of diabetic enteropathy had manifest CAN. Bharucha et al37 showed in 78 patients with DM type 1, that decreased
heart rate variability in the deep breathing test and not the response
to standing or the Valsalva maneuver, correlated with prolonged
gastric emptying. Detailed heartrate variability analysis was not part
of the primary endpoint and the possible association to prolonged
gastric emptying will be investigated in a future study.
Gastric Contractions
Comparing the basic gastric contraction frequency, the amplitude of contractions and the time with identifiable contractions, we
found no difference between patients with DM and HCs. Previous
studies of the myoelectrical activity assessed with electrogastrography have shown discoordinated activity in patients with DM.
This contrasts our results, but electrical impulses from the surface
of the body may not entirely correlate with gastric contractions.38
Also, in contrast to our data, a study of 113 subjects evaluated with
the WMC found a decreased number of contractions per hour in
patients with DM. The reduced number of contractions was associated with prolonged gastric emptying.39 The difference to our
study may be due to a type II error caused by the smaller number of
patients in our study.
We used the electromagnetic 3D-Transit system to describe
gastric motility in detail. The 3D-Transit capsule is very sensitive as
even millimeters of displacements in its position or a few degrees of
rotation will be registered. Capsule location in the stomach fundus
may change the contraction frequency. However, brief stays in the
fundus were included in the total gastric contraction analysis, as
the stays were short lasting and estimated without influence of the
contractility pattern. Theoretically, changes in position are more
sensitive than pressure changes, especially in large hollow organs.
Hence, we expected that the 3D-Transit would add new and valuable information about gastric contractions not available with other
methods. However, median values for the frequency of gastric contractions were almost identical among patients with DM and HCs.
The number of subjects included in the present study was too small
to draw definite conclusions, but our data may suggest the basic
frequency of myoelectrical activity generated by the smooth muscle
cells was intact. The amplitude of movements of the capsule was
lower in patients with DM than in HCs, but the difference did not
reach statistical significance, which may be related to the relatively
small sample. Previous studies have shown that DM causes impaired accommodation of the stomach, which may contribute to GI
symptoms even if gastric contractions remain unaltered.40
Journal of Neurogastroenterology and Motility
�Objective Measures of Diabetic Gastroenteropathy
Gastrointestinal Transit Times
Patients with diabetic enteropathy have pan-enteric dysmotility and assessment of regional GI transit times is part of the clinical
evaluation at many centers. The commonly used WMC is a radiation-free, ambulatory and minimal invasive method that has been
validated against scintigraphy and the 13C breath test.41 The 3DTransit system is not yet as well established as the WMC. However, gastric emptying and small intestinal transit time obtained by
magnet tracking have been tested together with endoscopic video
capsule (PillCam) and gastric emptying scintigraphy.24,42 The electromagnetic capsule for 3D-Transit is smaller (21.5 mm × 8.3 mm)
than the WMC (26.8 mm × 11.7 mm) but normative data for
regional transit times with the 2 methods are very similar. With the
WMC, gastric emptying was more affected in DM than the small
intestinal transit time.43 Thus, the previous studies with the WMC
support the findings of the present study.
Volume of the Small Intestine
In previous studies, rats with DM had hyperplasia of the
small intestine.16-18 This is probably mainly due to mucosal hypertrophy.44,45 In our study, patients with diabetes had a 34% increase
of small intestinal wall volume compared to HCs. We found it
noteworthy that 68% of patients with DM and symptoms of upper
GI dysmotility had volumes of the small intestinal wall above the
upper 95% limit of the HCs. Thus, assessment of small intestinal
wall volume holds promise as a more sensitive marker of diabetic
enteropathy than other existing methods. Unfortunately, assessment
of intestinal volumes is time consuming and new techniques for this
are warranted.
Limitations
The present study is an explorative study including 40 study
participants in total. The small study size increases the risk of type
II errors. Thus, a larger study is needed to confirm our findings.
Furthermore, in future studies a control group of patients recently
diagnosed with DM could be included. The patients included
in the present study were selected from the much larger group of
patients referred to our unit for assessment of diabetic enteropathy.
This may have caused selection bias and therefore affect the external
validity of the study findings. The main reasons for excluding patients from the study were use of medication influencing gut motility and nephropathy.
Gastric emptying scintigraphy was not part of our study protocol, but 14 patients had the procedure performed on clinical indica-
tions. A direct comparison between 3D-Transit or volume assessed
by CT and gastric emptying scintigraphy would be highly relevant,
as the latter is considered the gold standard test for gastric emptying. Such comparison was however beyond the scope of the present
study. There was discrepancy between results from gastric emptying scintigraphy and the 3D-Transit capsule. Scintigraphy was not
performed on the same days as the 3D-Transit study. Symptoms
of diabetic enteropathy may fluctuate and there is intersubjective
variation in objective methods used. Whether this is the cause of the
discrepancy found or 3D-Transit is more sensitive than gastric emptying scintigraphy needs to be addressed in larger studies. Finally,
all patients in the present study had DM type 1 and results may not
be directly applicable to patients with DM type 2.
In conclusion, in this present study the frequency of gastric
contractions was unaffected by DM. Among the parameters studied, gastric emptying time and volume of the small intestine seem to
provide the most sensitive objective measures in patients with DM
type 1 and symptoms attributed to the upper GI tract.
Financial support: This article was financial supported by; The
Novo Nordisk Foundation (13159), The Lundbeck Foundation
(R230-2016-2306), Højmosegaard Legatet, The A.P. Møller
Foundation for the Advancement of Medical Science, Holger Rabitz og Hustru Doris Mary født Phillips Legat, Loge nr 73, Svend
Fældings Humanitære Fond, Torben og Alice Frimodts Fond, The
Foundation for Medical Students University of Copenhagen and
Wilhelm Frank og Angelina Franks Mindelegat.
Conflicts of interest: Vincent Schlageter is co-owner of Motilis
Medica SA, he took part in the technical terms of improving the
software for gastric analysis. Jesper Fleischer is the co-inventor of
Vagus. Mette W Klinge, Nanna Sutter, Esben B Mark, AnneMette Haase, Per Borghammer, Sten Lund, Karoline Knudsen,
Asbjørn M Drewes, and Klaus Krogh have no competing interests.
Author contributions: Mette W Klinge: contribution to the
concept and design, analyzing of data, interpretation of data, and
drafting the article; Nanna Sutter: practical work during study examinations and data analysis; Esben B Mark: data analysis, critical
reviewing for important intellectual content; Anne-Mette Haase:
contribution to the concept and design, data analysis, and critical
reviewing for important intellectual content; Per Borghammer and
Sten Lund: contribution to the concept and design, interpretation
of data, and critical reviewing for important intellectual content;
Vincent Schlageter: data analysis, interpretation of data, and critical
reviewing for important intellectual content; Jesper Fleischer: in-
Vol. 27, No. 3 July, 2021 (390-399)
397
�Mette W Klinge, et al
terpretation of data and critical reviewing for important intellectual
content; Karoline Knudsen: data analysis and critical reviewing for
important intellectual content; Asbjørn M Drewes: interpretation
of data and critical reviewing for important intellectual content; and
Klaus Krogh: contribution to the concept and design, interpretation
of data, drafting the article, and critical reviewing for important intellectual content. All authors final approved the manuscript before
submission.
References
1. Du YT, Rayner CK, Jones KL, Talley NJ, Horowitz M. Gastrointestinal
symptoms in diabetes: prevalence, assessment, pathogenesis, and management. Diabetes Care 2018;41:627-637.
2. Bytzer P, Talley NJ, Leemon M, Young LJ, Jones MP, Horowitz M.
Prevalence of gastrointestinal symptoms associated with diabetes mellitus: a population-based survey of 15.000 adults. Arch Intern Med
2001;161:1989-1996.
3. DiBaise JK, Patel N, Noelting J, Dueck AC, Roarke M, Crowell MD.
The relationship among gastroparetic symptoms, quality of life, and gastric emptying in patients referred for gastric emptying testing. Neurogastroenterol Motil 2016;28:234-242.
4. Farmer AD, Pedersen AG, Brock B, et al. Type 1 diabetic patients with
peripheral neuropathy have pan-enteric prolongation of gastrointestinal
transit times and an altered caecal pH profile. Diabetologia 2017;60:709718.
5. Clouse RE, Lustman PJ. Gastrointestinal symptoms in diabetic patients:
lack of association with neuropathy. Am J Gastroenterol 1989;84:868872.
6. Punkkinen J, Färkkilä M, Mätzke S, et al. Upper abdominal symptoms
in patients with type 1 diabetes: unrelated to impairment in gastric emptying caused by autonomic neuropathy. Diabet Med 2008;25:570-577.
7. Abell TL, Camilleri M, Donohoe K, et al. Consensus recommendations
for gastric emptying scintigraphy: a joint report of the American neurogastroenterology and motility society and the society of nuclear medicine.
Am J Gastroenterol 2008;103:753-763.
8. Darwiche G, Almér LO, Björgell O, Cederholm C, Nilsson P. Delayed
gastric emptying rate in type 1 diabetics with cardiac autonomic neuropathy. J Diabetes Complications 2001;15:128-134.
9. Vijayvargiya P, Jameie-Oskooei S, Camilleri M, Chedid V, Erwin PJ,
Murad MH. Association between delayed gastric emptying and upper
gastrointestinal symptoms: a systematic review and meta-analysis. Gut
2019;68:804-813.
10. Wang YT, Mohammed SD, Farmer AD, et al. Regional gastrointestinal
transit and pH studied in 215 healthy volunteers using the wireless motility capsule: influence of age, gender, study country and testing protocol.
Aliment Pharmacol Ther 2015;42:761-772.
11. Hasler WL, May KP, Wilson LA, et al. Relating gastric scintigraphy
and symptoms to motility capsule transit and pressure findings in suspected gastroparesis. Neurogastroenterol Motil 2018;30:e13196.
398
12. Arora Z, Parungao JM, Lopez R, Heinlein C, Santisi J, Birgisson S.
Clinical utility of wireless motility capsule in patients with suspected multiregional gastrointestinal dysmotility. Dig Dis Sci 2015;60:1350-1357.
13. Haase AM, Gregersen T, Schlageter V, et al. Pilot study trialling a new
ambulatory method for the clinical assessment of regional gastrointestinal
transit using multiple electromagnetic capsules. Neurogastroenterol Motil
2014;26:1783-1791.
14. Fynne L, Worsøe J, Gregersen T, Schlageter V, Laurberg S, Krogh K.
Gastrointestinal transit in patients with systemic sclerosis. Scand J Gastroenterol 2011;46:1187-1193.
15. Gregersen T, Haase AM, Schlageter V, Gronbaek H, Krogh K. Regional gastrointestinal transit times in patients with carcinoid diarrhea:
assessment with the novel 3D-transit system. J Neurogastroenterol Motil
2015;21:423-432.
16. Schedl HP, Schwartz J, Wilson HD. Increased intestinal growth in the
streptozotocin-diabetic rat occurs prior to changes in hormone secretion.
Digestion 1988;39:137-143.
17. Zhao J, Yang J, Gregersen H. Biomechanical and morphometric intestinal remodelling during experimental diabetes in rats. Diabetologia
2003;46:1688-1697.
18. Sha H, Zhao JB, Zhang ZY, et al. Effect of kaiyu qingwei jianji on the
morphometry and residual strain distribution of small intestine in experimental diabetic rats. World J Gastroenterol 2006;12:7149-7154.
19. Revicki DA, Rentz AM, Dubois D, et al. Gastroparesis cardinal
symptom index (GCSI): development and validation of a patient reported assessment of severity of gastroparesis symptoms. Qual Life Res
2004;13:833-844.
20. Rentz AM, Kahrilas P, Stanghellini V, et al. Development and psychometric evaluation of the patient assessment of upper gastrointestinal symptom severity index (PAGI-SYM) in patients with upper gastrointestinal
disorders. Qual Life Res 2004;13:1737-1749.
21. Andersen ST, Witte DR, Fleischer J, et al. Risk factors for the presence
and progression of cardiovascular autonomic neuropathy in type 2 diabetes: addition-Denmark. Diabetes Care 2018;41:2586-2594.
22. Apelqvist J, Bakker K, van Houtum WH, Scapher NC. Practical guidelines on the management and prevention of the diabetic foot: based upon
the international consensus on the diabetic foot (2007) prepared by the
international working group on the diabetic foot. Diabetes Metab Res
Rev 2008;24(suppl 1):S181-S187.
23. Haase AM, Fallet S, Otto M, Scott SM, Schlageter V, Krogh K. Gastrointestinal motility during sleep assessed by tracking of telemetric capsules
combined with polysomnography - a pilot study. Clin Exp Gastroenterol
2015;8:327-332.
24. Knudsen K, Haase AM, Fedorova TD, et al. Gastrointestinal transit
time in parkinson’s disease using a magnetic tracking system. J Parkinson
Dis 2017;7:471-479.
25. Fedorova TD, Seidelin LB, Knudsen K, et al. Decreased intestinal acetylcholinesterase in early parkinson disease: an 11C-donepezil PET study.
Neurology 2017;88:775-781.
26. Klinge MW, Borghammer P, Lund S, et al. Enteric cholinergic neuropathy in patients with diabetes: non-invasive assessment with positron emission tomography. Neurogastroenterol Motil 2020;32:e13731.
Journal of Neurogastroenterology and Motility
�Objective Measures of Diabetic Gastroenteropathy
27. Agachan F, Chen T, Pfeifer J, Reissman P, Wexner SD. A constipation
scoring system to simplify evaluation and management of constipated
patients. Dis Colon Rectum 1996;39:681-685.
28. Horváth VJ, Vittal H, Lörincz A, et al. Reduced stem cell factor links
smooth myopathy and loss of interstitial cells of cajal in murine diabetic
gastroparesis. Gastroenterology 2006;130:759-770.
29. Guo C, Quobatari A, Shangguan Y, Hong S, Wiley JW. Diabetic autonomic neuropathy: evidence for apoptosis in situ in the rat. Neurogastroenterol Motil 2004;16:335-345.
30. Guy RJ, Dawson JL, Garrett JR, et al. Diabetic gastroparesis from autonomic neuropathy: surgical considerations and changes in vagus nerve
morphology. J Neurol Neurosurg Psychiatry 1984;47:686-691.
31. Tay SS, Wong WC. Short and long-term induced effects of streptozotocin induced diabetes on the dorsal motor nucleus of the vagus nerve in
the rat. Acta Anat 1994;150:274-281.
32. Frokjaer JB, Andersen SD, Ejskjaer N, Funch-jensen P, Drewes AM,
Gregersen H. Impaired contractility and remodeling of the upper
gastrointestinal tract in diabetes mellitus type-1. World J Gastroenterol
2007;13:4881-4890.
33. Bulc M, Palus K, Dąbrowski M, Całka J. Hyperglycaemia-induced
downregulation in expression of nNOS intramural neurons of the small
intestine in the pig. Int J Mol Sci 2019;20:1681.
34. Demedts I, Masaoka T, Kindt S, et al. Gastrointestinal motility changes
and myenteric plexus alterations in spontaneously diabetic biobreeding
rats. J Neurogastroenterol Motil 2013;19:161-170.
35. Aleppo G, Calhoun P, Foster NC, et al. Reported gastroparesis in adults
with type 1 diabetes (T1D) from the T1D exchange clinic registry. J Diabetes Complications 2017;31:1669-1673.
36. Merio R, Festa A, Bergmann H, et al. Slow gastric emptying in type 1
diabetes: relation to autonomic and peripheral neuropathy, blood glucose
and glycemic control. Diabetes Care 1997;20:419-423.
37. Bharucha AE, Batey-Schaefer B, Cleary PA, et al. Delayed gastric
emptying is associated with early and long-term hyperglycemia in type 1
diabetes mellitus. Gastroenterology 2015;149:330-339.
38. Yin J, Chen JDZ. Electrogastrography: methodology, validation and applications. J Neurogastroenterol Motil 2013;19:5-17.
39. Kloetzer L, Chey WD, McCallum RW, et al. Motility of the antroduodenum in healthy and gastroparetics characterized by wireless motility
capsule. Neurogastroenterol Motil 2010;22:527-533, e117.
40. Chedid V, Brandler J, Vijayvargiya P, Park SY, Szarka LA, Camilleri M.
Characterization of upper gastrointestinal symptoms, gastric motor functions, and associations in patients with diabetes at a referral center. Am J
Gastroenterol 2019;114:143-154.
41. Hasler WL. The use of SmartPill for gastric monitoring. Expert Rev
Gastroenterol Hepatol 2014;8:587-600.
42. Worsøe J, Fynne L, Gregersen T, et al. Gastric transit and small intestinal
transit time and motility assessed by a magnet tracking system. BMC
Gastroenterol 2011;11:145.
43. Rouphael C, Arora Z, Thota PN, et al. Role of wireless motility capsule
in the assessment and management of gastrointestinal dysmotility in patients with diabetes mellitus. Neurogastroenterol Motil 2017;29:e13087.
44. Fischer KD, Dhanvantari S, Drucker DJ, Brubaker PL. Intestinal
growth is associated with elevated levels of glucagon-like peptide 2 in diabetic rats. Am J Physiol 1997;273:E815-E820.
45. Zhao M, Liao D, Zhao J. Diabetes-induced mechanophysiological
changes in the small intestine and colon. World J Diabetes 2017;8:249269.
Vol. 27, No. 3 July, 2021 (390-399)
399
�
 Vincent Schlageter
Vincent Schlageter