RANDOMIZED CONTROLLED TRIALS
Improvement in Glucose Metabolism After Bariatric Surgery:
Comparison of Laparoscopic Roux-en-Y Gastric Bypass and
Laparoscopic Sleeve Gastrectomy
A Prospective Randomized Trial
Ralph Peterli, MD,* Bettina Wölnerhanssen, MD,† Thomas Peters, MD,‡ Noémie Devaux, MD,*
Beatrice Kern, MD,* Caroline Christoffel-Courtin, MD,‡ Juergen Drewe, MD,§ Markus von Flüe, MD,*
and Christoph Beglinger, MD¶储
Background: The exclusion of the proximal small intestine is thought to
play a major role in the rapid improvement in the metabolic control of
diabetes after gastric bypass.
Objective: In this randomized, prospective, parallel group study, we sought
to evaluate and compare the effects of laparoscopic Roux-en-Y gastric
bypass (LRYGB) with those of laparoscopic sleeve gastrectomy (LSG) on
fasting, and meal-stimulated insulin, glucose, and glucagon-like peptide-1
(GLP-1) levels.
Methods: Thirteen patients were randomized to LRYGB and 14 patients to
LSG. The mostly nondiabetic patients were evaluated before, and 1 week and
3 months after surgery. A standard test meal was given after an overnight
fast, and blood samples were collected before and after food intake in both
groups for insulin, GLP-1, glucose, PYY, and ghrelin concentrations. This
trial was registered in www.clinicaltrials.gov (NCT00356213) before the first
patient was randomized.
Results: Body weight and body mass index decreased markedly (P ⬍ 0.002)
and comparably after either procedure. Excess BMI loss was similar at 3
months (43.3 ⫾ 12.1% vs. 39.4 ⫾ 9.4%, P ⬎ 0.36). After surgery, patients
had markedly increased postprandial plasma insulin and GLP-1 levels,
respectively (P ⬍ 0.01) after both of these surgical procedures, which favor
improved glucose homeostasis. Compared with LSG, LRYGB patients had
early and augmented insulin responses as early as 1-week postoperative;
potentially mediating improved early glycemic control. After 3 months, no
significant difference was observed with respect to insulin and GLP-1
secretion between the 2 procedures.
Conclusion: Both procedures markedly improved glucose homeostasis:
insulin, GLP-1, and PYY levels increased similarly after either procedure.
Our results do not support the idea that the proximal small intestine mediates
the improvement in glucose homeostasis.
(Ann Surg 2009;250: 234 –241)
T
he World Health Organization has described obesity as the
greatest current threat to human health.1 The rising prevalence of
obesity is causing a major health burden in terms of morbidity and
From the *Department of Surgery, St. Claraspital, Basel, Switzerland; †Department of Surgery, University Hospital, Basel, Switzerland; ‡Department of
Medicine, St. Claraspital, Basel, Switzerland; §Department of Clinical Pharmacology, University Hospital, Basel, Switzerland; ¶Department of Research,
Clinical Research Center, University Hospital, Basel, Switzerland; and
㛳Department of Gastroenterology, University Hospital, Basel, Switzerland.
Supported by grants from the Swiss National Science Foundation (3200B0120020 and 320000-118330) and by a grant from Ethicon Endosurgery, USA.
Dr. Ralph Peterli is a consultant to Ethicon Endosurgery.
Reprints: Ralph Peterli, MD, Department of Surgery, St. Claraspital, CH-4016
Basel, Switzerland. E-mail: ralph.peterli@claraspital.ch.
Copyright © 2009 by Lippincott Williams & Wilkins
ISSN: 0003-4932/09/25002-0234
DOI: 10.1097/SLA.0b013e3181ae32e3
234 | www.annalsofsurgery.com
mortality.2 The complications of obesity, especially type 2 diabetes
mellitus (T2D), are placing growing demand on health care resources. Existing medical therapeutic strategies (diet, behavioral
changes, drugs) to achieve and maintain clinically significant weight
loss remain limited.3 Bariatric surgery is currently the only effective
treatment for morbid obesity.3– 6 Laparoscopic Roux-en-Y gastric
bypass (LRYGB) has become the most commonly performed bariatric operation in many parts of the world and has superseded other
restrictive and malabsorptive procedures.4,7 LRYGB results in
greater weight loss than do restrictive procedures (such as gastric
banding) in the absence of clinically significant malabsorption for
macronutrients.3,4,8 Furthermore, dramatic improvements in glycemic control have been observed in subjects with T2D after the
RYGB procedure.3,4,9 In the early postoperative period, many patients achieve normal fasting glucose concentrations before any
substantial weight loss has occurred.10 It has been proposed that
the improvement in glycemic control may be due to changes in
circulating hormones (mainly glucagon-like peptide-1 or 关GLP1兴) from the distal gut. This “hind-gut hypothesis” holds that
diabetes control results from the expedited delivery of nutrients
to the distal small intestine, enhancing hormone release, such as
GLP-1, as a physiologic signal that improves glucose metabolism. This incretin hormone is secreted by L cells of the distal
bowel in response to intestinal nutrients. It stimulates insulin
secretion and suppresses glucagon secretion thereby improving
glucose metabolism.10 –13
An alternative hypothesis is that the positive effects of RYGB
surgery on diabetes depends on the exclusion of the duodenum and
proximal jejunum from the transit of nutrients, possibly preventing
secretion of a putative signal that promotes insulin resistance and
T2D (“fore-gut hypothesis”).14,15
Laparoscopic sleeve gastrectomy (LSG) is the restrictive part
of biliopancreatic diversion duodenal switch and was initially
applied as an isolated operation on superobese patients with
severe comorbidities in a staged concept.16 It is a purely restrictive operation with no malabsorptive effect. Long-term results of
LSG do not exist, but weight loss in the first postoperative years
is promising.17–20 LSG may have the potential to be a dependable
isolated bariatric procedure. In a staged-therapy concept, LSG
seems to be superior to laparoscopic gastric banding as the firststage procedure.21,22 LSG preserves the integrity of the pylorus and
does not include intestinal bypass as part of the technique. Therefore, no significant changes in distal gut hormone release would be
expected.
The purpose of this prospective, randomized study was to
investigate and compare the effects of LRYGB to the effects of
LSG on glycemic control (primarily insulin and GLP-1 release)
in morbidly obese, mostly nondiabetic patients undergoing bariatric surgery.
Annals of Surgery • Volume 250, Number 2, August 2009
�Annals of Surgery • Volume 250, Number 2, August 2009
MATERIALS AND METHODS
Patients
All studies were performed according to the principles of the
Declaration of Helsinki. The Local Research and Ethics Committee
in Basel approved the study. Morbidly obese patients were evaluated
for bariatric surgery by an interdisciplinary team and were included
in the study if they fulfilled the criteria for bariatric surgery in
Switzerland (BMI ⬎40 kg/m2 with comorbidity, age below 60
years, 2 years of unsuccessful conservative treatment, and approval
of surgery by their health insurance). Patients with extensive hiatal
hernias and after previous extensive abdominal surgery were excluded. All patients were informed in detail about the risks and
benefits of each operation, and all gave their written informed
consent. Computer-generated random numbers were used to assign the
type of surgery (LRYGB or LSG), and these were individually written
on cards, then sealed in completely opaque envelopes. All the operations were performed laparoscopically by the same surgeon.
The LRYGB technique included a 150 cm antecolic Roux-limb
with 25 mm circular pouch-jejunostomy and an exclusion of 50 cm of
proximal jejunum. In LSG, the longitudinal resection of the stomach
from the angle of His to approximately 3 to 4 cm orally to the pylorus
was performed using 35 French bougie inserted along the lesser curvature.
Study Design
The study was conducted as a randomized, prospective,
parallel group trial. All patients underwent complete evaluation
before the operation and during follow-up until 3 months postoperatively, including medications, nutritional behavior, anthropometric
and clinical parameters, blood sampling for fasting glucose, triglycerides, and cholesterol, as well as other laboratory tests.
For the meal studies, subjects were admitted to the Clinical
Research Centre before the operation, and at 1 week (8 –10 days)
and 3 months after the operation. On each occasion, an overnight
fast of at least 10 hours preceded insertion of an antecubital vein
catheter for blood collection. After taking the fasting samples, a
liquid test meal (400 kcal) was served to stimulate hormone release
(details of the meal are given in Table 1). Blood was drawn at the
following time points: ⫺15, 0, 15, 30, 45, 60, 120, and 180 minutes
(time 0 corresponded to the start of meal intake, also see Figs. 1, 2, and
3). Samples (10 mL per withdrawal) were collected on ice into EDTA
tubes containing aprotinin at a final concentration of 500 KIU/mL of
blood and a DPP-IV inhibitor; samples were immediately processed to
avoid the breakdown of peptides. After centrifugation at 4°C, plasma
samples were kept frozen at ⫺20°C until analysis.
Hormones
The following hormones were measured: GLP-1, insulin,
PYY, and ghrelin; in addition, glucose concentrations were
determined. GLP-1 was measured with a commercially available
ELISA kit (Linco Research Inc., St. Charles, MO). This kit is for
nonradioactive quantification of biologically active forms of
glucagon-like peptide-1 (ie, GLP-1 关7-36 amide兴 and GLP-1
TABLE 1.
Composition of the Test Meal
200 mL Diabetes Resource Vanille (Novartis, Basel, Switzerland)
Enriched With 50 g Heavy Cream
Nutrients
Protein
15 g
Carbohydrate
24.9 g
Fat
28.1 g
Calories
1054 kJ
© 2009 Lippincott Williams & Wilkins
Metabolic Effect of Bypass or Sleeve
关7-37兴) in plasma and other biologic media. It is highly specific
for the immunologic measurement of active GLP-1 and will not
detect other forms of GLP-1 (eg, 1-36 amide, 1-37, 9-36 amide,
or 9-37 amide). This assay is based, sequentially, on: (1) capture
of active GLP-1 from sample by a monoclonal antibody, immobilized in the wells of a microwell plate, that binds specifically to
the N-terminal region of active GLP-1 molecule, (2) washing to
remove unbound materials, (3) binding of an anti GLP-1-alkaline
phosphatase detection conjugate to the immobilized GLP-1, (4)
washing off unbound conjugate, and (5) quantification of bound
detection conjugate by adding methyl umbelliferyl phosphate, which
in the presence of alkaline phosphatase forms the fluorescent product
umbelliferone. Because the amount of fluorescence generated is directly
proportional to the concentration of active GLP-1 in the unknown
sample, the latter can be derived by interpolation from a reference curve
generated in the same assay with reference standards of known concentrations of active GLP-1. The intra- and interassay variability remained below 9% and 13%, respectively. When using a 100 L plasma
sample, the lowest level of GLP-1 that could be detected by this assay
was 0.25 pmol/L.
PYY was measured with a commercially available kit
(Linco Research Inc). Raised in guinea pigs, the antibody displays 100% cross-reactivity with human PYY1-36 and human
PYY3-36, but no cross-reactivity with human pancreatic
polypeptide, NPY, and unrelated peptides, such as leptin and
ghrelin. 125I-PYY was used as a label; the labeled peptide was
purified by HPLC (specific activity: 302 Ci/g). The lowest
level of PYY that could be detected by this assay was 10 pg/mL
when using a 100 L plasma sample. Intra- and interassay
variability was below 9% and 9%, respectively.
Total ghrelin was measured with a commercially available kit
(Linco Research Inc). The lowest level of ghrelin that can be
detected by this assay is 93 pg/mL, when using a 100 L sample
size. At 1 ng/mL, the intra-assay coefficient of variation was 10.0%,
whereas the interassay coefficient of variation was 14.7%.
Insulin was measured with a commercial radioimmunoassay
(Cisbio international, F-30200 Bagnols, France). The lowest level of
insulin that can be detected by this assay is 4.6 U/mL when using
a 100 L sample. The intra-assay coefficient of variation was
12.2%, whereas the interassay coefficient of variation was 9.0%.
Blood glucose concentrations were measured by a commercial
hexokinase-glucose-6-phosphate-dihydrogenase method (Roche, Basel,
Switzerland).
Statistical Analysis
Data are expressed as mean ⫾ SEM unless indicated otherwise. Descriptive statistics were used for demographic variables
such as age, weight, height, and BMI. Hormones were analyzed by
calculating time courses, area under the curve (AUC), and Cmax.
These parameters were compared by analysis of variance. Whenever
this analysis revealed significant differences, pairwise comparisons
were performed using Tuckey multicomparison test. All statistical
analyses were done using SPSS-for-Windows software (version
14.0). The level of significance was P ⬍ 0.05.
RESULTS
After randomization, 13 patients underwent LRYGB, and 14,
LSG. All procedures were successfully concluded laparoscopically
with no conversion to open surgery. The demographic characteristics of the 2 groups of patients are given in Table 2. Both groups had
similar preoperative body weight and BMI. None of the patients of
the LRYGB group had T2D, whereas 3 patients in the LSG group
had T2D (2 patients were on insulin treatment and 1 of them was on
oral antidiabetic drugs). With the exception of one patient in the
www.annalsofsurgery.com | 235
�Peterli et al
Annals of Surgery • Volume 250, Number 2, August 2009
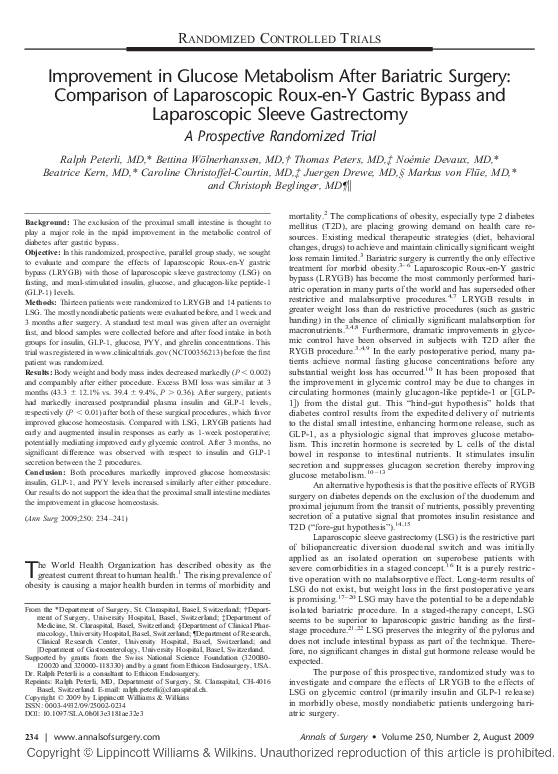
FIGURE 1. Meal-stimulated time courses of GLP-1 (pmol/L), insulin (U/mL), and glucose (mmol/L) in 2 groups of patients
(LRYGB and LSG) before, and 1 week and 3 months after the respective operation. Data are mean ⫾ SEM.
LSG group (who had a normal HOMA Index), all other patients in
both groups had an abnormal HOMA-Index (defined as ⬎3.8,
details given in Table 2), indicating insulin resistance in these
236 | www.annalsofsurgery.com
patients. In the LRYGB group 8 patients had hypercholesterolemia,
and 3 had hypertriglyceridemia; in the LSG group 7 patients had
hypercholesterolemia, and 5 had hypertriglyceridemia.
© 2009 Lippincott Williams & Wilkins
�Annals of Surgery • Volume 250, Number 2, August 2009
Metabolic Effect of Bypass or Sleeve
FIGURE 2. Time courses of ghrelin concentrations (pg/mL) in
response to meal ingestion in 2 groups of patients (LRYGB and
LSG) before, ands 1 week and 3 months after the respective
operation. Data are mean ⫾ SEM.
All patients had a complete evaluation at all time points of the
follow-up. Either procedure was followed by a marked reduction in
body weight and BMI (P ⬍ 0.002) (Table 3). The LRYGB group
lost 25.6 ⫾ 9.5 kg 3 months after the operation, and the LSG group,
21.6 ⫾ 6.0 kg, corresponding to excessive BMI losses of 43.3 ⫾
12.1% and 39.4 ⫾ 9.4%, respectively (P ⬎ 0.36).
Preoperative fasting insulin and GLP-1 levels were similar in
both groups (Tables 3 and 4), but both demonstrated elevated fasting
insulin concentrations and basal insulin resistance as assessed by the
HOMA index (Tables 3 and 4). Postoperatively, fasting insulin
concentrations were reduced in both groups; HOMA indices were
reduced after 1 week, already suggesting a rapid improvement in
glycemic control before any significant weight loss has occurred.
Fasting GLP-1 levels were not significantly different before and
after surgery in either study group (Tables 3 and 4).
Meal-stimulated concentrations of GLP-1, insulin, and glucose before and after the operation are given in Figure 1. The time
courses for GLP-1 document an impaired postprandial GLP-1 response to the test meal, with a subsequently attenuated insulin
response before the operation. One week after surgery, an early and
marked increase in postprandial insulin concentrations was observed
in both the LRYGB and LSG groups. Despite the marked insulin
response, subjects did not experience hypoglycemia or symptoms of
a dumping syndrome after the test meal. An improvement in the
HOMA indices was seen as early as 1 week postoperatively in both
groups, and most subjects were found to be as insulin-sensitive as
lean normal weight subjects 3 months after the operation (Fig. 2).
Two of the 3 patients with manifest diabetes were euglycemic
without medication; one patient with long-lasting T2D showed
significant improvement but was still insulin dependent.
Both groups had a defective GLP-1 response to test meal
intake before the operation. Postoperatively, LRYGB patients had
an exaggerated postprandial GLP-1 response at 1 week postsurgery
(P ⬍ 0.001 vs. preoperative), significantly higher than that of the
LSG group (P ⫽ 0.038 for AUC and 0.016 for Cmax, Fig. 1 and
Table 5). The exaggerated GLP-1 response was unchanged after 3
months in the LRYGB group; in contrast, the GLP-1 response was
further increased in the LSG group and showed a pattern similar to
that of the LRYGB patients, although the AUC was slightly smaller
© 2009 Lippincott Williams & Wilkins
FIGURE 3. HOMA index before, and 1 week and 3 months
after the respective operation in patients with LRYGB (white
bars) versus patients with LSG (gray bars). Data are mean ⫾
SEM.
in the LSG patients (P ⫽ 0.084 for AUC, Fig. 1 and Table 5).
Preoperative fasting PYY levels in the LRYGB group were slightly
higher than those of the LSG groups, but the difference was
statistically not significant. Before surgery, PYY levels did not
significantly increase in response to meal ingestion (Fig. 3), suggesting a defective PYY response. Fasting PYY levels decreased
after surgery in both study groups. Both groups had an exaggerated
postprandial PYY response one week after the operation, which was
slightly less prominent but still present 3 months later (Fig. 3, Table
5). The response pattern and the secretory output were comparable
for both groups, with no significant differences.
Fasting ghrelin levels in the LRYGB group were similar to
those in the LSG group (Tables 3 and 4, not significantly different).
Postoperatively, fasting ghrelin levels decreased significantly in both
groups (P ⬍ 0.001 vs. preoperative values). Multivariate analysis
revealed that there was a significant change in ghrelin secretion
(AUC) after the operation: meal-induced ghrelin release was diminished in both groups P ⬍ 0.001 vs. preoperative, Fig. 4, Table 5).
The reduction in ghrelin secretion in the LSG group was more
prominent than that in the LRYGB group, both at 1 week and 3
months (lower AUC and lower Cmax, Fig. 4, Table 5).
www.annalsofsurgery.com | 237
�Annals of Surgery • Volume 250, Number 2, August 2009
Peterli et al
TABLE 2.
Patient Characteristics at Baseline: Mean ⫾ SD and (Range)
Parameter
Age (yr)
BMI (kg/m2)
Weight (kg)
Systolic bp (mm Hg)
Diastolic bp (mm Hg)
Type 2 diabetes
HbA1c
HOMA-index
Cholesterol (mmol/L)
Triglycerides (mmol/L)
LRYGB n ⴝ 13
LSG n ⴝ 14
P
41.8 ⫾ 10.4 (23.6–53.9)
47 ⫾ 6.4 (39.4–56.9)
131.2 ⫾ 29.3 (98–203)
134.6 ⫾ 15.2 (110–170)
87.7 ⫾ 11.4 (60–100)
0
5.7 ⫾ 0.3
9.1 ⫾ 1.2
4.83 ⫾ 0.9 (3.1–6.2)
1.76 ⫾ 0.8 (0.6–3.43)
37.8 ⫾ 10.4 (28.8–58.9)
45.7 ⫾ 6.7 (39.0–61.0)
125.4 ⫾ 21.9 (88–160)
137.1 ⫾ 17.2 (110–170)
83.9 ⫾ 11.1 (70–110)
3
6.1 ⫾ 1.3
9.1 ⫾ 1.7
5.36 ⫾ 1.3 (3.6–8.4)
1.96 ⫾ 1.5 (0.6–5.4)
0.96
0.88
0.32
0.68
0.91
0.16
0.33
0.95
0.3
0.05
TABLE 3. Body Weight, Fasting Insulin, GLP-1, Glucose, PYY, and Ghrelin Concentrations
Before, and 1 Week and 3 Months Postoperatively After LRYGB: Mean ⫾ SD and (Range)
Parameter
BMI (kg/m2)
Excess BMI loss (%)
Glucose (mmol/L)
Insulin (U/mL)
GLP-1 (pmol/L)
HOMA index
PYY (pmol/L)
Ghrelin (pmol/L)
Preoperative
1 Wk
3 Mo
47.3 ⫾ 6.6 (39.4–56.9)
NA
5.7 ⫾ 0.8
28.3 ⫾ 13.3
1.2 ⫾ 0.4
9.1 ⫾ 1.2
141 ⫾ 66
529 ⫾ 89
44.9 ⫾ 6.3 (36.5–53.6)
11.3 ⫾ 6.9 (4.4–31.2)
5.6 ⫾ 0.7
21.6 ⫾ 5.2
1.1 ⫾ 0.4
6.1 ⫾ 0.7
111 ⫾ 48
275 ⫾ 42
38.1 ⫾ 6.1 (30.6–50.5)
43.3 ⫾ 12.1 (17.8–66.2)
5.1 ⫾ 0.5
14.9 ⫾ 3.7
1.1 ⫾ 0.4
3.4 ⫾ 0.3
115 ⫾ 17
476 ⫾ 56
TABLE 4. Body Weight, Fasting Insulin, GLP-1, Glucose, PYY, and Ghrelin Concentrations
Before, and 1 Week and 3 Months Postoperatively After LSG: Mean ⫾ SD and (Range)
Parameter
BMI (kg/m2)
Excess BMI loss (%)
Glucose (mmol/L)
Insulin (U/mL)
GLP-1 (pmol/L)
HOMA index
PYY (pmol/L)
Ghrelin (pmol/L)
Preoperative
1 Wk
3 Mo
45.7 ⫾ 6.7 (39.0–61.0)
NA
6.3 ⫾ 1.8
37.0 ⫾ 26.1
1.5 ⫾ 1.2
9.1 ⫾ 1.7
115 ⫾ 28
505 ⫾ 63
43.6 ⫾ 6.3 (36.8–57.9)
10.9 ⫾ 4.9 (0–18.1)
5.5 ⫾ 1.9
23.9 ⫾ 15.7
1.3 ⫾ 1.0
6.0 ⫾ 1.4
88 ⫾ 30
284 ⫾ 57
37.9 ⫾ 5.5 (30.4–48.3)
39.4 ⫾ 9.4 (24.0–64.1)
5.4 ⫾ 1.0
24.2 ⫾ 17.3
1.1 ⫾ 0.4
4.0 ⫾ 0.6
97 ⫾ 33
271 ⫾ 56
DISCUSSION
The present study can be summarized as follows: both
LRYGB and LSG were associated with an early and dramatic
improvement in glycemic control, which was present 1 week after
the operations before a significant weight loss had occurred. Our
data support previous findings obtained in patients with RYGB.23–28
The effect observed in our LSG group was, however, unexpected, as
previous studies in patients with gastric banding did not experience
such a dramatic improvement.27,29 A strength of the present study
design was that it was a randomized trial on humans and that there
were not only single measurements of gastrointestinal peptides after
an overnight fast and after meal stimulation but sequential measurements until 3 hours after the stimulation. Both groups were comparable preoperatively, which makes a selection bias unlikely. Based
on previous findings, the LRYGB patients were expected to improve
rapidly (hind-gut hypothesis).10 –13 On the other hand, the improvement in glucose homeostasis in the LSG patients was expected to
238 | www.annalsofsurgery.com
occur at a later stage, being associated with weight loss and caloric
restriction, as the flow of nutrients through the proximal small
intestine is unchanged in this group. The following discussions will
address the potential mechanisms that could be responsible for the
improvement.
Antidiabetic Effects of Both Surgical Procedures
A number of studies have documented that RYGB dramatically ameliorates T2D; the reversal of impaired glucose tolerance
without diabetes was almost universal.3,4,9,23–27,30 In a published
meta-analysis on more than 22,000 bariatric interventions including
989 diabetic patients undergoing RYGB, more than 83% showed
complete remission of their disease.4 Thus, gastric bypass surgery is
a highly effective procedure to reverse T2D; more importantly, the
improvement in glycemic control is documented within a few days
after the operation, at a time before any major weight loss has
occurred.27 The present study confirms and extends these observa© 2009 Lippincott Williams & Wilkins
�Annals of Surgery • Volume 250, Number 2, August 2009
Metabolic Effect of Bypass or Sleeve
TABLE 5. GLP-1, PYY, and Ghrelin Concentrations Expressed as AUC and Cmax Before, and at
1 Week and 3 Months Postsurgery; Comparison of Patients With LRYGB to Patients With LSG.
Data are Mean ⫾ SEM
Parameter
GLP-1
AUC (0–180) (pmol*min/L)
Cmax (pmol/L)
PYY
AUC (0–180) (pg*min/mL)
Cmax (pg/mL)
Ghrelin
AUC (0–180) (pg*min/mL)
Cmax (pg/mL)
1,
2,
3,
4,
5,
6,
7,
8,
significantly
significantly
significantly
significantly
significantly
significantly
significantly
significantly
different
different
different
different
different
different
different
different
Treatment
Preoperative
1 Wk
3 Mo
LRYGB
LSG
LRYGB
LSG
335.1 ⫾ 49.8
332.3 ⫾ 51.9
3.4 ⫾ 0.7
2.5 ⫾ 0.4
1174.5 ⫾ 138.0 1,2
725.7 ⫾ 108.2 1,2
17.0 ⫾ 2.7 1,4
9.2 ⫾ 1.5 1,4
1325.3 ⫾ 175.6 1,3
915.8 ⫾ 121.2 1,3
20.3 ⫾ 3.3 1,5
13.3 ⫾ 1.6 1,5
LRYGB
LSG
LRYGB
LSG
27609 ⫾ 2839
22869 ⫾ 1107
174.8 ⫾ 18.0
148.2 ⫾ 7.2
53534 ⫾ 2983 1
49267 ⫾ 5373 1
389.3 ⫾ 26.8
372.6 ⫾ 55.5 1
43078 ⫾ 4153 1
41520 ⫾ 6625 1
319.8 ⫾ 29.9
315.7 ⫾ 56.5 1
LRYGB
LSG
LRYGB
LSG
9048 ⫾ 1511
89823 ⫾ 9205
566.7 ⫾ 87.2
535.6 ⫾ 59.6
64308 ⫾ 6117 1,6
47379 ⫾ 2326 1,6
394.9 ⫾ 37.9 1
305.3 ⫾ 17.9
73958 ⫾ 8121 1,7
49734 ⫾ 2922 1,7
468.6 ⫾ 52.2 1,8
308.2 ⫾ 18.5
from preoperative, P ⬍ 0.001.
between treatments at 1 wk: P ⫽ 0.038.
between treatments at 3 mo: P ⫽ 0.084.
between treatments at 1 wk: P ⫽ 0.016.
between treatments at 3 mo: P ⫽ 0.024.
between treatments at 1 wk: P ⫽ 0.046.
between treatments at 3 mo: P ⫽ 0.016.
between treatments at 3 mo: P ⫽ 0.014.
tions: a marked amelioration in glycemic control was seen within 8
to 10 days after either of the 2 procedures. The HOMA-Index
(indicating insulin resistance) significantly improved in most subjects; the majority of patients was found to be as insulin-sensitive as
lean normal-weight subjects 3 months after the operation (Fig. 2).
Surprisingly, the LSG-patients showed a similar improvement in
glucose metabolism despite the fact that all 3 diabetic patients
belonged to this group. In 2 of these patients, diabetes resolved
within 3 months after the operation.
What mechanism could explain this rapid and marked reversal of disturbed glucose metabolism? One possibility is that patients
consume very little or no food in the immediate postoperative
period, leaving the insulin-producing cells resting. Starvation alone
is associated with improvement in glycemic control in T2D. A few
days after surgery, patients start to eat again, but smaller meals,
which means that their energy intake is markedly reduced, inducing
a negative energy balance, a condition that further ameliorates
glucose tolerance. This mechanism would apply to both surgical
procedures, LRYGB and LSG. At a later stage a further improvement in glycemic control can be explained by the well-known effect
of weight loss to increase insulin sensitivity.
An alternative explanation, which might act in concert with
the mechanisms described previously, is that changes in gastrointestinal hormone secretion would improve insulin secretion and/or
action. The most likely candidate for an increased insulin response
is GLP-1. Indeed, we did observe a marked increase in GLP-1 (and
insulin) secretion already at 1 week postoperatively. The increase in
GLP-1 secretion cannot be explained by caloric restriction, as
GLP-1 release depends on luminal stimulation by nutrients. Although the increase in both GLP-1 and insulin concentrations was
more apparent in the LRYGB group, it was no longer strikingly
different at 3 months. We infer from these results that the hind-gut
hypothesis does not fully explain the improvement seen in glucose
homeostasis in the early postoperative period. After RYGB surgery,
© 2009 Lippincott Williams & Wilkins
nutrients reach the distal small intestine more rapidly, bypassing the
duodenum. The larger postprandial nutrient delivery induces a
marked and rapid GLP-1 release within 8 to 10 days after the
procedure, an effect that was confirmed in our study. The GLP-1
response was rapid and impressive (although slightly smaller) after
LSG after one week, despite the fact that delivery of nutrients to the
distal gut is not as rapid in this group.
The blunted GLP-1 response observed preoperatively confirms previous findings and may reflect a functional deficiency state
(“GLP-1 resistance”) contributing to poor glycemic control.31–33
After surgery (both bypass and gastric sleeve), it is likely that
different mechanisms act in concert to achieve rapid and improved
glycemic control. The increased GLP-1 response may also act as a
satiety signal, promoting weight loss, but the time course of the
effects suggests that the incretin effect seems to be the initial factor.
Secretion of PYY, another hormone produced in the distal gut
was similarly enhanced after both operations. Similar to GLP-1, the
blunted PYY response observed preoperatively may reflect a functional deficiency state (“PYY resistance”), contributing to poor
appetite control and perhaps insufficient glycemic control. In healthy
subjects, peak concentrations of PYY are obtained postprandially; in
addition, exogenous administration of PYY3-36 induces a dosedependent loss of appetite, both in healthy volunteers and in obese
persons, suggesting that the peptide acts as a satiety factor.34,35
Whether the increase observed both in our LRYGB and LSG
patients contributed to glucose homeostasis is not clear, but the
increased PYY concentrations could have contributed to weight loss.
Again, both surgical procedures produced similar effects on PYY
secretion confirming a recent publication.36
Finally, changes in ghrelin may have contributed to improved
glucose homeostasis, as it has been proposed that gastric bypass
patients’ appetite may be suppressed because ghrelin levels are low
or fail to show the expected rise associated with other forms of
weight loss. Produced in the stomach, ghrelin increases in the fasting
www.annalsofsurgery.com | 239
�Peterli et al
FIGURE 4. Meal-stimulated time courses of PYY (pg/mL) in
2 groups of patients (LRYGB and LSG) before, and 1 week
and 3 months after the respective operation. Data are
mean ⫾ SEM.
state and peaks before a meal, but decreases postprandially.31,37– 40
These actions are consistent with ghrelin acting as a hunger hormone. The present results are in line with this hypothesis, as a
marked reduction was seen in ghrelin concentrations after both
surgical procedures, although the decrease was markedly higher
after LSG than after LRYGB. Ghrelin exerts several diabetogenic
effects (increase in growth hormone, cortisol, and epinephrine; at
pharmacological doses, inhibition of insulin secretion).41,42 Therefore, suppression of ghrelin could have contributed to improved
glucose homeostasis.
Roles of Foregut and Hindgut After LRYGB and LSG
Both operations promoted weight loss and improved glucose
homeostasis, but only LRYGB excluded the intestinal foregut from
digestive continuity. The results of our study do not fully support the
hypothesis that exclusion of the proximal small intestine from
contact with nutrients is a critical component in the mechanism
improving glucose tolerance after RYGB.10,14,15,27 The mechanisms
proposed by the hind-gut hypothesis suggest a rapid increase in
hormones from the distal gut, such as GLP-1, PYY, and neurotensin.
The concept is supported by rat studies, which indicated that
240 | www.annalsofsurgery.com
Annals of Surgery • Volume 250, Number 2, August 2009
gastrojejunal bypass and duodenal exclusion are equally effective in
improving glucose tolerance; both procedures equivalently expedite
nutrient delivery to the hindgut.13,43 Our results in humans are in
contrast to these observations. Previous clinical studies, including a
randomized trial comparing gastrectomy combined with duodenal
exclusion (such as the Roux-en-Y reconstruction) versus gastrectomy combined with preservation of duodenal passage, showed that
exclusion of the duodenum from the passage of food impairs glucose
tolerance in nondiabetic subjects and, furthermore, results in lower
plasma glucose-dependent insulinotropic polypeptide and insulin
levels.44,45 Based on these observations it has been suggested that
duodenal-jejunal exclusion may disrupt the physiologic enteroinsular axis in nondiabetic individuals. In contrast, when gastrectomy
with duodenal exclusion is performed in diabetic patients, the result
is an improvement of diabetes, just as in the case of bariatric
operations with duodenal exclusion.46 – 48 The results of these studies are consistent with the possibility that surgical bypass of the
proximal small intestine reverses a humoral mechanism that originates in the proximal bowel and impairs glucose tolerance in
diabetic individuals. Rubino et al have therefore proposed the
hypothesis that type 2 patients with diabetes are characterized by
having a component of duodenal-jejunal dysfunction.15 The results
of our study only partially support such a hypothesis: LRYGB
patients showed a rapid improvement at an early stage, but the
benefit in glycemic control was similar after both operations.
RYGB surgery reliably decreases body weight. Such surgery
creates a gastrojejunal anastamosis, so that gastric volume is severely restricted and ingested food moves from a small, proximal
stomach pouch to the jejunum, bypassing the remainder of the
stomach and the entire duodenum. One would expect a massive
decrease in body weight induced by RYGB to trigger an elevation of
ghrelin levels; however, RYGB patients in our study had extremely
low plasma ghrelin levels. What causes the unusual ghrelin reduction or lack of ghrelin response to weight loss in most RYGB
patients? Some authors have suggested that the effect of surgery to
reduce ghrelin levels depends on whether the procedure affects the
integrity of the gastric fundus. Adjustable gastric banding and
biliopancreatic diversion (with horizontal gastrectomy) - 2 other
surgical treatments for obesity - leave the fundus in contact with
ingested food, whereas RYGB does not. In several studies, plasma
ghrelin levels were substantially elevated after gastric banding or
biliopancreatic diversion, but not after RYGB.27,37,49 –52 In the
present study, premeal ghrelin levels were substantially decreased
after both operations, although the reduction was significantly more
pronounced after LSG. Postprandial ghrelin responses were not
significantly different from fasting levels, suggesting that nutrient
detection in the stomach is involved in ghrelin regulation. We
believe that the disordered ghrelin response in both groups of
patients is likely due to the exclusion of nutrients from the fundus.
If fluctuations in circulating ghrelin are indeed tied to the perception
of hunger and satiety, a more detailed analysis of the factors that
control plasma ghrelin levels will be useful for clinical applications.
In conclusion, our study showed that both LSG and LRYGB
markedly improved glucose homeostasis: insulin, GLP-1, and PYY
levels increased similarly after either procedure. Our results do not
support the idea that the proximal small intestine mediates the
improvement in glucose homeostasis.
ACKNOWLEDGMENTS
The authors thank the team of the Clinical Research Centre
(Ms. Luisa Baselgia Jeker and Ms. Claudia Bläsi) for expert technical help with these experiments and Ms. Silvia Ketterer and Ms.
Gerdien Gamboni for their work in measuring the hormones.
© 2009 Lippincott Williams & Wilkins
�Annals of Surgery • Volume 250, Number 2, August 2009
Metabolic Effect of Bypass or Sleeve
REFERENCES
1. Kopelman PG. Obesity as a medical problem. Nature. 2000;404:635– 643.
2. Sturm R. Increases in morbid obesity in the USA: 2000 –2005. Public Health.
2007;121:492– 496.
3. Sjöström L, Lindroos A, Peltonen M, et al. Lifestyle, diabetes, and cardiovascular risk factors 10 years after bariatric surgery. N Engl J Med. 2004;
351:2683–2693.
4. Buchwald H, Avidor Y, Braunwald E, et al. Bariatric surgery. A systemic
review and meta-analysis. JAMA. 2004;292:1724 –1737.
5. Sjöström L, Narbro K, Sjostrom CD, et al. Swedish Obese Subjects Study.
Effects of bariatric surgery on mortality in Swedish obese subjects. N Engl
J Med. 2007;357:741–752.
6. Adams TD, Gress RE, Smith SC, et al. Long-term mortality after gastric
bypass surgery. N Engl J Med. 2007;357:757–761.
7. Nguyen NT, Root J, Zainabadi K, et al. Accelerated growth of bariatric
surgery with the introduction of minimally invasive surgery. Arch Surg.
2005;140:1198 –1202.
8. Weber M, Muller MK, Bucher T, et al. Laparoscopic gastric bypass is
superior to laparoscopic gastric banding for treatment of morbid obesity. Ann
Surg. 2004;240:975–982.
9. MacDonald KG, Long SD, Swanson MS, et al. The gastric bypass operation
reduces the progression and mortality of non-insulin-dependent diabetes
mellitus. J Gastrointest Surg. 1997;1:213–220.
10. Cummings DE, Overduin J, Foster-Schubert KE, et al. Role of the bypassed
proximal intestine in the anti-diabetic effects of bariatric surgery 关review兴.
Surg Obes Relat Dis. 2007;3:109 –115.
11. Drucker DJ. Biological actions and therapeutic potential of the glucagon-like
peptides. Gastroenterology. 2002;122:531–544.
12. Holst JJ. The physiology of glucagon-like peptide 1 关review兴. Physiol Rev.
2007;87:1409 –1439.
13. de Paula AL, Macedo AL, Prudente AS, et al. Laparoscopic sleeve gastrectomy with ileal interposition (“neuroendocrine brake”)–pilot study of a new
operation. Surg Obes Relat Dis. 2006;2:464 – 467.
14. Rubino F, Gagner M, Gentileschi P, et al. The early effect of the Roux-en-Y
gastric bypass on hormones involved in body weight regulation and glucose
metabolism. Ann Surg. 2004;240:236 –242.
15. Rubino F, Forgione A, Cummings DE, et al. The mechanism of diabetes
control after gastrointestinal bypass surgery reveals a role of the proximal
small intestine in the pathophysiology of type 2 diabetes. Ann Surg. 2006;
244:741–749.
16. Regan JP, Inabnet WB, Gagner M, et al. Early experience with two-stage
laparoscopic Roux-en-Y gastric bypass as an alternative in the super-super
obese patient. Obes Surg. 2003;13:861– 864.
17. Frezza E. Laparoscopic vertical sleeve gastrectomy for morbid obesity. The
future procedure of choice? Surg Today. 2007;37:275–281.
18. Langer FB, Reza Hoda MA, Bohdjalian A, et al. Sleeve gastrectomy and gastric
banding: effects on plasma ghrelin levels. Obes Surg. 2005;15:1024 –1029.
19. Cottam D, Qureshi FG, Mattar SG, et al. Laparoscopic sleeve gastrectomy as
an initial weight-loss procedure for high-risk patients with morbid obesity.
Surg Endosc. 2006;20:859 – 863.
20. Lee CM, Cirangle PT, Jossart GH. Vertical gastrectomy for morbid obesity in
216 patients: report of two-year results. Surg Endosc. 2007;21:1810 –1816.
21. Peterli R, Wölnerhanssen BK, Peters T, et al. Prospective study of a two-stage
operative concept in the treatment of morbid obesity: primary lap-band
followed if needed by sleeve gastrectomy with duodenal switch. Obes Surg.
2007;17:334 –340.
22. Wölnerhanssen BK, Peters T, Kern B, et al. Predictors of outcome in
treatment of morbid obesity by laparoscopic adjustable gastric banding:
results of a prospective study of 380 patients. Surg Obes Relat Dis. 2008;4:
500 –506.
23. Pories WJ, Swanson MS, MacDonald KG, et al. Who would have thought it?
An operation proves to be the most effective therapy for adult-onset diabetes
mellitus. Ann Surg. 1995;222:339 –350; discussion 350 –352.
24. Schauer PR, Ikramuddin S, Gourash W, et al. Outcomes after laparoscopic
Roux-en-Y gastric bypass for morbid obesity. Ann Surg. 2000;232:515–529.
25. Schauer PR, Burguera B, Ikramuddin S, et al. Effect of laparoscopic Roux-en
Y gastric bypass on type 2 diabetes mellitus. Ann Surg. 2003;238:467– 484;
discussion 484 – 485.
26. Sugerman HJ, Wolfe LG, Sica DA, et al. Diabetes and hypertension in severe
obesity and effects of gastric bypass-induced weight loss. Ann Surg. 2003;
237:751–756; discussion 757–758.
27. le Roux CW, Aylwin SJ, Batterham RL, et al. Gut hormone profiles following
© 2009 Lippincott Williams & Wilkins
28.
29.
30.
31.
32.
33.
34.
35.
36.
37.
38.
39.
40.
41.
42.
43.
44.
45.
46.
47.
48.
49.
50.
51.
52.
bariatric surgery favor an anorectic state, facilitate weight loss, and improve
metabolic parameters. Ann Surg. 2006;243:108 –114.
Maggard MA, Sugarman LR, Suttorp M, et al. Meta-analysis: surgical
treatment of obesity. Ann Intern Med. 2005;142:547–559.
Biertho L, Steffen R, Ricklin T, et al. Laparoscopic gastric bypass versus
laparoscopic adjustable gastric banding: a comparative study of 1,200 cases.
J Am Coll Surg. 2003;197:536 –544; discussion 544 –545.
Dixon JB, Pories WJ, O’Brien PE, et al. Surgery as an effective early
intervention for diabesity: why the reluctance? 关review兴. Diabetes Care.
2005;28:472– 474.
le Roux CW, Welbourn R, Werling M, et al. Gut hormones as mediators of
appetite and weight loss after Roux-en-Y gastric bypass. Ann Surg. 2007;
246:780 –785.
Rodieux F, Giusti V, D’Alessio DA, et al. Effects of gastric bypass and
gastric banding on glucose kinetics and gut hormone release. Obesity (Silver
Spring). 2008;16:298 –305.
Laferrère B, Teixeira J, McGinty J, et al. Effect of weight loss by gastric
bypass surgery versus hypocaloric diet on glucose and incretin levels in
patients with type 2 diabetes. J Clin Endocrinol Metab. 2008;93:2479 –2485.
Degen L, Oesch S, Casanova M, et al. Effect of peptide YY3-36 on food
intake in humans. Gastroenterology. 2005;129:1430 –1436.
Batterham RL, Cohen MA, Ellis SM, et al. Inhibition of food intake in obese
subjects by peptide YY3-36. N Engl J Med. 2003;349:941–948.
Karamanakos SN, Vagenas K, Kalfarentzos F, et al. Weight loss, appetite
suppression, and changes in fasting and postprandial ghrelin peptide-YY
levels after Roux-en-Y gastric bypass and sleeve gastrectomy, a prospective,
double blind study. Ann Surg. 2008;247:401– 407.
Williams DL, Cummings DE. Regulation of ghrelin in physiologic and
pathophysiologic states 关review兴. J Nutr. 2005;135:1320 –1325.
Stanley S, Wynne K, McGowan B, et al. Hormonal regulation of food intake.
Physiol Rev. 2005;85:1131–1158.
Liou JM, Lin JT, Lee WJ, et al. The serial changes of ghrelin and leptin levels
and their relations to weight loss after laparoscopic minigastric bypass
surgery. Obes Surg. 2008;18:84 – 89.
Garcia-Fuentes E, Garrido-Sanchez L, Garcia-Almeida JM, et al. Different
effect of laparoscopic Roux-en-Y Gastric bypass and open biliopancreatic
diversion of Scopinaro on serum PYY and ghrelin levels. Obes Surg.
2008;18:1424 –1429.
Davenport AP, Bonner TI, Foord SM, et al. International Union of Pharmacology. LVI. Ghrelin receptors nomenclature, distribution, and function
关review兴. Pharmacol Rev. 2005;57:541–546.
Murphy KG, Dhillo WS, Bloom SR. Gut peptides in the regulation of food
intake and energy homeostasis. Endocr Rev. 2006;27:719 –727.
Koopmans HS, Sclafani A. Control of body weight by lower gut signals. Int
J Obes. 1981;5:491– 495.
Cummings DE, Overduin J, Foster-Schubert KE. Gastric bypass for obesity:
mechanisms of weight loss and diabetes resolution. J Clin Endocrinol Metab.
2004;89:2608 –2615.
Vella A, Service FJ. Incretin hypersecretion in post-gastric bypass hypoglycemia–primary problem or red herring? J Clin Endocrinol Metab. 2007;92:
4563– 4565.
Tarnoff M, Shikora S, Lembo A, et al. Chronic in-vivo experience with an
endoscopically delivered and retrieved duodenal-jejunal bypass sleeve in a
porcine model. Surg Endosc. 2008;22:1023–1028.
Cohen RV, Schiavon CA, Pinheiro JS, et al. Duodenal-jejunal bypass for the
treatment of type 2 diabetes in patients with body mass index of 22–34 kg/m2:
a report of 2 cases. Surg Obes Relat Dis. 2007;3:195–197.
Rodriguez-Grunert L, Galvao Neto MP, Alamo M, et al. First human
experience with endoscopically delivered and retrieved duodenal-jejunal
bypass sleeve. Surg Obes Relat Dis. 2008;4:55–59.
Leonetti F, Silecchia G, Iacobellis G, et al. Different plasma ghrelin levels
after laparoscopic gastric bypass and adjustable gastric banding in morbid
obese subjects. J Clin Endocrinol Metab. 2003;88:4227– 4231.
Stoeckli R, Chanda R, Langer I, et al. Changes of body weight and plasma
ghrelin levels after gastric banding and gastric bypass. Obes Res. 2004;12:
346 –350.
Frühbeck G, Diez-Caballero A, Gil MJ, et al. The decrease in plasma ghrelin
concentrations following bariatric surgery depends on the functional integrity
of the fundus. Obes Surg. 2004;14:606 – 612.
Hanusch-Enserer U, Cauza E, Brabant G, et al. Plasma ghrelin in obesity
before and after weight loss after laparoscopical adjustable gastric banding.
J Clin Endocrinol Metab. 2004;89:3352–3358.
www.annalsofsurgery.com | 241
�
 Ralph Peterli
Ralph Peterli