teamwork and communication
Using SBAR to Communicate
Falls Risk and Management in
Inter-professional Rehabilitation
Teams
Angie Andreoli, Carol Fancott, Karima Velji, G. Ross Baker, Sherra Solway, Elaine Aimone and Gaétan Tardif
Abstract
This study implemented and evaluated the adapted SituationBackground-Assessment-Recommendation (SBAR) tool for
use on two inter-professional rehabilitation teams for the
specific priority issue of falls prevention and management.
SBAR has been widely studied in the literature, but rarely
in the context of rehabilitation and beyond nurse-physician
communication. In phase one, the adapted SBAR tool was
implemented on two teams with a high falls incidence over
a six-month period. In phase two, process and outcome
evaluations were conducted in a pre-post design comparing
the impact of the intervention with changes in the rest of
the hospital, including the perceptions of safety culture (as
measured by the Hospital Survey on Patient Safety Culture);
effective team processes, using the Team Orientation Scale;
and safety reporting, including falls incidence, severity and
near misses. This study suggests that the adapted SBAR tool
was widely and effectively used by inter-professional rehabilitation teams as part of a broader program of safety activities.
Near-miss and severity of falls incidence trended downward
but were inconclusive, likely due to a short time frame as well
as the nature of rehabilitation, which pushes patients to the
limit of their abilities. While SBAR was used in the context
of falls prevention and management, it was also utilized it in
a variety of other clinical and non-clinical situations such as
transitions in care, as a debriefing tool and for conflict resolu-
94
Healthcare Quarterly Vol.13 Special Issue September 2010
tion. Staff found the tool useful in helping to communicate
relevant and succinct information, and to “close the loop” by
providing recommendations and accountabilities for action.
Suggestions are provided to other organizations considering adopting the SBAR tool within their clinical settings,
including the use of an implementation tool kit and video
simulation for enhanced uptake.
Background
The physical, psychological, social and economic consequences
of falls and falls-related injuries have been well documented in
the literature. Each year in Canada, approximately one third
of healthy, community-dwelling older adults experience a fall
(Registered Nurses Association of Ontario [RNAO] 2007). Falls
in hospitals are almost three times this rate and account for up
to 84% of all in-patient incidents (Halfon et al. 2001). There
is compelling evidence, however, that falls can be prevented
through timely risk detection and appropriate management.
Numerous guidelines have emerged over the past decade
outlining best practice for falls risk prevention and management both within healthcare settings and in the community
(American Geriatrics Society, British Geriatrics Society and
American Academy of Orthopaedic Surgeons Panel on Falls
Prevention 2001; RNAO 2007). Inherent within these guidelines is the need for strong inter-professional team collabora-
�Angie Andreoli et al. Using SBAR to Communicate Falls Risk and Management in Inter-professional Rehabilitation Teams
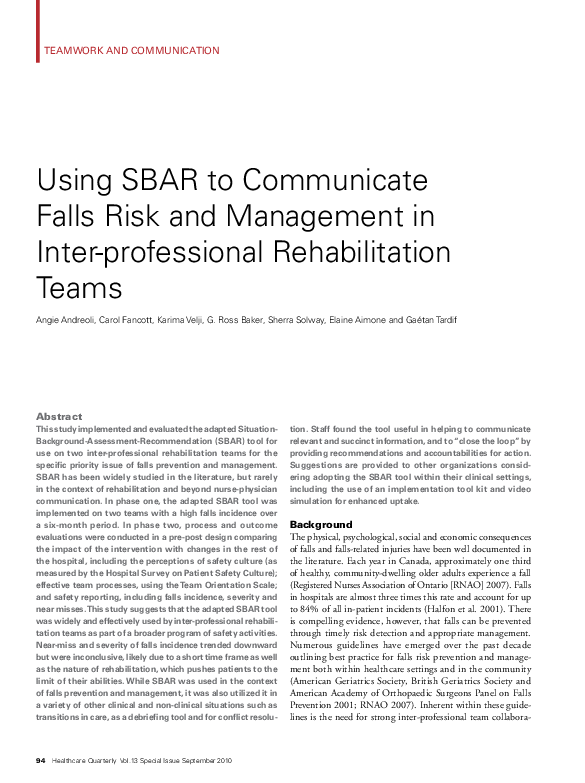
tion and communication. Communication
Figure 1. The adapted SBAR tool
breakdown has long been cited as the leading
cause of inadvertent patient harm, including
falls (Joint Commission on Accreditation
of Health Care Organizations 2004). All
too frequently, however, communication is
context or personality dependent and influenced by a myriad of factors including gender,
culture, profession and structured hierarchies
within healthcare (Leonard et al. 2004).
The Toronto Rehabilitation Institute
(Toronto Rehab), a large academic rehabilitation and complex continuing care hospital, has
embarked upon a novel patient safety strategy
to improve team communication. In a pilot
study, we adapted and implemented a structured communication tool – the SituationBackground-Assessment-Recommendation
(SBAR) process – for use in a rehabilitation
setting, with promising results (Boaro et al.
2010; Velji et al. 2008; see Figure 1 for the
adapted SBAR tool). The SBAR tool is a situational briefing model that provides appropriate
assertion, critical language and education to a
safety issue (Leonard et al. 2004). While many
organizations have implemented the SBAR
tool, there is little evidence regarding its effectiveness beyond the acute care environment
and nurse-physician communication. The
pilot study offered preliminary insights into
how SBAR may be used and evaluated within
an inter-professional rehabilitation team.
This current study builds upon our previous
work in three ways: it implements SBAR on
Source: Toronto Rehabilitation Institute.
two rehabilitation units with high falls rates;
it focuses team communication around the
high-priority issue of falls prevention and
management; and evaluates processes and outcomes specific to chosen for this study. Both units are similar in size, admit similar
patient safety culture, team communication, and falls incidence patient populations (older adults with multiple co-morbidities)
and have similar lengths of stay (ranging from 35 to 40 days).
and severity.
They are also comparable in terms of falls incidence. In the two
years leading up to the study, falls on these units constituted
Methods
This project had two phases: in phase one we implemented the 43% of all reported falls in our organization (excluding longadapted SBAR tool and in phase two we evaluated its processes term care).
and outcomes.
Participants
Phase One: Implementation of the Adapted
SBAR Tool
Study Teams
The geriatric and the musculoskeletal rehabilitation units were
Clinical and non-clinical staff members and leaders of the
geriatric rehabilitation (50/55) and musculoskeletal rehabilitation (35/50) units participated in this study. Participants
included health professionals who deliver direct patient care
(e.g., health disciplines, nurses and physicians), as well as support
Healthcare Quarterly Vol.13 Special Issue September 2010 95
�Using SBAR to Communicate Falls Risk and Management in Inter-professional Rehabilitation Teams Angie Andreoli et al.
staff who have a critical
role within the unit (e.g.,
porters, housekeeping and
volunteers). In both study
groups, all health disciplines, physicians and
unit leaders participated.
Education Sessions
Table 1. Study teams pre- and post-intervention
Pre-intervention
(%)
Postintervention (%)
Overall Perceptions of Safety
38
59
20
4.43
Frequency of Events Reported
45
52
8
1.29
Manager Expectations
Promoting Safety
77
82
5
1.11
Safety Dimension
Change
(%)*
Critical Ratio
Test (z >1.96)*
The implementation
of the SBAR process
Organizational Learning
72
85
14
3.04
occurred over a six-month
Teamwork within Units
73
82
9
2.23
period. A series of three
education workshops
Communication Openness
42
54
13
2.33
(a total of four hours)
Feedback and Communication
52
67
15
2.70
introduced staff to key
about
Error
elements of patient safety
including communication
Non-punitive Response to Error
39
51
13
2.31
breakdown in healthcare,
Staffing
40
56
16
3.49
a systems approach to
safety culture, openness
Management Support for
71
78
8
1.57
to reporting incidents
Patient Safety
and near misses and
Teamwork across Hospital Units
63
79
17
3.82
the use SBAR to facilitate communication.
Handoffs and Transitions
30
57
28
5.76
Role-playing using real*Legend: Those results presented in shaded grey boxes are considered clinically improved (≥5%); in blue boxes are considered statistically improved
life case examples related
(z >1.96); and in yellow boxes represent no change.
to falls risk assessment,
prevention and management was used to demonstrate how SBAR may be
Outcomes were measured using a pre-post test design, and data
implemented in clinical situations. These scenarios provided from the study teams are presented in aggregate form. The
participants with powerful feedback in learning how to apply process evaluation involved a multimodal approach that aimed
the tool.
to better understand the context and uptake of SBAR on the
two inter-professional teams.
Sustaining the Use of SBAR on the Units
Our previous work supported using local champions to reinforce
the use of SBAR during the implementation phase and beyond.
We also used a series of reminder tools including pocket cards,
posters, telephone prompts and educational binders that were
located strategically throughout the units. A member of the
research team or SBAR champion also attended weekly team
rounds as a way to further reinforce the use of SBAR, and to
understand the situations in which SBAR was being used (or
not), with whom and in what context.
Phase Two: Outcome and Process Evaluation of the
Effectiveness of the Adapted SBAR Tool
The three main outcome measures of this study examined staff
perceptions of patient safety culture, team effectiveness and
falls incidence, including fall severity and near-miss reporting.
96
Healthcare Quarterly Vol.13 Special Issue September 2010
Staff Perceptions of Safety Culture
Staff perceptions of patient safety culture were measured using
the Hospital Survey on Patient Safety Culture (HSOPSC; Westat
et al. 2004). The 43-item survey can be used to track changes
in patient safety culture over time, as well as to evaluate the
impact of patient safety interventions at both the organization
and unit levels. The survey consists of 12 patient safety domains
and has been found to be valid and reliable. All Toronto Rehab
staff (n = 1,700) were sent the survey prior to the implementation of SBAR and approximately 12 months later. Response
rates pre- and post-intervention were 31% (n = 520) and 33%
(n = 569), respectively. The study teams had a response rate of
87% (n = 74) pre-intervention and 69% (n = 59) post-intervention. Surveys were analyzed using the “5% rule of thumb” as
suggested by the survey authors; that is, results must be at least
�Angie Andreoli et al. Using SBAR to Communicate Falls Risk and Management in Inter-professional Rehabilitation Teams
Table 2. Study teams compared with the rest of the hospital pre- and post-intervention
Pre-intervention*
Post-intervention*
Study
Units
(%)
Rest of
Hospital (%)
Rest of
Hospital
(%)
Difference
(%)
Overall Perceptions of
Safety
38
59
−21
6.60
59
63
−4
1.05
Frequency of Events
Reported
45
53
−8
1.95
52
56
−4
0.69
Manager Expectations
Promoting Safety
77
76
1
0.46
82
76
6
1.93
Organizational
Learning
72
72
0
0.18
85
77
8
2.37
Teamwork within
Units
73
79
−5
2.09
82
81
1
0.34
Communication
Openness
42
58
−16
4.35
54
56
−2
0.39
Feedback and
Communication about
Error
52
62
−10
2.58
67
64
3
0.72
Non-punitive
Response to Error
39
45
−6
1.77
51
48
3
0.71
Staffing
40
52
−12
3.64
56
52
4
0.91
Management Support
for Patient Safety
71
76
−5
1.60
78
80
−2
0.47
Teamwork across
Hospital Units
63
65
−2
0.68
79
67
12
3.41
Handoffs and
Transitions
30
47
−17
4.90
57
51
6
1.62
Safety Dimension
Difference (%)
Critical
Ratio Test
(z >1.96)
Study
Units
(%)
Critical
Ratio Test
(z >1.96)
*Legend: Those results presented in shaded grey boxes are considered clinically improved (≥5%); in blue boxes are considered statistically improved (z >1.96); in yellow boxes represent no change; in
purple boxes are considered statistically worse; and in pink boxes are considered clinically worse (≤5%).
5% higher or lower to be considered clinically significant. We
also tested for statistical significance within the study units, as
well as compared with the rest of the hospital, which served as
our control group.
which is an area of emphasis for the organization. Nine of the
12 safety dimensions were also statistically significant (Table 1).
Study Teams Pre- and Post-intervention
At baseline, the aggregated results for the study teams scored
clinically lower than results for the rest of the hospital in
nine of the 12 safety dimensions, and statistically lower in six
dimensions (Table 2). Many of these dimensions were related
to teamwork and communication. Post-intervention, intervention units scored clinically higher in four safety dimen-
Over the study period, the geriatric and musculoskeletal rehabilitation teams showed clinically meaningful change (using the
5% rule of thumb) in all 12 safety dimensions of the HSOPSC.
Many of these improvements were greater than 10% and ranged
as high as 28% in the Handoffs and Transitions dimension,
Study Teams Compared with the Rest of the Hospital
Pre- and Post-intervention
Healthcare Quarterly Vol.13 Special Issue September 2010 97
�Using SBAR to Communicate Falls Risk and Management in Inter-professional Rehabilitation Teams Angie Andreoli et al.
Table 3. Comparison in change scores within the study teams and the rest of the organization
Pre-post Results for Study Team
Safety Dimension
Change
(%)
Pre-post Results for Rest of Hospital
Critical Ratio Test
(z >1.96)
Change (%)
Critical Ratio Test
(z >1.96)
Overall Perceptions of Safety
17
4.43
4
1.98
Frequency of Events Reported
4
1.29
3
1.50
Manager Expectations Promoting Safety
5
1.11
0
0.17
Organizational Learning
8
3.04
5
2.39
Teamwork within Units
6
2.23
3
1.43
Communication Openness
15
2.33
−2
0.61
Feedback and Communication about Error
13
2.70
2
0.88
9
2.31
3
1.19
16
3.49
0
0.39
3
1.57
4
2.69
Teamwork across Hospital Units
14
3.82
2
1.28
Handoffs and Transitions
23
5.76
4
2.04
Non-punitive Response to Error
Staffing
Management Support for Patient Safety
*�Legend: Those results presented in shaded grey boxes were considered clinically improved (≥5%); in blue boxes were considered statistically improved (z >1.96); and in yellow boxes represent no
change.
sions: Manager Expectations Promoting Safety, Organization
Learning – Continuous Improvement, Teamwork across Units
and Handoffs and Transitions. Two of these dimensions were
also statistically significant.
Table 3 examines these change scores in greater detail. It
compares the changes within the study units and the control
group pre- and post-intervention. While the organization
showed some improvements in clinical (one dimension) and
statistical scores (four dimensions), the study teams demonstrated clinically significant change in 10 dimensions and statistically significant change in nine.
Team Orientation Scale
The Team Orientation Scale was administered to the study
teams at baseline and following the implementation of SBAR.
This scale measures team effectiveness and incorporates issues of
team communication, team perspectives and valuing others, and
is part of a larger questionnaire based on the cognitive-motivational survey by Millward and Purvis (1998). The survey and its
domains have been found to be valid and reliable. Pre-and postimplementation, the study teams showed significant change in
four of the 10 items, including items that emphasized effective
98
Healthcare Quarterly Vol.13 Special Issue September 2010
and agreed-upon methods of communication, and a belief that
participants’ contributions were valued (Table 4).
Safety Reporting
Falls incidence and severity, as well as near-miss reporting, were
examined through our online reporting system. Severity ratings
were categorized in four levels (no harm, minor, moderate and
major) and tracked over an 18-month period, including the
six months leading up to and following the study period. Both
near-miss reporting and the number of major falls demonstrated
an overall decreasing trend across both the organization and the
study units. Conversely, total falls showed an increasing trend
on the study teams. These data do not account for repeat fallers;
nor do they consider whether falls increased on these units or if
staff were simply reporting more incidents. Figure 2 shows the
total number of major falls, or falls causing serious injury, on
the two study team units rehabilitation units compared to the
entire organization.
Process Evaluation: How Was SBAR Used?
The aim of the process evaluation was to further explore the
uptake (or not) of SBAR on the two inter-professional rehabili-
�Angie Andreoli et al. Using SBAR to Communicate Falls Risk and Management in Inter-professional Rehabilitation Teams
Table 4. Team Orientation Scale pre- and post-intervention
Pre-intervention
(% Agree)
Postintervention
(% Agree)
Change (%)
Critical Ratio
Test (z >1.96)
1. Team members act upon the information I communicate to them.
74
83
9
1.00
2. I am able to communicate effectively with team members.
74
91
17
2.12
3. This team has agreed methods for communication.
40
79
39
4.16
4. Communication between team members is unclear.
37
69
32
3.33
5. I regularly communicate with other members of the team.
96
94
−2
−0.04
6. �I act upon the information that other members of the team
communicate to me.
96
96
0
−0.38
7. All team members’ perspectives are important.
100
96
−4
0.95
8. �This team believes it is important to consider the perspectives of all
team members.
82
87
5
0.49
9. I believe other team members value my contribution to our work.
78
93
15
1.97
10. Each team member plays a valuable role within the team.
95
96
1
Item
0.003
*Legend: Those results presented in blue boxes were considered statistically improved (z >1.96); and in yellow boxes represent no change.
tation teams and to provide additional contextual understanding
of our results. To do this, we conducted brief one-on-one interviews with all participants mid-way through the study. We
also held focus groups (n = 18) on each of the study units at
the end of the implementation period. Each focus group was
conducted by two experienced moderators and was audiotaped
and transcribed verbatim. These groups provided us with an in
depth understanding of the enablers of and barriers to using
structured communication on inter-professional teams. For
example, at the beginning of the study participants regularly
said to us, “We are good communicators. Why do we need
SBAR? We do this already!” At the end of the study, however,
this notion had changed. Many participants expressed that
while they were able to provide the situation and background
of an issue; they only sometimes offered their assessment and
rarely made a recommendation.
Three main themes emerged from this evaluation. First,
staff used SBAR to communicate falls prevention and management; but they also used the tool in a variety of other clinical
and non-clinical contexts, for example, as a debriefing tool and
to discuss changes in team processes. Second, participants used
SBAR in situations that they perceived to be sensitive or hierarchical in nature (e.g., when approaching their manager or during
conflict resolution). And third, staff used the tool in urgent situations (e.g., changes in a patient’s health status); but they also
used it in a variety non-urgent situations, including changes in a
patient’s treatment plan and during transitions in care.
Recommendations for the Adoption of SBAR
in Other Clinical Settings
Results from this study suggest that SBAR was widely and effectively used by inter-professional rehabilitation teams as part of
a broader program of safety activities. In particular, we have
seen compelling changes in staff perceptions of safety culture, as
well as effective team processes and communication. Based on
experiences with both our pilot and expanded studies, we offer
the following recommendations to other organizations considering adopting structured communication tools:
Healthcare Quarterly Vol.13 Special Issue September 2010 99
�Using SBAR to Communicate Falls Risk and Management in Inter-professional Rehabilitation Teams Angie Andreoli et al.
Figure 2. Total number of major falls reported
GR = geriatric rehabilitation; MSK = musculoskeletal rehabilitation.
• Sustain the momentum. SBAR champions emerged
naturally from the study teams and were an effective means
to reinforce, encourage and model the use of SBAR. We
also included clinical and support staff in both phases of the
study, which made the SBAR process relevant to the entire
rehabilitation unit and additionally recognized the key role
that support staff play in patient safety within the organization. Finally, we found that reminder tools, such as telephone
prompts and pocket cards were useful and widely utilized.
• Recognize the diversity of the SBAR conversation. We
asked teams to structure their SBAR conversations around
communicating the issue of falls risk and management (e.g.,
SBAR to communicate falls risk assessment, as a handoff
mechanism at shift change to discuss falls issues or as a
post-falls debriefing tool); however, staff also used the tool
in a multitude of other urgent and non-urgent situations.
Whatever the context, SBAR was not used randomly − staff
consistently used the tool for what they perceived to be sensitive or hierarchical issues.
• Consider the value of context-dependent and relevant
case examples to reinforce the value of SBAR during
education sessions. We developed role-playing scenarios
from clinical situations that were meaningful to the study
teams, as an effective means to practise the SBAR process. We
also built in evaluative and tracking mechanisms throughout
100
Healthcare Quarterly Vol.13 Special Issue September 2010
the implementation phase
that reinforced an iterative “learning-in-action”
approach. This allowed us
to refine the tool and our
processes.
• Consider implementing SBAR in
clinical environments
with teams that may be
underperforming. We
implemented SBAR onto
two teams with a high falls
incidence. Implementing
change initiatives, even
pilot studies, on highperforming teams may be
a lost opportunity. Staff
found the tool useful in
helping to communicate
relevant and succinct
information and to “close
the loop” by providing
recommendations and
accountabilities for
action.
• Use our implementation tool kit. From our previous work,
we developed an implementation tool kit for enhanced
uptake of SBAR in other healthcare settings. This tool kit
is currently in its second edition (Trentham et al. 2010)
and includes a video DVD showing SBAR in action. The
DVD uses falls prevention and management as a platform
to highlight inter-professional team communication in
two different scenarios: during team rounds and between
two clinicians on the nursing unit. Each of these scenarios
demonstrate both ineffective and effective team communication. The accompanying facilitator’s guide emphasizes key
teaching moments for educators to consider when SBAR
education sessions. The tool kit and DVD are available free
of charge at www.torontorehab.com/SBAR.
Study Limitations
We used falls incidence and near-miss reporting as well as
severity of falls as proxy measures for safety. While near-miss
and total major falls showed a decreasing trend, total falls on
the study units increased. It does not seem that SBAR had a
significant impact on these measures for a few reasons. First,
the data may be trended across a time frame that is too short to
determine accurate results and may therefore be inconclusive.
Second, the nature of rehabilitation is to push patients to the
limits of their abilities in order to maximize function. In this
�Angie Andreoli et al. Using SBAR to Communicate Falls Risk and Management in Inter-professional Rehabilitation Teams
References
way, the risk of falls and other events are an inherent part of
the rehabilitation process.
We cannot attribute changes in safety reporting and perceptions of patient safety solely to this study; instead, these changes
should be considered within the context of a range of patient
safety initiatives at Toronto Rehab. For example, new initiatives
regarding leader engagement, upgrades to our online reporting
system and a corporate-wide falls best practice initiative have
all increased awareness of safety and incident reporting across
the organization.
We used the 5% rule of thumb to suggest clinically significant change in the HSOPSC; however, this guideline was
meant to be used with large sample sizes. We chose to aggregate
the study results for a number of reasons, including statistical
power. It would also be interesting to look at the study units
individually with the specific purpose of sharing key learnings
across our organization.
Joint Commission on Accreditation of Healthcare Organizations.
2004. Root Causes of Sentinel Events, 1995–2004 (Report). Oakbrook
Terrace, IL: Author. The Joint Commission.
The adapted SBAR process is an
Trentham, B., A. Andreoli, N. Boaro, K. Velji and C. Fancott. 2010.
SBAR: A Shared Structure for Team Communication. Adapted for
Rehabilitation and Complex Continuing Care: An Implementation
Toolkit (2nd ed.). Toronto, ON: Toronto Rehabilitation Institute.
effective way to communicate urgent
and non-urgent safety issues and has the
potential to be widely used among interprofessional teams.
Conclusions
The purpose of this study was to implement and evaluate the
adapted SBAR tool for use on two inter-professional rehabilitation teams for the specific priority issue of falls prevention and
management. Issues of patient safety and communication have
been studied in the literature, but usually from the perspective
of acute care and involving nurse-physician communication.
This study contributes to the literature in patient safety by
examining the influence that strong inter-professional team
collaboration and communication can have on falls prevention
and management in rehabilitation. These results suggest that
the adapted SBAR process is an effective way to communicate
urgent and non-urgent safety issues and has the potential to be
widely used among inter-professional teams. Our next steps are
to consider SBAR as one of our organizational best practices and
as part of “how we do business”. While SBAR has been adapted
for use within our setting, it is one of a number of structured
team communication tools. Our hope is that these learnings
are transferable to other healthcare settings, settings that also
recognize the importance (and challenges) of communicating
in inter-professional teams.
Acknowledgements
This project was jointly funded by the Canadian Patient Safety
Institute and the Toronto Rehabilitation Institute.
American Geriatrics Society, British Geriatrics Society and American
Academy of Orthopaedic Surgeons Panel on Falls Prevention. 2001.
“Guideline for the Prevention of Falls in Older Persons.” Journal of the
American Geriatrics Society 49(5): 664–72.
Boaro, N., C. Fancott, G.R. Baker, K. Velji and A. Andreoli. 2010.
“Using SBAR to Improve Communication in Interprofessional Teams.”
Journal of Interprofessional Care 24(10): 111–14.
Leonard, M., S. Graham and D. Bonacum. 2004. “The Human Factor:
The Critical Importance of Effective Teamwork and Communication
in Providing Safe Care.” Quality and Safety in Health Care 13: 85–90.
Millward, L. and R. Purvis. 1998. Team Building Techniques – A Critical
Evaluation. Farnborough, United Kingdom: Defense Evaluation
Research Agency, Centre for Human Sciences.
Registered Nurses’ Association of Ontario. 2007. Falls Prevention:
Building the Foundations for Patient Safety. A Self Learning Package.
Toronto, ON: Author.
Velji, K., G.R. Baker, C. Fancott, A. Andreoli, N. Boaro, G. Tardif et al.
2008. “Enhancing Effective Team Communication for Patient Safety.”
Healthcare Quarterly 11(Special Issue): 72–79.
Westat, R., J. Sorra and V. Nieva. 2004. Hospital Survey on Patient
Safety Culture (Publication No. 04-0041). Rockville, MD: Agency for
Healthcare Research and Quality. Retrieved January 10, 2009. <http://
www.ahrq.gov/qual/hospculture/>.
About the Authors
Angie Andreoli, BSc(PT), MSc, is the acting advanced
practice leader of patient safety at the Toronto Rehabilitation
Institute (Toronto Rehab), in Toronto, Ontario. She can be
contacted at (416) 597-3422 x 3984 or andreoli.angie@
torontorehab.on.ca.
Carol Fancott, BSc(PT), MSc(PT), PhD(c), is the advanced
practice leader of patient safety at Toronto Rehab.
Karima Velji, RN, PhD, is vice-president of clinical and
residential programs and chief nursing officer at Baycrest
Hospital in Toronto, Ontario.
G. Ross Baker, PhD, is a professor in the Department of
Health Policy, Management and Evaluation at the University
of Toronto.
Sherra Solway, BSc(PT), MHSc, CHE, is the director of
patient safety, best practice, and patient care projects at
Toronto Rehab.
Elaine Aimone, BSc(PT), MSc, is the director of quality and
risk services and accreditation manager at Toronto Rehab.
Gaétan Tardif, MD, FRCPD, FCCHSE, is vice-president of
quality patient care and chief medical officer at Toronto
Rehab, and a professor of medicine at the University of
Toronto.
Healthcare Quarterly Vol.13 Special Issue September 2010 101
�
 Carol Fancott
Carol Fancott