Obesity Surgery, 17, 962-969
Review Article
Sleeve Gastrectomy for Morbid Obesity
Andrew A. Gumbs, MD; Michel Gagner, MD; Gregory Dakin, MD; Alfons
Pomp, MD
New York-Presbyterian Hospital, Division of Laparoscopy, and Department of Surgery WeillCornell College of Medicine, New York, NY, USA
The rising prevalence of morbid obesity and the
increased incidence of super-obese patients (BMI >50
kg/m2) seeking surgical treatments has led to the
search for surgical techniques that provide adequate
EWL with the least possible morbidity. Sleeve gastrectomy (SG) was initially added as a modification to
the biliopancreatic diversion (BPD) and then combined with a duodenal switch (DS) in 1988. It was first
performed laparoscopically in 1999 as part of a DS
and subsequently done alone as a staged procedure
in 2000. With the revelation that patients experienced
weight loss after SG, interest in using this procedure
as a bridge to more definitive surgical treatment has
risen. Benefits of SG include the low rate of complications, the avoidance of foreign material, the maintenance of normal gastro-intestinal continuity, the
absence of malabsorption and the ability to convert to
multiple other operations. Reduction of the ghrelinproducing stomach mass may account for its superiority to other gastric restrictive procedures. SG
should be in the armamentarium of all bariatric surgeons. Nonetheless, long-term studies are necessary
to see if it is a durable procedure in the treatment of
morbid obesity.
Key words: Gastric, sleeve, Magenstrasse & Mill procedure, gastroplasty, morbid obesity, bariatric surgery
Correspondence to: Michel Gagner, MD, Chief, Laparoscopic
and Bariatric Surgery, Department of Surgery, Joan and Sanford
I. Weill Medical College of Cornell University, New YorkPresbyterian Hospital-Weill Cornell Medical Center, 525 East 68
Street, PO Box 294, New York, NY 10021, USA.
E-mail: mig2016@med.cornell.edu
962
Obesity Surgery, 17, 2007
Introduction
The most commonly performed bariatric procedure
in the USA is Roux-en-Y gastric bypass (RYGBP).1
This is due to its effective long-term weight loss and
treatment of co-morbidities, as well as the fact that it
is being increasingly performed laparoscopically.2-4
Initially, the National Institutes of Health supported
RYGBP and the vertical banded gastroplasty (VBG)
in the treatment of morbid obesity refractory to lifestyle modifications and diets.5 Laparoscopic
adjustable gastric banding (LAGB) was approved in
the USA after a lengthy FDA trial. However, there is
some concern about its effectiveness due to the lower
degree of weight loss compared to RYGBP and VBG
and due to the fact that one-third of bands have had to
be removed in some studies.1,6 In 2004, the Centers
for Medicare and Medicaid Services (CMS) added
biliopancreatic diversion (BPD) to the list of recommended bariatric procedures for the surgical management of morbid obesity. This also followed a consensus conference of the American Society for Bariatric
Surgery in 2004.7,8
Sleeve Gastrectomy (SG) was first described as a
modification to the BPD and combined with a duodenal switch (DS) in 1998, and first performed
laparoscopically in 1999.9-11 It consists of a SG as a
component of restriction and then duodeno-ileostomy as an intestinal bypass. Benefits of SG in BPDDS include preservation of the pyloric valve and
gastric antrum as compared to distal gastrectomy in
standard BPD, resulting in decreased complications
© Springer Science + Business Media, Inc.
�Sleeve Gastrectomy for Morbid Obesity
associated with gastrojejunostomy such as marginal
ulceration and dumping syndrome.12 Benefits of DS
over BPD include a small duodenal segment that
absorbs iron and calcium.
Initial success in bariatric surgery is defined as a
>50% loss of excess weight, or 50% EWL.1,6
Average %EWL is greatest with BPD (range 7580%), followed by RYGBP (range 60-85%), then
VBG (range 50-60%). LAGB has a %EWL in the
range of 23-70%.1,6 Although the initial experience
with BPD was associated with higher complications
due to a more difficult anatomic dissection, interest
in this procedure has grown due to increasing experience with performing BPD-DS laparoscopically,
the low rate of complications at large academic centers, and the superior %EWL in the long-term.13 As
experience with BPD-DS grew, surgeons attempted
to perform this operation in increasingly obese
patients and at times chose to abandon the procedure after only performing the SG.14
Patients experience excellent weight loss after SG
alone, and multiple recent reports have documented
SG as single therapy in the treatment of morbid obesity.14-23 Nonetheless, the use of SG as a bridge to
more definitive surgery is perhaps its most interesting
role. In super-obese (BMI >50 kg/m2) and supersuper obese (BMI >60 kg/m2) patients, the incidence
of complications and mortality is increased due to
more prevalent co-morbidities and increased difficulty in performing surgery.24 By using less invasive procedures such as SG as initial management in the
super-obese, overall morbidity and mortality may be
reduced in this patient population.24
cipal that gastric restriction would lead to weight loss
and that these procedures needed to be accomplished
by dividing the stomach and not simply stapling it.25
The Magenstrasse or “street of the stomach” is the
name given to the narrow tube of lesser curvature created after division of the proximal greater curvature.
Experience from non-divided VBG led surgeons to
promote stapled division to avoid gastro-gastric fistulization from the gastric remnant to the restricted
portion of the stomach.25,26 This restricted stomach is
created by a similar technique to that used for VBG.
In the standard VBG, the EEA is fired from ~6 cm
distal to the esophago-gastric junction at about the
middle of the lesser curvature.
In the M&M procedure, an EEA stapler is fired
along the junction of the antrum and body of the
stomach just distal to the incisura angularis. After
placement of a 32-36 Fr bougie, sequential firings of
GIA staplers to the angle of His complete the creation of the Magenstrasse. The remaining antrum is
known as the Mill because of the normal grinding
that the food bolus undergoes before its expulsion
into the duodenum.25,27 SG is essentially a completion of the Magenstrasse distally, by completely
separating the greater curvature of the stomach from
the lesser curvature and antrum. However, the
M&M procedure by leaving the ghrelin-producing
portion of the stomach in situ, may lessen the beneficial satiety hormonal effects of the SG. (Figure 1).
The Magenstrasse and Mill Procedure
The concept for sleeve gastrectomy (SG) in the primary treatment of morbid obesity came as a modification of the DS in the USA where patients were
treated with the first portion of the DS and only
underwent SG. Although similar in technique to the
restrictive Magenstrasse and Mill procedure (M&M)
developed in the United Kingdom, SG is conceptually different because its efficacy is based on the
removal of the grehlin-producing portion of the stomach. First described in 1995 by a group in Leeds,
England, the M&M procedure was based on the prin-
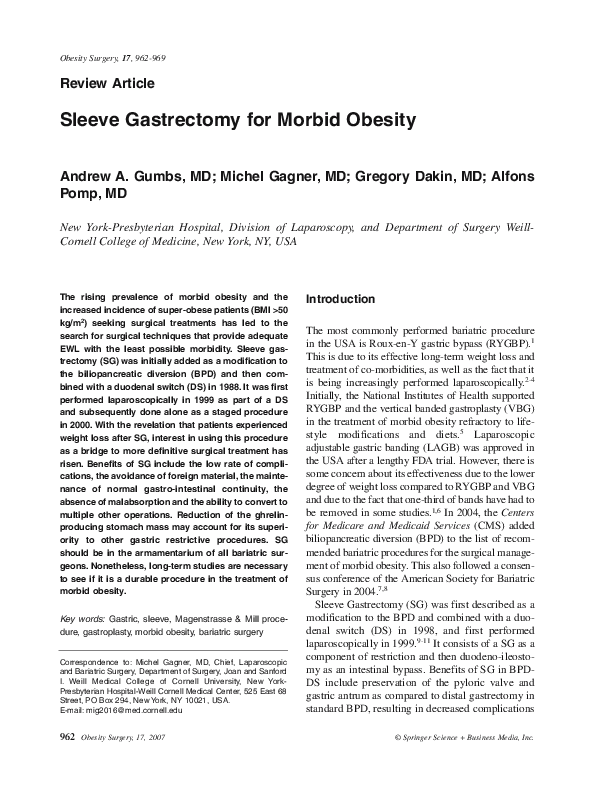
6 cm
Figure 1. Image of laparoscopic placement of endoscopic stapler, 6 cm proximal to the pyloric valve at approximately the incisura angularis, for a laparoscopic sleeve
gastrectomy.
Obesity Surgery, 17, 2007
963
�Gumbs et al
Restrictive bands are not placed, because the length
of the gastric tube created is believed to provide adequate restriction.25 Separation of the greater curvature
from the rest of the stomach is also advocated,
because it is believed that the greater curvature and
fundus are particularly elastic and prone to dilation
over time.28 Another benefit of the M&M procedure
is the preservation of gastric emptying. Concomitant
problems such as diarrhea, dumping and vomiting are
also reduced when compared to RYGBP.29,30 Furthermore, the M&M procedure eliminates the need for a
foreign material to create a restrictive band or for
placement of a subcutaneous reservoir.27
In the largest published series to date analyzing
the results of 100 morbidly obese patients who
underwent the M&M procedure, mean EWL was
60% after 1 year. Patients were followed for up to 5
years, and no significant weight loss was found after
the first postoperative year.27 In a study of 39
patients and another study of 43 patients 3 years
after undergoing the M&M procedure, a decrease in
insulin resistance and significantly lower levels of
plasma insulin after weight loss were found when
compared to control groups.31,32
Sleeve Gastrectomy
SG has been gaining popularity because it can be
created with relative ease via minimally invasive
techniques. Three 10-mm ports are placed: in the
supra-umbilical region, between the subxiphoid
space and umbilicus, and in the right upper quadrant.
Two working 15-mm ports to be used for stapling are
placed in the mid-abdomen just medial to the midclavicular lines, and one 5-mm port for retraction is
placed in the left upper quadrant (Figure 2).
Alternatively, all stapling can be done through one
working trocar along the right paramedian line.33
The assistants stand on either side of the patient and
the surgeon stands in-between the legs with the
patient in the French position (Figure 3).
SG, as the first operation in a two-stage management of morbid obesity, was first reported in superobese patients who underwent a laparoscopic sleeve
gastrectomy followed by a second stage laparoscopic RYGBP.16 Since that initial study, a total of 15
studies have been published looking at outcomes
964
Obesity Surgery, 17, 2007
Figure 2. Trocar placement for laparoscopic sleeve gastrectomy.
reported as %EWL after SG with at least 6 months
follow-up, of which one is in abstract form.23
Although % excess BMI loss would be more accurate,34 most papers did not report this data, and thus
%EWL was used. In total, 646 patients were reported with an average BMI of 51 (Table 1).14,16-24,35-39
Figure 3. Position of surgeon between the patient’s legs
in the “French” position, with the camera holder on the
patient’s right and the other surgical assistant on the
patient’s left.
�Sleeve Gastrectomy for Morbid Obesity
regain after laparoscopic BPD-DS with re-operative
SG. This patient initially went from a BMI of 64 to
29, but after 17 months was found to be regaining
weight. The authors questioned whether she would
benefit from further bypass or restriction. An upper
GI series found that her gastric pouch had dilated significantly over this period and the decision was made
to perform a repeat SG of the dilated stomach. At 10
months after this revision, the patient’s BMI was
noted to have fallen to 22.40
In an effort to avoid gastric dilation in the longterm, surgeons began performing SG with the smallest possible bougies. This was because of the gastric
dilation noted after M&M procedures and the reduction of this dilatation after such techniques as micropouch creation for RYGBP.25,27,28 In our experience,
durable weight loss can be observed after SG if a
bougie no larger than a 42 Fr is used for primary
treatment of morbid obesity. Although not published,
we have data that suggest that a 34-Fr bougie may
provide superior weight loss without any increased
postoperative intolerance. In patients who are candi-
The mean EWL is reported as 49% and 56% at 6
and 12 months, respectively. The average follow-up
time is 12 months for these studies.
Complications occurred in ~9% of patients and
include one intra-operative splenic injury not requiring splenectomy (Table 2).14,16-24,35-39 Postoperative
complications included trocar-site problems such as
infection, hernia and hemorrhage. Other postoperative complications include urinary tract infection and
atelectasis. There was one documented leak at the
transection site with delayed gastric emptying, presenting as gastric dilation and prolonged emesis.
There were 4 reported mortalities (<1%): one was
due to a traumatic trocar insertion, the second was in
the peri-operative period, the third due to primary
peritonitis 3 weeks after surgery even though no leak
or bowel ischemia was identified at autopsy, and the
fourth patient died secondary to a pulmonary embolus 3 months after surgery.19,20,24,36
The first reported use of SG as revisional therapy in
the treatment of recurrent morbid obesity was in 2003
when Gagner et al40 reported the treatment of weight
Table 1. Outcome of published series on sleeve gastrectomy
Study
No.
Pre-op
BMI
%EWL
6/12 (mos)
Compl
(%)
Mort
(%)
Weight
Regain (%)
Average Resolution of
f/u (mos) co-morbidities
Himpens 200635
Hammoui 200636
Roa 200637
Mognol 200638
Silecchia 200639
Lee 200623
Cottam 200624
Catheline 200617
Langer 200618
Han 200519
40
118
30
10
41
216
126
4
23
60‡
39
55
41
64
57
49
65
65
48.5
37
NR/58
38/49
53/NR
NR/51
NR
NR/58†
NR/45
40/NR
46/56
71/81
5
15
13
0
NR
6
14
25
4
1
0
<1
0
0
NR
0
<1
0
0
1
NR
NR
NR
NR
NR
4.2§
NR
0
13
7
12
12
6
12
12
24
12
6
20
12
Baltasar 200520
31
35-74
56-71
3
3
NR
3-27
Mognol 200514
Langer 200521
Milone 200522
Regan 200316
10
10
20
7
64
48
69
63
NR/51
61/NR
35/NR
33*
0
NR
5
29
0
NR
0
0
NR
NR
NR
NR
12
6
6
11
NR
NR
NR
NR
60+
NR
>75
NR
NR
HTN (93-100)**
DM (100)
HTN (100)
DM (100)
NR
NR
NR
NR
Total
Mean
646
51
49/56
9
<1
7
12
60-100
†= %EWL at 24 months was 83, §= weight loss plateau (<4.5 kg lost/6 mos), No. = patients, Compl= complications, Mort= mortality,
HTN= hypertension, DM= diabetes mellitus, ‡130 total patients analyzed in calculation of complications, *%EWL at 11 months, + and
additional 24% had improvement in co-morbidities, **93% of patients had resolution in HTN and 100% had improvement.
Obesity Surgery, 17, 2007
965
�Gumbs et al
Table 2. Reported complications after sleeve
gastrectomy
Reoperations*
Leak
Prolonged Ventilator Requirements**
Strictures
Renal Insufficiency
Postoperative hemorrhage
Atelectasis
Pulmonary Embolus†
Delayed Gastric Emptying
Gastric Dilation
Prolonged vomiting
Subphrenic abscess
Trocar-site infection
Urinary Tract Infection
Splenic Injury
Trocar site hernia
Death
29
6
5
5
4
2
2
2
2
1
1
1
1
1
1
1
4
Complications after 646 Gastric Sleeves for morbid obesity.
*indications not reported, ** >24 hour ventilator requirements,
†1 resulted in death.14,16-24
dates for BPD-DS as a single stage operation, we
generally use a 60-Fr bougie because the restriction
obtained with a smaller bougie combined with duodeno-ileostomy can be too severe for most patients to
tolerate.10,12,40 Again, new data seem to suggest that
smaller bougies may be similarly tolerated in these
patients; our analysis is still underway.
Another concern preventing surgeons from
embracing SG has been the long staple-line created
along the stomach. Concerns regarding staple-line
hemorrhage and leak have resulted in attempts to
avoid these complications by the use of buttressing
material. We initially used non-absorbable material
as a buttress along staple-lines in bariatric surgery.
However, after one case of bovine pericardium
migration in a patients’ emesis, this practice was
stopped.42 We subsequently began using an
absorbable polymer buttress material along our SG
staple-lines and noted decreased instances of stapleline hemorrhage and leak. Use of this material
resulted in decreased overall complications and
length of stay.43 Importantly, many groups use a
continuous running suture of the staple-lines and
note that this adequately controls staple-line hemorrhage and may decrease adhesion formation with a
lower overall operative cost.
966
Obesity Surgery, 17, 2007
Because of the rising incidence of super-obese
patients, interest in less invasive techniques for the
treatment of these patients as a bridge to more definitive surgery has increased. The first study to
demonstrate superiority of SG to another weight
loss modality was published in 2004. Comparing 20
patients who underwent laparoscopic SG to historical controls of patients treated with an intragastric
balloon, superior EWL at 6 months was observed
for the SG group.22 Although the endoscopicallyplaced intragastric balloon resulted in a %EWL of
24 over this period, SG obtained superior %EWL
(33) and was better tolerated.22
In another study comparing laparoscopic SG to
LAGB, superior EWL was found after 6 months,
61% vs 29%. It was theorized that the resection of
the fundus after SG reduced a large area of ghrelinproducing stomach. The authors found decreased
levels of ghrelin in the SG patients after 1 and 6
months and no change after LAGB.21 The removal
of large hormonally active areas of the stomach may
account for the superior results seen after SG, but
studies with longer follow-up are needed.21
Recently, Givon-Madhala et al44 performed 25
consecutive laparoscopic sleeve gastrectomies as
sole therapy in patients with average BMI 43 kg/m2,
and reported early percent excess BMI loss of 49
and no complications. Only long-term follow-up
studies, however, will ascertain the effectiveness of
laparoscopic SG as a sole operation.
Sleeve Gastrectomy in Two-Stage
Procedures
To date, there have been only two published reports
on patients undergoing staged laparoscopic RYGBP
after an initial SG. The first report by Regan and
colleagues16 described 7 patients with an initial
average BMI of 63 kg/m2. They underwent a laparoscopic sleeve gastrectomy as an initial procedure
and over an average of 11 months experienced a
mean %EWL of 33%. Six of their patients underwent second-stage laparoscopic RYGBP and at very
early follow-up had an additional mean %EWL of
40%. There were no mortalities in this series,
although 5 minor complications did occur.16
Another group described staged laparoscopic
�Sleeve Gastrectomy for Morbid Obesity
RYGBP but utilized a different initial procedure.15
These authors note that in the super-obese, exposure
of the angle of His is difficult due to the large size of
the liver, making sleeve gastrectomy difficult.
Therefore, instead of performing an initial restrictive
procedure, they performed a modified laparoscopic
RYGBP with a low gastrojejunal anastomosis and a
larger gastric pouch encompassing the gastric fundus.
The low anastomosis obviated the need for exposure
of the gastroesophageal junction and the angle of His.
They then describe a second-stage procedure to be
performed after a 6-12 month period of weight loss
where the large gastric fundus portion of the pouch is
removed with a “completion” sleeve gastrectomy.
This report is only a description of the technique and
gives no data on the results of surgery.15
The use of second-stage surgery is appealing
because it has the potential to reduce morbidity in
high-risk super-obese patients. Obviously, this is a
new concept that has yet to be proven with prospective study. One key issue to be determined is the
timing of second-stage surgery. Some may favor
performing a second-stage procedure at a set interval after the initial surgery while the patient is still
in a period of rapid weight loss. Others may argue
that it is best to wait until weight loss plateaus
before performing a second stage, thereby maximizing the effect of the first stage. Another important
question that remains unanswered is what operation
to perform as a second stage, with RYGBP, DS, and
adjustable band all being viable options.
Discussion
As the global population continues to suffer from
increasing obesity, surgeons have begun devising safer
methods for the management of these patients. By performing less invasive procedures as the initial part of a
two-staged surgical regimen, complications and mortality can be kept to a minimum.15,16 The least invasive
procedures for the management of morbid obesity are
the ones that result in pure gastric restriction.21,22 One
method for the management of super-obese patients
has become the two-stage SG followed by duodenoileostomy in the BPD-DS procedure.12,21 As experience with this procedure has grown, some surgeons
have begun using SG as solitary therapy for the treat-
ment of morbid obesity. This is because of the lack of
need for foreign material, excellent patient tolerance
by maintenance of gastric emptying, and decreased
incidence of nutritional deficiencies.14,16-22 A very
recent study of 23 patients, not included in this analysis, found that after SG, stomach contents actually
empty rapidly into the small intestines casting doubt as
to whether this procedure is truly restrictive and underscoring the possibility that gut hormonal alterations
may play a larger role in satiety and weight loss than
currently appreciated.45
SG is essentially a modification of the M&M procedure and has gained popularity in the laparoscopic era because of the ease of performing SG via minimally invasive techniques. Although the M&M has
adequate weight loss with follow-up of up to 5 years
reported in 16 patients, this procedure has not been
reported laparoscopically or from outside of one
center in Leeds, England.25,27 Nonetheless, the experience from this procedure has greatly assisted our
understanding of the optimal creation of the gastric
sleeve. When bougies of 40 Fr have been used in the
creation of the M&M, gastric dilatation has been
reported. When bougies of 32-36 Fr were utilized,
no difference in EWL has been found and no incidence of gastric dilatation has been reported.27
In one study, 20 patients who underwent laparoscopic SG over a 48 Fr bougie were followed for an average
of 20 months. EWL at 6 and 12 months was 46% and
56%, respectively. All patients were screened for gastric dilatation with an upper GI series. Only 1 patient of
23 (4%) was found to have gastric dilation. SG has been
found to have excellent %EWL at 6 and 12 months, but
longer-term follow-up is needed to see the effects of
gastric dilation over time. An interesting treatment for
patients who do suffer from gastric dilatation postoperatively is re-operative SG. This procedure can also be
performed laparoscopically and has minimal morbidity.37,45 As a result, the lack of complete resection of the
greater curvature of the stomach may account for the
increased rate of gastric dilation seen after M&M procedures when bougies larger than 36 Fr are used.
Interestingly, some authors also recommend resecting
the antral portion of the greater curvature at the initial
surgery to prevent the risk of gastric dilation and the
need for re-sleeve gastrectomy in the future.45
Obesity Surgery, 17, 2007
967
�Gumbs et al
Conclusion
SG is an excellent procedure for the surgical management of morbid obesity. EWL at 6 and 12
months averages 49% and 56%, respectively.14,1624,35-39 Improvement in co-morbidities of obesity,
such as hypertension and diabetes mellitus, has been
reported to occur in the majority of patients with
resolution in 60-100%.19,20,24,39 When compared to
other restrictive procedures,46 the removal of the
greater curvature of the stomach may result in
decreased risk of gastric dilation and the removal of
ghrelin-producing stomach mass may result in better long-term weight loss. In populations with an
increased incidence of gastric cancer, SG is also
particularly useful for the reduction in gastric tissue
and the maintenance of GI continuity for preservation of a route for endoscopic surveillance. This
operation has a low incidence of complications and
mortality, and is particularly useful in the superobese who may benefit from a two-staged procedure.15,16,24 Although SG may be effective treatment
for morbid obesity up to 2 years after surgery,
longer term studies (>5 years) are necessary to
determine whether SG is a durable procedure in the
treatment of morbid obesity.23
Andrew A. Gumbs, MD was supported by fellowship grants from
Tyco Healthcare, U.S. Surgical, Norwalk, CT, USA (2005-6) and
KARL STORZ GmbH & Co. KG, Tuttlingen, Germany (2006-7).
This work was supported by grants from the Association pour la
Recherche contre le Cancer (ARC) of France and the Philippe
Foundation in Paris, France. The authors would also like to thank
Dr. Ziad Awad for the use of Figures 1-3.
References
1. Gumbs AA, Modlin IM, Ballantyne GH. Changes in
insulin resistance following bariatric surgery: role of
caloric restriction and weight loss. Obes Surg 2005;
15: 462-73.
2. Hickey MS, Pories WJ, MacDonald KG Jr et al. A
new paradigm for type 2 diabetes mellitus: could it be
a disease of the foregut? Ann Surg 1998; 227: 637-43;
discussion 643-4.
3. Cottam DR, Mattar SG, Schauer PR. Laparoscopic
era of operations for morbid obesity. Arch Surg 2003;
138: 367-75.
4. Rosenthal RJ, Szomstein S, Kennedy CI et al.
968
Obesity Surgery, 17, 2007
Laparoscopic surgery for morbid obesity: 1,001 consecutive bariatric operations performed at the
Bariatric Institute Cleveland Clinic Florida. Obes
Surg 2006; 16: 119-24.
5. Gastrointestinal surgery for severe obesity. National
Institutes of Health Consensus Development Conference
Draft Statement. Obes Surg 1991; 1: 257-65.
6. Ballantyne GH, Gumbs A, Modlin IM. Changes in
insulin resistance following bariatric surgery and the
adipoinsular axis: role of the adipocytokines, leptin,
adiponectin and resistin. Obes Surg 2005; 15: 692-9.
7. Proceedings of the ASBS Consensus Conference on
the State of Bariatric Surgery and Morbid Obesity:
Health Implications for Patients, Health Professionals
and Third-Party Payers, Washington, DC, USA, May
6-7, 2004. Surg Obes Relat Dis 2005; 1: 105-53.
8. 2004 ASBS Consensus Conference on Surgery for
Severe Obesity. Surg Obes Relat Dis 2005; 1: 297381.
9. Marceau P, Hould FS, Simard S et al. Biliopancreatic
diversion with duodenal switch. World J Surg 1998;
22: 947-54.
10.Ren CJ, Patterson E, Gagner M. Early results of
laparoscopic biliopancreatic diversion with duodenal
switch: a case series of 40 consecutive patients. Obes
Surg 2000; 10: 514-23; discussion 524.
11.de Csepel J, Burpee S, Jossart G et al. Laparoscopic
biliopancreatic diversion with a duodenal switch for
morbid obesity: a feasibility study in pigs. J
Laparoendosc Adv Surg Tech A 2001; 11: 79-83.
12.Gagner M, Boza C. Laparoscopic duodenal switch for
morbid obesity. Expert Rev Med Devices 2006; 3:
105-12.
13.Gagner M, Steffen R, Biertho L et al. Laparoscopic
adjustable gastric banding with duodenal switch for
morbid obesity: technique and preliminary results.
Obes Surg 2003; 13: 444-9.
14.Mognol P, Chosidow D, Marmuse JP. Laparoscopic
sleeve gastrectomy as an initial bariatric operation for
high-risk patients: initial results in 10 patients. Obes
Surg 2005; 15: 1030-3.
15. Nguyen NT, Longoria M, Gelfand DV et al. Staged
laparoscopic Roux-en-Y: a novel two-stage bariatric
operation as an alternative in the super-obese with massively enlarged liver. Obes Surg 2005; 15: 1077-81.
16.Regan JP, Inabnet WB, Gagner M et al. Early experience with two-stage laparoscopic Roux-en-Y gastric
bypass as an alternative in the super-super obese
patient. Obes Surg 2003; 13: 861-4.
17.Catheline JM, Cohen R, Khochtali I et al. [Treatment
of super super morbid obesity by sleeve gastrectomy].
Presse Med 2006; 35:383-7.
18.Langer FB, Bohdjalian A, Felberbauer FX et al. Does
�Sleeve Gastrectomy for Morbid Obesity
gastric dilatation limit the success of sleeve gastrectomy as a sole operation for morbid obesity? Obes Surg
2006; 16:166-71.
19. Moon Han S, Kim WW, Oh JH. Results of laparoscopic sleeve gastrectomy (LSG) at 1 year in morbidly
obese Korean patients. Obes Surg 2005; 15: 1469-75.
20.Baltasar A, Serra C, Perez N et al. Laparoscopic
sleeve gastrectomy: a multi-purpose bariatric operation. Obes Surg 2005; 15: 1124-8.
21.Langer FB, Reza Hoda MA, Bohdjalian A et al.
Sleeve gastrectomy and gastric banding: effects on
plasma ghrelin levels. Obes Surg 2005; 15: 1024-9.
22.Milone L, Strong V, Gagner M. Laparoscopic sleeve
gastrectomy is superior to endoscopic intragastric balloon as a first stage procedure for super-obese patients
(BMI ≥50). Obes Surg 2005; 15: 612-7.
23.Lee CM FJ, Cirangle PT, Jossart GH. Laparoscopic
vertical sleeve gastrectomy for morbid obesity in 216
patients: report of two-year results. SAGES 2006
Final Program 2006: 88.
24.Cottam D, Qureshi FG, Mattar SG et al. Laparoscopic
sleeve gastrectomy as an initial weight-loss procedure
for high-risk patients with morbid obesity. Surg
Endosc 2006; 20: 859-63.
25. Sue-Ling DJAH. Surgical Management of Morbid
Obesity, 3rd Edn. Oxford: Butterworth-Heinemann, 1995.
26.Baltasar A. Modified vertical gastroplasty: Technique
with vertical division and serosal patch. Acta Chir
Scand 1989; 155: 107-12.
27.Johnston D, Dachtler J, Sue-Ling HM et al. The
Magenstrasse and Mill operation for morbid obesity.
Obes Surg 2003; 13: 10-6.
28. Sapala JA, Wood MH, Sapala MA et al. The micropouch gastric bypass: technical considerations in primary
and revisionary operations Obes Surg 2001; 11: 3-17.
29.Carmichael AR, Sue-Ling HM, Johnston D. Quality
of life after the Magenstrasse and Mill procedure for
morbid obesity. Obes Surg 2001; 11: 708-15.
30.Carmichael AR, Johnston D, Barker MC et al. Gastric
emptying after a new, more physiological anti-obesity
operation: the Magenstrasse and Mill procedure. Eur
J Nucl Med 2001; 28: 1379-83.
31.Carmichael AR, Johnston D, King RF et al. Effects of
the Magenstrasse and Mill operation for obesity on
plasma leptin and insulin resistance. Diabetes Obes
Metab 2001; 3: 99-103.
32.Carmichael AR, Tate G, King RF et al. Effects of the
Magenstrasse and Mill operation for obesity on plasma plasminogen activator inhibitor type 1, tissue plasminogen activator, fibrinogen and insulin.
Pathophysiol Haemost Thromb 2002; 32: 40-3.
33.Baltasar A, Serra C, Perez N et al. Re-sleeve gastrectomy. Obes Surg 2006; 16: 1535-8.
34.Deitel M, Gawdat K, Melissas J. Reporting weight
loss 2007. Obes Surg 2007; 17: 565-8.
35.Himpens J, Dapri G, Cadiere GB. A prospective randomized study between laparoscopic gastric banding
and laparoscopic isolated sleeve gastrectomy: results
after 1 and 3 years. Obes Surg 2006; 16: 1450-6.
36.Hamoui N, Anthone GJ, Kaufman HS et al. Sleeve
gastrectomy in the high-risk patient. Obes Surg 2006;
16: 1445-9.
37.Roa PE, Kaidar-Person O, Pinto D et al. Laparoscopic
sleeve gastrectomy as treatment for morbid obesity:
technique and short-term outcome. Obes Surg 2006;
16: 1323-6.
38.Mognol P, Chosidow D, Marmuse JP. Laparoscopic
sleeve gastrectomy (LSG): review of a new bariatric
procedure and initial results. Surg Technol Int 2006;
15: 47-52.
39.Silecchia G, Boru C, Pecchia A et al. Effectiveness of
laparoscopic sleeve gastrectomy (first stage of biliopancreatic diversion with duodenal switch) on comorbidities in super-obese high-risk patients. Obes
Surg 2006; 16: 1138-44.
40.Gagner M, Rogula T. Laparoscopic reoperative sleeve
gastrectomy for poor weight loss after biliopancreatic
diversion with duodenal switch. Obes Surg 2003; 13:
649-54.
41.Feng JJ, Gagner M. Laparoscopic biliopancreatic
diversion with duodenal switch. Semin Laparosc Surg
2002; 9: 125-9.
42.Consten EC, Dakin GF, Gagner M. Intraluminal
migration of bovine pericardial strips used to reinforce the gastric staple-line in laparoscopic bariatric
surgery. Obes Surg 2004; 14: 549-54.
43.Consten EC, Gagner M, Pomp A et al. Decreased
bleeding after laparoscopic sleeve gastrectomy with
or without duodenal switch for morbid obesity using
a stapled buttressed absorbable polymer membrane.
Obes Surg 2004; 14: 1360-6.
44.Givon-Madhala O, Spector R, Wasserberg N et al.
Technical aspects of laparoscopic sleeve gastrectomy
in 25 morbidly obese patients. Obes Surg 2007; 17:
722-8.
45.Melissas J, Koukouraki S, Askoxylakis J et al. Sleeve
gastrectomy: a restrictive procedure? Obes Surg 2007;
17: 57-62.
46.Kotidis EV, Koliakos GG, Baltzopoulos VG et al.
Serum ghrelin, leptin and adiponectin levels before
and after weight loss: comparison of three methods of
treatment – a prospective study. Obes Surg 2006; 16:
1425-32.
(Received April 19, 2007; accepted May 11, 2007)
Obesity Surgery, 17, 2007
969
�
 Andrew Gumbs
Andrew Gumbs