REVIEW
Hyperinflation and its management in COPD
Luis Puente-Maestu 1
William W Stringer 2
1
Hospital General Universitario
Gregorio Marañón, Servicio de
Neumología, Madrid, Spain; 2 Los
Angeles Biomedical Research Institute
at Harbor-UCLA Medical Center;
1000 West Carson Street, Bin 400;
Torrance, CA 90509, USA
Abstract: Chronic obstructive pulmonary disease (COPD) is characterized by poorly
reversible airflow limitation. The pathological hallmarks of COPD are inflammation of the
peripheral airways and destruction of lung parenchyma or emphysema. The functional consequences of these abnormalities are expiratory airflow limitation and dynamic hyperinflation,
which then increase the elastic load of the respiratory system and decrease the performance
of the respiratory muscles. These pathophysiologic features contribute significantly to the
development of dyspnea, exercise intolerance and ventilatory failure. Several treatments
may palliate flow limitation, including interventions that modify the respiratory pattern
(deeper, slower) such as pursed lip breathing, exercise training, oxygen, and some drugs.
Other therapies are aimed at its amelioration, such as bronchodilators, lung volume reduction surgery or breathing mixtures of helium and oxygen. Finally some interventions, such
as inspiratory pressure support, alleviate the threshold load associated to flow limitation. The
degree of flow limitation can be assessed by certain spirometry indexes, such as vital capacity
and inspiratory capacity, or by other more complexes indexes such as residual volume/total
lung capacity or functional residual capacity/total lung capacity. Two of the best methods
to measure flow limitation are to superimpose a flow–volume loop of a tidal breath within a
maximum flow–volume curve, or to use negative expiratory pressure technique. Likely this
method is more accurate and can be used during spontaneous breathing. A definitive definition
of dynamic hyperinflation is lacking in the literature, but serial measurements of inspiratory
capacity during exercise will document the trend of end-expiratory lung volume and allow
establishing relationships with other measurements such as dyspnea, respiratory pattern,
exercise tolerance, and gas exchange.
Keywords: COPD, flow limitation, dynamic hyperinflation, treatment, exercise
Introduction
Correspondence: Luis Puente-Maestu
Hospital General Universitario Gregorio
Marañón, Servicio de Neumología,
c/- Doctor Ezquerdo 46, 28007 Madrid,
Spain
Tel +34 91 586 8336
Fax +34 91 586 8018
Email lpuente.hgugm@madrid.salud.org
Chronic obstructive pulmonary disease (COPD) is defined as a disease state characterized
by poorly reversible airflow limitation and loss of pulmonary capillary bed. It is usually
progressive and associated with abnormal inflammatory responses in the lung (Pauwels
et al 2001). Chronic inflammation is a predominant feature of COPD and involves
the airways (Saetta et al 2001), lung parenchyma (Saetta et al 1999), and pulmonary
vasculature (Peinado et al 1999). It is caused by exposure to inhaled noxious particles
and gases present in tobacco smoke (Von Essen et al 1995; Salvi et al 1999) and
likely in other air pollutants that may be inhaled during breathing. Macrophages,
T lymphocytes (predominately CD8+), and neutrophils are increased numerically as
well as activated (Pesci et al 1998), this results in the release of a variety of mediators
(Keatings et al 1996; Mueller et al 1996; Yamamoto et al 1997; Beeh et al 2003) that
are believed to be capable of unbalance the protease-antiprotease equilibrium (Gottlieb
et al 1996; Stockley et al 1999) and damage lung structures (Liu et al 1999; Shapiro
and Senior 1999).
The pathological hallmarks of COPD are inflammation of the peripheral airways
and destruction of lung parenchyma or emphysema (Thurlbeck 1991). The functional
International Journal of COPD 2006:1(4) 381–400
© 2006 Dove Medical Press Limited. All rights reserved
381
�Puente-Maestu and Stringer
consequence of these abnormalities is expiratory airflow limitation. Since the determinants of expiratory flow through the
airways are both the driving alveolar pressure that promotes
flow (elastic recoil of the lung) and the opposing resistance
of the airways, the reduction in flow occurring in COPD is
defined more accurately as airflow limitation rather than airflow obstruction, since both loss of elastic recoil and increase
in airway resistance play an important role (Pride and Green
1997). Emphysema will contribute to the airflow limitation
by reducing the elastic recoil of the lung through parenchymal
destruction, as well as by reducing the elastic load applied to
the airways through destruction of alveolar attachments. On
the other hand, inflammation of the peripheral airways will
contribute to the airflow limitation by increasing the thickness
of the airway wall which, together with fibrosis and smooth
muscle hypertrophy, may cause airway narrowing (Thurlbeck
1985). The role of mucus hypersecretion in the development of
chronic airflow limitation is still controversial (Peto et al 1983;
Vestbo et al 1996).
Expiratory flow limitation and dynamic hyperinflation (DH)
are clinical and pathologic concepts that have been present for
well over 100 years. Recent developments have revitalized
the interest on this crucial psychopathological consequence of
obstructive disease. In accordance with this renewed interest,
a provocative hypothesis has been put forward recently that
proposes that the transition from peripheral airways disease to
COPD follows three pathophysiological stages defined by the
severity of expiratory flow limitation: In Stage I, closing volume
eventually exceeds the functional residual capacity (FRC); in
Stage II tidal volume expiratory flow limitation (EFL) develops;
and in Stage III, DH increases to a point that produces dyspnea
and exercise limitation. The presence of airway closure (Stage
I) and EFL (Stage II) may promote peripheral airway injury
and accelerate the abnormalities of lung function (Milic-Emili
2004).
Pathophysiology of dynamic
hyperinflation
Nonmuscular factors
The respiratory system (ie, the combined elastic recoil of
the lung and chest wall) is an elastic structure able to change
its shape and volume in order to breathe the necessary air
in, and the alveolar gas out, to sustain the amount of gas
exchange needed to match metabolic needs. Under normal
physiological conditions the respiratory muscles provide the
power to produce such changes in volume. For a given change
in pleural pressure generated by the respiratory muscles,
the attainable end-inspiratory and end-expiratory volumes
are determined by the passive pressure–volume (P–V)
relationship of the respiratory system (Figure 1) (Mead et al
1967; Agostoni and Hyatt 1986). The P–V behavior of the
respiratory system is distinctly sigmoid (Figure 1) since the
respiratory system is most compliant between 20% to 80%
120
Volume (% VC)
100
(normal)
(airways narrowing)
(emphysema)
80
60
FRC
40
20
−40
0
−30
−20
−10
0
10
20
30
40
50
Elastic recoil pressure ( cm H O)
2
Figure 1 Pressure volume relationship of the passive respiratory system. Lower and upper boundaries of the elastic recoil pressure–volume relationship of the respiratory
system in healthy subjects (---), in patients with narrowed airways (—), and in patients with loss of lung elastic recoil (·····). The loops represent tidal breathing at rest (—)
and during exercise (·····).
Abbreviations: FRC, functional residual capacity;VC, vital capacity.
382
International Journal of COPD 2006:1(4)
�Hyperinflation in COPD
of the vital capacity (VC) (Mead et al 1967; Agostoni and
Hyatt 1986). To state this in a clearer way, the elastic work
of breathing is minimized by maintaining tidal volume within
the 20%–80% of the VC range. In COPD there are different
forms and degrees of damage to the alveolar wall resulting in
pathophysiological changes in the lung elastic recoil. These
changes might reduce the amount of pressure required to
achieve a specific change in volume (Cherniack et al 1963;
Saksena and Burrows 1966), or simply shift the normal
relationship upwards near passive FRC (Figure 1) (Sharp
et al 1968). There is limited information about passive
elastic recoil characteristics of the lung and chest wall during exercise, but at least in healthy subjects, they remain
essentially unchanged, or decrease slightly (Stubbing
et al 1980; Younes and Kivinen 1984). Therefore total lung
capacity (TLC) does not change significantly during physical activity either in normal subjects or in COPD patients
(Stubbing et al 1980).
While the P–V relationship determines the attainable
volume extremes for a given muscular pressure, the actual
volume change in a given amount of inspiratory or expiratory time depends on the pressure–flow (P–F) relationship,
which is highly dependent on the airways resistance (in a
linear system, the volume at the time tx [Vtx] is given by
the expression
Vtx = P·C·(1–e-tx/RC)
where P is the pressure applied, C the compliance of the
system, tx the time elapsed, and R the resistance. The product RC is the time constant, which determines the speed of
the change), as can be seen in Figure 2. During inspiration,
even when inspiratory resistances are high, flow down the
airways can be increased by increasing the force of inspiratory
muscle contraction up to its maximum capacity (Younes and
Riddle 1981). The same is true during expiration at relative
low pressures, but during forced expiration in both normal
and COPD, increments in alveolar pressure (generated by
increasing muscle effort) produce progressively smaller
increments in expiratory flow, until flow ultimately reaches
a plateau (Figure 3) where it is independent of any increase
of driving pressure (Hyatt and Wilcox 1963). This phenomenon is called flow limitation and it seems to be related to
the dynamic compression of the intra-thoracic airways at a
segment progressively distal as lung volume decreases (Green
and Pride 1997). The resulting increase in airways resistance
offsets the pressure generated by the additional increase in
muscular effort, and therefore expiratory flow is actually
1.5
Volume (I)
1.0
Normal resistance
Increased resistance
0.5
0.0
0
1
2
3
Time (S)
Figure 2 Effects of time and resistance on the change in expiratory volume. Rates of changes of volume after a similar given change of alveolar pressure in a subject with
normal respiratory system resistance (—) and a resistance 3 times greater (---) such as in COPD, assuming a constant compliance. Note the marked effect of resistance on
the volume change, particularly when the available time is shortened.
Abbreviations: COPD, chronic obstructive pulmonary disease.
International Journal of COPD 2006:1(4)
383
�Flow
Puente-Maestu and Stringer
+
−
+
Pleural pressure
Normal
COPD
−
Figure 3 Iso-volume pressure-flow relationship. Schematic representation of the pressure-flow relationship in a healthy (normal) subject and a patient with COPD, showing
the effect of the increased expiratory resistance upon the maximum expiratory flow and in both cases the independence of the maximum flow from the pleural pressure.
Copyright © 1986. Modified with permission from Pride NB, Macklem PT. 1986. Lung mechanics in disease. In: Fishman AP (ed). Handbook of physiology, Section 3,Volume III,
Part 2: The respiratory system. Bethesda MD: American Physiological Society, pp 659–92.
Abbreviations: COPD, chronic obstructive pulmonary disease.
largely independent of muscle effort and is determined by
the respiratory system elastic recoil. Elastic recoil of the
system is proportional to lung volume and the expiratory
airways conductance (ie, the inverse of resistance) (Hyatt
1983). Respiratory mechanics in COPD are characterized by
both elevated inspiratory and expiratory resistance to airflow
(McGregor and Becklake 1961; Citterio 1981; Aldrich et al
1989). An increased inspiratory airflow resistance can be
compensated by augmenting the activation of the inspiratory muscles (Im Hof et al 1986), but the increased expiratory resistance, together with the reduced lung elastic recoil
present in these patients, further limits expiratory flow (Hyatt
1961). This is physiologically much more deleterious because
expiration is primarily effort independent (Figure 3), and cannot be compensated by increasing expiratory muscle effort
(Poon et al 1987). The consequence in COPD is that the time
needed for lung units to empty their volume and achieve their
passive equilibrium point is significantly increased and many
of them do not reach their relaxation volume before a new
inspiration is initiated. As a result, part of the gas that would
have been expired in a normal lung remains “ trapped” (ie,
more gas remains inside that what would be if those units
were not altered) and the alveolar pressure at the end of the
expiration is higher than the atmospheric pressure (intrinsic
PEEP) (Pride and Macklem 1986; Younes 1991). In young
healthy subjects RV is about 25% of the TLC, and FRC is
about 50% of the TLC (Stocks and Quanjer 1995). In older
384
healthy subjects, RV and FRC are about 30% and 55% of
TLC respectively (Stocks and Quanjer 1995). In COPD,
values of RV and FRC are increased to values as high
as 70% and 85% of the TLC, respectively (Fishman et al
2003). Since tidal breathing is performed at FRC, COPD
must breathe at volumes that are very close to TLC where
the system is much less distensible (Figure 1).
During exercise minute ventilation must increase to meet
the increased metabolic demands. This is achieved by increasing both the tidal volume (VT) and the respiratory frequency
(fR), what means that the expiratory time necessary to reach
passive FRC or below is reduced. In normal young subjects
expiratory flow is fast enough to decrease end-expiratory
lung volume (EELV) up to 0.5–1L below the resting FRC
with increasing work. This is due to the activation of expiratory muscles (Pride and Macklem 1986; Henke et al
1988). The decreased EELV not only allows increasing
VT within the most compliant part of the P–V relationship,
but also has a beneficial inspiratory effect because, as the
expiratory muscles relax, the passive tendency of the respiratory system below FRC is towards inspiration. In older
subjects, EELV also decreases during moderate exercise,
but thereafter, tends to increase back to near resting levels
(Johnson et al 1991). In COPD, due to the increased flow
limitation, more and more units are unable to empty their
gas as expiratory time decreases when the respiratory rate
increases, and EELV typically rises (Figures 1 and 4) (Hyatt
International Journal of COPD 2006:1(4)
�Hyperinflation in COPD
B
Flow
Flow
A
Volume
Volume
Rest
Exercise
IC
Rest
Exercise
IC
Figure 4 Maximum and tidal flow-volume curves in subjects with and without flow limitation. In this figure it can be seen an schematic representation of the spontaneous
flow-volume curves generated at tidal volume at rest (inner dotted line ····) and peak exercise (dashed line ----) compared with the maximum flow volume curve in a
subject without flow limitation able to reduce its end-expiratory lung volume (Panel A) and a flow-limited COPD patient with dynamic hyperinflation (Panel B).
Abbreviations: COPD, chronic obstructive pulmonary disease; IC, inspiratory capacity.
1961; Grimby et al 1968; Potter et al 1971; Dodd et al 1984;
Pride and Macklem 1986; Babb et al 1991; Younes 1991;
Yan et al 1997; Diaz et al 2000; O’Donell et al 2001; Oga
et al 2002, 2003; O’Donnell and Webb 2003; Puente-Maestu
et al 2005) in spite of expiratory muscles activity (Dodd et al
1984; Younes 1991). This temporary increase in EELV in
COPD above its baseline (admittedly already elevated) value
is termed DH. The extent of DH depends on the degree of
expiratory flow limitation, the prevailing ventilation, the
breathing pattern for a given ventilation, and is inversely
related to the level of resting lung hyperinflation (O’Donnell
et al 2001; Puente-Maestu et al 2005).
Muscle function
To move the air into the alveoli, sufficient force must be
exerted by the respiratory muscles to expand the lungs and
the chest wall. In addition, respiratory muscles must overcome the resistance and inertia in the system so that air will
flow into the airways. This force is provided by the respiratory muscles and, thus, breathing is the results of their cyclic
activation. Whether the net force is inspiratory or expiratory
will depend on the balance between the pressure generated by
the muscles and the elastic recoil of the respiratory system.
The maximum inspiratory and expiratory pressures that the
respiratory muscles are able to generate are related to several
factors such as age (Black and Hyatt 1969), muscle training
International Journal of COPD 2006:1(4)
(Leith and Bradley 1976), the integrity of the inervation (Gross
et al 1980) and, more important for the present discussion, of
the length and shape (usually termed as “configuration”) of
the respiratory muscles, and particularly of the diaphragm
(Marshall 1962). According to the Laplace’s relationship (the
Laplace relationship establishes the relationship between the
pressure generated across a curved surface “P”, the tension of
the surface “T” and its radius “r”: P = T/r), the less curved a
surface is, the lower the pressure difference created across it.
Thus at high lung volumes, a given neural output would be
likely to cause less change in trans-diaphragmatic pressure
than at low lung volumes. Furthermore, inspiratory muscles
are able to generate less pressure for a given neural input
because of their length–tension relationship (Kim et al 1976;
Similowski et al 1991; Polkey et al 1998). The ability of the
respiratory muscles to sustain a given level of pressure output (endurance) is defined by its pressure time index (PTI)
(McGregor and Becklake 1961; Bellee and Grassino 1982, 1983)
PTI = (Pimus/MIP) × (Ti/Ttot) × 100
(1)
Where “ Pimus” is the inspiratory muscular pressure needed
to achieve a certain displacement of the respiratory system,
“ MIP” is the maximum inspiratory pressure, “ Ti” the
inspiratory time and “Ttot” the total respiratory time. Thus
the PTI is determined to a considerable degree by how high
MIP is, and the fraction of MIP required to sustaining a given
VT. MIP decreases as lung volume increases, while maximum
385
�Puente-Maestu and Stringer
expiratory pressure changes in the opposite direction (Agostoni
and Hyatt 1986), therefore at high volumes a greater fraction
of maximum effort is required to generate the same pressure.
Paradoxically, thus, while flow limitation is primarily an expiratory phenomenon, its consequences are mainly suffered
by the inspiratory muscles because expiratory muscles cannot appreciably increase flow (Figures 3) (Hyatt 1961, 1983;
Hyatt and Wilcox 1963; Pride and Macklem 1986; Green and
Pride 1997) to force the emptying of the lungs. In consequence
the volume at which the respiratory system has to operate is
increased (Hyatt 1961; Grimby et al 1968; Potter et al 1971;
Dodd et al 1984; Pride and Macklem 1986; Babb et al 1991;
Younes 1991; Yan et al 1997; Diaz et al 2000; O’Donnell et al
2001; Oga et al 2002, 2003; O’Donnell and Webb 2003; PuenteMaestu et al 2005) and hence the elastic work needed for a given
displacement of the thorax (Figure 1 and 4) (Cherniack et al
1963; Saksena and Burrows 1966; Mead et al 1967; Sharp et al
1968; Younes and Kivinen 1984; Agostoni and Hyatt 1986).
Second inspiratory muscles have to generate a substantial inspiratory pressure (intrinsic PEEP) before inspiratory airflow
can occur. PEEP behaves actually as an inspiratory threshold
load (Pepe and Marini 1982; Pride and Macklem 1986; Haluszka
et al 1990; Younes 1991), and finally, as we have seen above,
at high lung volume efficacy of respiratory muscles as pressure
generators is greatly reduced (Marshall 1962; Kim et al 1976;
Similowski et al 1991; Polkey et al 1998).
Clinical consequences of dynamic
hyperinflation
Exercise limitation
Patients with COPD characteristically show a poor exercise
performance which is manifested as marked reduction in
peak oxygen uptake and decreased endurance to submaximal
levels of exercise (Table 1) (Gallagher 1994; Casaburi et al
1999; O’Donnell and Webb 2003). The origin of this poor
exercise tolerance is multifactorial and includes abnormal lung
mechanics, impaired pulmonary gas exchange, destruction of
the pulmonary vascular bed, impaired cardiac function and
peripheral muscle dysfunction (Gallagher 1994; Casaburi
et al 1999; O’Donnell and Webb 2003). Dynamic hyperinflation has a detrimental impact on exercise tolerance via
three important physiopathological mechanisms. The relatively rapid shallow breathing pattern in COPD compared
with healthy subjects, reflects the mechanical constraints
on tidal volume expansion, which has an exaggerated
386
Table 1 Main clinical consequences of dynamic hyperinflation
Exercise limitation and dyspnea
Hypoventilation during exercise
Hypercarbic respiratory failure during exacerbations
Hypercapnia during exercise
Cardiac dysfunction during exercise
Weaning failure
Hypotension and barotraumas during mechanical ventilation
Independent risk factor for survival in COPD subjects
Reduced improvement with exercise training
frequency-dependency in COPD, fR increases with exercise
in COPD up to a maximum of about 25–35min-1 (Diaz
et al 2000; Nield et al 2003; Puente-Maestu et al 2005).
At increased respiratory rates, the inversely proportional
decrease in expiratory time, even though there is a slight
reduction of Ti/Ttot to 0.40–0.45 (Diaz et al 2000; PuenteMaestu et al 2005), and as result of the decreased expiratory
time further DH ensues. When EELV reaches approximately
0.5L tidal volume, ventilation reaches a plateau (or even a
slight decreases), exercise soon stops (Figure 5) (O’Donnell
et al 2001; Puente-Maestu et al 2005). This encroachment
of tidal volume not only hampers the ventilatory response to
the metabolic load of exercise, it contributes to reducing the
efficiency of ventilation (ie, increases the dead space) as well
(Gallagher 1994). This effect, together with the augmented
mechanical impedance of the respiratory system results in
an increased work and O2 cost of breathing at any given
metabolic load compared with age-matched healthy controls,
(Roussos et al 1982; Donahoe et al 1989; Shindoh et al 1994;
Mannix et al 1999; Takayama et al 2003). In one study this
additional oxygen cost has been found to be as much as 40%
of the total oxygen uptake (Levison and Cherniack 1968).
Dyspnea
Dyspnea is believed to be the unpleasant awareness of the
respiratory muscle effort. As it was discussed above DH both
increases the pressure changes needed to achieve a given tidal
volume and decreases the ability of the respiratory muscles
to generate this pressure (Marshall 1962; Kim et al 1976;
Similowski et al 1991; Polkey et al 1998). This then increases
the amount of pressure needed to achieve a certain tidal volume
with respect to the maximum pressure (Killian et al 1992). The
change in lung mechanics during exacerbation of COPD has
been show to be directly related to dyspnea during spontaneously breathing. The improvement in operating lung volumes
(ie, increase in inspiratory capacity [IC]) as the exacerbation
International Journal of COPD 2006:1(4)
�Minute ventilation ( l·min−1)
Hyperinflation in COPD
50
50
40
40
30
30
20
20
10
10
0
10
20
30
40
%TLC
100%
0
0%
100%
90%
90%
80%
80%
70%
70%
60%
60%
50%
50%
40%
10
20
30
40
−1
Respiratory rate (min )
40%
0%
20%
40%
60%
80%
100%
EILV
EELV
20%
40%
60%
80%
100%
Work rate (% max)
Figure 5 Tidal volume encroachment by dynamic hyperinflation in COPD. In this figure the effects of respiratory rate and work rate on the end-inspiratory (EILV),
end-expiratory lung volume (EELV), tidal volume (ie, EILV–EELV) and minute ventilation in subjects with severe COPD is displayed. While EILV increases with increasing
respiratory rate from 20 to 30min-1 (lower left panel), so does EELV resulting in an almost constant (encroached) tidal volume. At respiratory rates higher than 30, though,
EILV does not increase any more , however, EELV further increases resulting in a reduced tidal volume and even a drop in ventilation (left upper panel) at respiratory rates
higher than 35min-1. In the right lower panel we can see how during progressive exercise tidal volume also decreases at high intensity due again to increase in EELV without
parallel increase in EILV (Constructed with data from Puente-Maestu et al 2005).
Abbreviation: COPD, chronic obstructive pulmonary disease; EELV, end-expiratory lung volume; EILV, end-inspiratory lung volume; TLC, total lung capacity.
resolves is correlated to symptomatic improvement and
reductions in dyspnea (Parker et al 2005; Stevenson et al
2005). While COPD patients do not usually stop exercise
at higher rates of perceived dyspnea than normal subjects,
the ratio of symptoms to the metabolic load and minute
ventilation are usually increased (Killian and Jones 1994;
Hamilton et al 1996). In these patients there exists a close
correlation between breathlessness during exercise and DH
(O’Donnell et al 1993; Eltayara et al 1996; Puente-Maestu et
al 2005; Vogiatzis et al 2005). In a recent study, arm exercise
in COPD has been found to produce DH as well (Gigliotti
et al 2005).
Hypoventilation/hypercapnia
The increase in inspiratory and expiratory airway resistance
characteristic of COPD would cause only minor problems
in ventilatory function (ie, for the respiratory muscles) if
the disease, through expiratory flow limitation did not cause
dynamic hyperventilation, and its corollaries that include
increased elastic recoil, encroached tidal volume, the threshold load imposed by intrinsic PEEP, and the changes in the
configuration of the thorax that greatly reduce their ability
to generate pressure. When COPD patients with expiratory
flow-limitation need to increase their respiratory rate to
International Journal of COPD 2006:1(4)
increase minute ventilation, there is potential for inspiratory
muscle failure due to DH (Table 1). During exacerbations,
the inflammatory process, the ventilation/perfusion (V’A/Q’)
mismatching, increased airflow resistance, and DH, expose
the respiratory muscles to the risk of fatigue, eventually
leading to ventilatory pump failure and hypercapnia (Rossi
et al 1997). DH is one of the major mechanisms involved
in the development of hypercapnia and (secondarily hypoxemia) during exercise in COPD patients (Diaz et al 2000;
O’Donnell et al 2002).
Cardiac dysfunction
Lung hyperinflation and excessive expiratory muscle recruitment can impair venous return and reduce right ventricular
preload in COPD (Mahler et al 1984; Miller, Pegelow, et al
2005). Moreover, large intrathoracic pressure swings generated during exercise to overcome the increased elastic and
resistive loads may result in left ventricular dysfunction
(increased left ventricular afterload) (Oswald-Mammosser
et al 1991; Montes de Oca et al 1996). Right ventricular
afterload during exercise is also increased because of the
increased pulmonary vascular resistance associated with
breathing at lung volumes close to TLC (Ranieri et al 1996;
Oswald-Mammosser et al 1998).
387
�Puente-Maestu and Stringer
Weaning failure
The incidence of EFL was very high in a small sample of
patients with COPD receiving invasive mechanical ventilation for acute respiratory failure. In this series IC was lower in
patients who failed weaning than those who were successfully
weaned (Alvisi et al 2003).
Hypotension and barotrauma in the
mechanical ventilated patient
Dynamic hyperinflation is a potential cause of hypotension
and barotrauma in mechanically ventilated patients with EFLs
(Table 1). DH should be minimized by the use of bronchodilators and appropriately setting minute ventilation (higher tidal
volumes, slower respiratory rate, higher I:E ratio) to maximize
expiratory time (Schumaker et al 2004).
Exercise training
Most rehabilitation programs are based on constant-load
exercise (CLE) training, consisting of sustained exercise for
30–40min (ACCP/AACVPR 1997). Generally, high-intensity
training is argued to be needed for the improvement of exercise capacity (Casaburi et al 2001). Although patients with
moderately severe COPD (mean forced expiratory volume in
one second [FEV1] >45% predicted) can tolerate high levels
(80%) of their peak tolerance for several minutes (Neder
et al 2000), more severe disease (FEV1 <45% predicted)
are unable to tolerate such high exercise intensities for long
periods of time (Maltais et al 1997). Together with peripheral muscle dysfunction, the major factor that limit exercise
tolerance in these patients is the development of DH, and
the concurrent mechanical constraints on ventilation that
contribute importantly to perceived respiratory discomfort
(Diaz et al 2000; Puente-Maestu et al 2005). Dynamic
hyperventilation is evident even with short exercise bouts
in interval training (Vogiatzis et al 2004). In one study,
a correlation was found between resting hyperinflation
(measured as RV/TLC%) and the increase in endurance time
after 8 weeks of leg muscle rehabilitation (Puente-Maestu
et al 2003). In another study, IC was found as a significant
predictor of the long term effects after a rehabilitation program, but in a multiple logistic regression model, only pressure of carbon dioxide (PaCO2) was identified as predictor
for the maintenance of improvement in health-related quality
of life over one year (Nishiyama et al 2005).
Survival
Certain variables closely linked to DH (O’Donnell et al
1993, 2001, 2002; Diaz et al 2000; Marin et al 2001) such
388
as exercise capacity (maximal oxygen uptake) (Gerardi et al
1996; Bowen et al 2000; Myers et al 2002; Hiraga et al 2003;
Oga et al 2003) or 6 minute walking distance (Pinto-Plata
et al 2004), dyspnea (Celli et al 2004), and oxygen desaturation (Nishimura et al 2002; Hiraga et al 2003; Tojo et al 2005)
during exercise have been show to be powerful predictors of
survival in COPD patients (Table 1). A recent study of 689
COPD patients, with a mean follow up of 34 month, showed
that the IC/TLC was an independent risk factor for mortality
in subjects with COPD (Casanova et al 2005). Using the criterion of IC/TLC <25% with a mean follow up period of 34
months, the adjusted hazard ratio for death of any cause was
1.97 and 2.04 for death caused by acute respiratory failure
(Casanova et al 2005). In another study RV/TLC was also
a prognostic factor for survival at 5 years but not independent of age, FEV1, and arterial oxygen pressure at maximal
exercise (Tojo et al 2005).
Therapeutic interventions
directed to ameliorate dynamic
hyperinflation
The treatment of flow limitation and DH has a long history
that goes back as far as the 19th century, but the recent recognition of the importance of DH has modified the target
physiological variables that we use to evaluate the therapeutic
interventions, such as bronchodilators or rehabilitation, and
has led to a renewed interest in specific treatments such as
the lung volume reduction surgery (LVRS). In this section
we will discuss those therapies grouped according their target
physiological variable.
Treatments that primarily
decrease respiratory rate and
increase VT
Pursed-lip breathing
Pursed-lip breathing (PLB) (Barach et al 1995) is aimed
to reduce breathing frequency and to diminish the impact
of intrinsic PEEP on respiratory muscles. PLB produces a
substantial increase in VT along with a reduced ventilatory
rate and minute ventilation (Thoman et al 1966; Mueller
et al 1970; Bianchi et al 2004). There is a direct relationship
between the efficacy of PLB in reducing dyspnea and the
effect on respiratory rate (Mueller et al 1970). This technique is able to increase expiratory airways pressure thus
inhibiting expiratory airways collapse (Ingram et al 1967). It
appears that patients that do not adopt PLB instinctively did
International Journal of COPD 2006:1(4)
�Hyperinflation in COPD
not assume it naturally for long periods of time even when
properly taught (Tiep et al 1986). In a recent study imposed
PLB did not improved 6 minute-walking distance, but improved the rate of dyspnea recovery to basal levels (Garrod
et al 2005). In another study, PLB reduced respiratory rate in
patients with COPD during exercise on a cycle-ergometer,
but the effect of imposed PLB on dyspnea were variable and
related to the change that it promoted in the tidal volume and
EELV (Spahija et al 2005).
Peripheral muscle training
A number of studies have shown that leg training decreases
respiratory rate during exercise (Cassaburi et al 1997; PuenteMaestu et al 2000; Vogiatzis et al 2002; Gigliotti et al 2003;
Ruiz de Oña et al 2004), and three previous studies have
directly analyzed the impact of leg training on DH at high
intensity exercise. In two uncontrolled studies, a reduction
of respiratory rate and an increase in IC was seen (Gigliotti
et al 2003; Porszasz et al 2005). In another controlled study,
the same effect was seen after 8 weeks of leg training on a
bike compared with no training in moderate to severe COPD
(Puente-Maestu et al 2006). In another study the opposite was
observed (Pellegrino 1999). However, this latter study included
eight quite unusual COPD subjects (ie, 38 [11] years, FEV1 3.5
(0.5) L and V O2 2.86 (0.6) L min-1) that can not be regarded
as a typical population of COPD patients. Arm training also
reduced DH during arm exercise in a small uncontrolled
study of COPD subjects (Gigliotti et al 2005).
Oxygen
Several observations in nonhypoxemic COPD patients demonstrate the favorable effect of oxygen supplementation during exercise in COPD patients without clinically significant
hypoxemia (Woodcock, Gross, Geddes, et al 1981; Dean et al
1992; O’Donnell, Bain, et al 1997). Endurance time increased
with supplemental oxygen at several different inhaled concentrations of oxygen both in a small group (10) of severe mildly
hypoxemic COPD patients and 7 healthy controls. In both
groups oxygen reduced fR, dyspnea, and increased VT, and
endurance time in a dose-dependent fashion, but the effects
were relatively larger in the COPD patients. In the healthy
subjects, differences were only appreciable with FIO2 > 0.5
or more. The improvement in endurance time was correlated
with a decrease in EELV (Somfay et al 2001). In a group of
18 severe COPD patients, oxygen reduced the degree of DH
during recovery from exercise but did not reduce breathlessness compared with air, which suggests that lung mechanics
International Journal of COPD 2006:1(4)
may play a different role in the genesis of dyspnea during
recovery from exercise (Stevenson et al 2004).
Opioids
Opioids have been show to decrease dyspnea during exercise
(Woodcock, Gross, Gellert, et al 1981; Light et al 1989), but
to our knowledge no study has addressed their effect on DH.
One study reported a decrease in fR for a given work-rate,
and increases in VT and ventilation were found (Light et al
1996). The reported side-effects of opioids and their tendency to lead to tolerance and addiction preclude their use
except in highly specific cases and end-of-life situations.
Benzodiazepines do not seem to improve exercise capacity
or dyspnea (Haas et al 1993) and have a deleterious effect
on inspiratory muscle function, reducing both VT and minute
ventilation (Jolly et al 1996).
Treatments that primarily reduce
flow limitation
One of the most exciting aspects of the renewed interest in DH is the realization that bronchodilator drugs may
significantly improve DH, and thus exercise tolerance (Belman
et al 1996; O’Donnell et al 1998), and that these changes
may not be detectable by isolated resting pulmonary function test (PFT) measurements like the FEV1 (Hadcroft and
Calverley 2001).
Bronchodilators
Several studies have addressed the effect of bronchodilators on
lung hyperinflation (Table 2). In 13 COPD patients randomly
assigned to receive either inhaled placebo or salbutamol, the
bronchodilator caused significant increase in both FEV1 and
forced vital capacity (FVC). There was also a significant
reduction in the peak exercise EELV/TLC and esophageal
inspiratory pressure/peak inspiratory esophageal pressure.
Moreover a significant reduction in breathlessness that correlated with changes in end-inspiratory lung volume/TLC
was also seen (Belman et al 1996). In a retrospective review
of 281 patients with TLC >133% predicted and 676 with TLC
between 115% to 133% predicted, 200µg of salbutamol produced a significant reduction of FRC, RV, and increased the
IC and FVC. The FEV1 improved in only a minority (around
30%). If lung volume measurements are also considered, the
overall bronchodilator response may improve up to 76% of
the severely hyperinflated group and up to 62% of the moderately hyperinflated ones. Changes in volumes correlated
poorly with changes in maximal airflows. Surprisingly TLC
was also slightly reduced (about 2.5%) by bronchodilators
389
�Ref
FEV1 (%)
“n”/design
Intervention
Duration Resting PFT
Resting
hyperinflation
13 cross-over
against placebo
281 TLC>133% and
676 TLC 113%–
133%) //
retrospective
200ìg of
salbutamol
200μg of
salbutamol
Improvement in
FEV1 and FVC
~30% improved
FEV1
16 with positive BD
test// cross-over
against placebo
20// 11 with FL
50μg of salmeterol
Improvement in
FEV1 and FVC
Reduced FRC
400μg of
salbutamol
No changes in
FEV1
Improvement in
IC only in FL
Improvement in
FEV1
Increased IC
Improvement in
FEV1, FVC, SVC,
Improvement
VC, but not FEV1,
Increased IC and
decreased FRC
Increased IC and
decreased FRC
Improvement VC,
but not FEV1,
Increased FEV1,
Improved
Increased IC and
decreased FRC
Increased IC
No effect on
FEV1, FVC, SVC,
Decreased
RV/TLC
Exercise
hyperinflation
Exercise
dyspnea
Improved
Improved
Endurance
time CLE
Comment
Single dose
(Belman et al
1996)
(Newton et al
2002)
40 (3)
52 (1)
//78(1)*
(RamirezVenegas
et al 1997)
(Boni et al
2002)
52 (13)
(Di Marco
et al 2993)
52 (3)*
20// cross-over
against placebo
200μg of
salbutamol// 12μg
of formoterol //
50μg of salmeterol
//200μg of oxytropium
43 (12)
40/41 // placebo
controlled
96/91 // placebo
controlled
Tiotropium 18μg/d
4 weeks
Tiotropium 18μg/d
6 weeks
Tiotropium 18μg/d
6 weeks
Salmeterol (50μg bid)
added to the
daily drug regimen.
Salmeterol (50μg
bid) added to the
daily drug regimen.
2 weeks
47 (18)
Reduced FRC
RV//
TLC was also reduced by
BD. overall sensitivity may
improve up to ~66% by
measuring changes in lung
volumes.
lower dyspnea during
resistive breathing
Improved
Changes in dyspnea
correlated with
improvements in resting IC
Fomoterol better than
salmeterol and than
oxytropium // Those with
decrease IC achieved a
larger effect
Long-term
(Celli et al
2003)
(O’Donnell
et al 2004a)
International Journal of COPD 2006:1(4)
(Maltais
et al 2005)
(O’Donnell
2004c)
(Man et al
2004)
44 (13)
43 (13)
42 (3)*
32 (4)
131/117 //placebo
controlled
23// cross-over
against placebo
16 “no reversible”//
cross-over against
placebo
2 weeks
Note: Values are men with standard deviation within parenthesis; except *SEM.
Improved
Improved
Improved
Improved
Improved
Improved
Improved
Improved
105 (40)s
(21%) >than
placebo
171 (58) s>
than placebo
No
improvement
Effects seen at 2.5h
still at 8h
Increased In peak oxygen
uptake and VT at 10w
incremental test.
Changes in dyspnea
correlated with
improvements DH and
esophageal pressure
Puente-Maestu and Stringer
390
Table 2 Summary of trials on BD measuring resting or dynamic hyperinflations an outcome
�Hyperinflation in COPD
suggesting that the changes in airways resistance or the
familiarity with the method may have affected the constant
volume plethysmographic technique used to measure volumes (Newton et al 2002). Unless salbutamol had produced
changes in the ability to generate force by the respiratory
muscles, or the elastic properties of the lung, both of which
it are unlikely. Ramirez-Venegas and colleagues (1997)
found that the use of salmeterol reduced not only dyspnea
but improved lung function in patients with COPD. Patients
showed an increase in FVC, a reduction in RV and FRC, and
no changes in TLC following inhalation of salmeterol. Boni
and colleagues (2002) studied 20 COPD, 11 with flow limitation using the negative expiratory pressure before and after
the inhalation of 400μg salbutamol. Following salbutamol,
IC did not change in non-flow limited patients but increased
significantly in the flow-limited ones. Dyspnea decreased
in relation to IC at rest even in the absence of a significant
improvement in FEV1. Di Marco and colleagues (1993) found
that in patients with decreased baseline inspiratory capacities; there was a much greater increase of IC after administration of bronchodilators such as salbutamol, formoterol,
salmeterol, and oxitropium. This increase correlated closely
with improvement in a sensation of dyspnea. Celli and colleagues (2003) evaluated the long-term effects (4 weeks) of
18µg/day of tiotropium. Significant similar improvements in
the area under the curve of FEV1 and IC and over the curve
in FRC were observed, reflecting sustained improvements in
hyperinflation. O’Donnell, Fluge, and colleagues (2004) and
Maltais and colleagues (2005) conducted a multicentric study
on the long-term effects (6 weeks) of 18µg/day of tiotropium.
Tiotropium reduced lung hyperinflation indices at rest and
during exercise, and improved exercise tolerance 8 h after
the inhalation of the drug. Finally O’Donnell, Voduc, and
colleagues (2004) studied the effects of 50µg of inhaled salmeterol. After salmeterol versus placebo at rest, IC increased
and FRC decreased at a standardized time during exercise.
In addition, IC and VT increased and dyspnea decreased.
Significant increments in peak ventilation, oxygen uptake,
and the duration of the incremental test were also seen. Man
and colleagues (2004) studied 16 patients with “irreversible”
severe COPD after two weeks of treatment with 50µg of
salmeterol twice a day. Salmeterol significantly reduced the
transdiaphragmatic pressure-time product, DH, and Borg
scores during endurance treadmill walk, however there was
no significant change in exercise endurance time.
In contrast with the results of Table 2, bronchodilators
have shown wide variations in regards to changes in exercise
International Journal of COPD 2006:1(4)
capacity (Liesker et al 2002). Earlier negative studies may have
included subjects whose exercise capacity was not ventilatorylimited. In fact, several studies in Table 2 demonstrate that the
effects of bronchodilators are larger in those with flow limitation than in those without flow limitation. Flow limitations are
a major determinant of exercise capacity (Diaz et al 2000).
Alternatively, they may have included a great proportion of
patients that were not responsive to bronchodilators (about
1/3 of COPD patients do not improve either FEV1 or IC with
bronchodilators) (Newton et al 2002). Third, some of those
studies may have used insufficient doses and only a few included long-acting bronchodilators, and in particular, none
included tiotropium (Liesker et al 2002). Fourth, most studies
included 6 minute walking tests to measure exercise capacity;
however, 6 minute walking distance is sensitive to a learning effect. Two training sessions are necessary to eliminate
a learning effect in walking tests (Kervio et al 2003; Knox
et al 1988). Constant work load tests appears to be more appropriate than other tests, as they allow for placebo-controlled
comparisons of symptoms and physiological parameters,
including exercise endurance time at a standardized work
rate or power output (O’Donnell, Fluge, et al 2004). Cycle
exercise endurance testing, combined with measurements of
exertional dyspnea, ventilation, and dynamic operating lung
volumes, has been shown to be reliable, reproducible, and
responsive to the intervention (Oga et al 2000; Puente-Maestu
et al 2003; O’Donnell, Fluge, et al 2004).
Heliox
Helium is gas that is less dense and more viscous than air. Its
lower density can decrease airway resistance in the absence
of any anatomical change. Therefore, the greatest theoretical
benefit of heliox would be achieved by decreasing turbulent
flow in large airways and at branch points in the tracheobronchial tree.
Heliox is unlikely to be of substantial benefit in adults
with asthma. A systematic analysis pooled results from seven
trials enrolling nearly 400 patients and found no significant
improvement in recovery of pulmonary function in patients
with acute asthma who were treated with heliox (Rodrigo
et al 2001, 2003). One study examined the effects of heliox
(80:20) on gas exchange, breathing pattern, respiratory mechanics, and gas distribution in patients with stable, but severe, COPD (Swidwa et al 1985). Heliox was not associated
with significant changes in minute ventilation or breathing
pattern, however a 15% reduction in FRC which increased
back to baseline after a return to air breathing was observed.
391
�Puente-Maestu and Stringer
On the other hand another small trial found no change in
DH among COPD patients (Pecchiari et al 2004). In addition, the high cost and limited availability of heliox make
its clinical use more difficult. In another study, researchers
used an esophageal balloon in recently extubated patients
without significant lung disease to quantify intrathoracic
pressure swings and estimate the work of breathing (Jaber
et al 2001). Fifteen of 18 patients exhibited a drop in their
work of breathing, although gas exchange parameters were
unchanged. The patients also reported decreased dyspnea
while breathing heliox.
The clinical effects of heliox in the absence of positive
pressure ventilation have not been well studied. Fifty normoxic COPD with an acute exacerbations were prospectively
randomized in the emergency room to receive either heliox
(70:30), or air as the driving gas for updraft nebulization of
a mixture of salbutamol and ipratropium bromide The baseline FEV1 was 44% There were no significant differences in
the change of FEV1 between the two groups by either the 1
h or 2 h time point. Lung volume measurements were not
made, but the improvement in forced expiratory flow over
the middle half of the FVC (FEF25%–75%) was significantly
greater in the heliox group, the authors considered that this
improvement had no clinical significance, but measures of
dyspnea or recovery were not provided (deBoisblanc et al
2000). A retrospective review of 81 patients presenting to the
emergency department with COPD and hypercarbic respiratory insufficiency found a significant reduction in the rates
of intubation (8% vs 50%) and in-hospital mortality (3% vs
24%) in the patients who received heliox as compared with
control patients (Gerbeaux et al 2001).
Several trials have compared noninvasive positive pressure ventilation (NPPV) combined with either air or heliox in
patients with exacerbations of COPD. In one well-designed
trial, patients with acute exacerbations of COPD were treated
with low or high pressure NPPV in combination with heliox
or oxygen-supplemented air (Jaber et al 2000). Differences in
breathing pattern, work of breathing, and gas exchange were
measured in nine patients using an esophageal balloon technique. Heliox was not associated with changes in breathing
pattern, whereas high pressure NPPV produced significant
increases in tidal volume and minute ventilation. Heliox was
associated with a reduction in PaCO2 and improvement in all
measured indices of respiratory effort and work. The beneficial effects on the measured variables were further increased
when high pressure NPPV was combined with heliox, compared with the low pressure/air group. The authors suggest
392
that the addition of heliox to NPPV may allow a larger
number of patients to benefit from NPPV. In addition, heliox
may allow the use of lower levels of pressure support, which
could reduce complications and patient discomfort resulting from high pressures and flow rates (Jaber et al 2000). A
crossover study monitored the effects of NPPV plus either
heliox (70:30) or oxygen (FiO2 0.30) on gas exchange and
dyspnea in 19 patients with severe COPD (Jolliet et al 1999).
The use of heliox decreased PaCO2, reduced dyspnea, and
favorably changed the breathing pattern of patients. Peak
inspiratory flow rates were higher, while inspiratory time
and the ratio of inspiratory time to respiratory cycle length
were both decreased. All of these findings suggest a reduced
work of breathing. A third series of 23 intubated patients with
COPD and respiratory failure found that the administration
of heliox significantly reduced intrinsic PEEP, trapped lung
volume, and peak and mean airway pressures (Tassaux et al
2000). Similar findings were noted in a second small study
of 12 patients recovering from acute exacerbations of COPD.
In this randomized prospective crossover trial, heliox decreased the resistive work of breathing and intrinsic positive
end-expiratory pressure (auto-PEEP) without changing the
breathing pattern (Diehl et al 2003).
One study examined the impact of heliox on pulmonary
function in ten aging runners with very mild COPD during
cardiopulmonary exercise testing. Heliox was associated
with an increase in minute ventilation, in the absence of any
change in the metabolic cost of breathing (Babb et al 2003).
Another work studied 12 patients with severe COPD (FEV1
38[10]% of predicted) comparing heliox (79:21) with air.
Exercise endurance increased significantly and peak ventilation time with heliox. This was associated with a significant
reduction in lung DH and dyspnea at isotime. The reduction
in dyspnea correlated significantly with the increase in IC
induced by heliox (Palange et al 2004).
Increasing elastic recoil
Although there are no currently available treatments to return
the lung to its normal structure once it has been damaged by
the inflammatory process (like COPD), this may indeed be
possible in the future using stem cells (Ortiz et al 2003; Suratt
et al 2003). Stem cells may indeed improve the compliance
characteristics of the lung. However, at this time lung volumereduction surgery (LVRS; a surgical or bronchoscopic procedure that involves resection or exclusion of the most severely
affected regions of diseased lung tissue) in patients with diffuse
emphysema, may improve lung function by increasing elastic
International Journal of COPD 2006:1(4)
�Hyperinflation in COPD
recoil of the lung, the effective pressure driving maximal
expiratory flow airway, and the conductance of the airways by
augmenting the radial traction of their alveolar attachments.
Hence it may improve flow proportionately at all areas of the
lung and secondarily reduce hyperinflation (Brantigan et al
1959; Rogers et al 1968; Fessler and Permutt 1998; Ingenito
et al 2001). This surgery was initially described in the late
1950s (Brantigan et al 1959). The persistent air leaks that
limited early success have been diminished considerably by
the recent surgical advances, which has increased interest in
this procedure and led to its greater availability (Wakabayashi
et al 1991; Cooper et al 1995; Keenan et al 1996; Hazelrigg
et al 1997; Brenner et al 2004).
Several randomized trials have compared LVRS with
optimal medical treatment (Geddes et al 2000; Fishman et al
2003; Miller, Berger, et al 2005) and by far the largest of
these was the National Emphysema Treatment Trial (NETT)
(Fishman et al 2003). NETT enrolled over 1200 patients
with severe emphysema who underwent baseline assessment followed by six months of mandatory pulmonary
rehabilitation. The patients were then randomly assigned
to surgical or continued medical therapy, with plans for
three-year follow-up. In this study high risk patients were
defined as having: FEV1 < 20% and either diffusing capacity
of the lung for carbon monoxide (DLCO) < 20% predicted
or homogeneous changes on chest computer tomography
(Table 3). The 30-day mortality was 16% in the surgical
group compared with no deaths in the medically managed
group (NETT 2001). In the remainder of the study, while
there was a significant improvement in exercise capacity
in the surgical group (the same has been found in another
study [Dolmage et al 2004]), there was no difference in the
total mortality rate at the end of follow-up with surgical or
medical therapy (9% vs 10% per year with medical therapy),
however, the 90-day mortality was significantly higher with
Table 3 Subjects likely to benefit for lung volume surgery
Marked disability after rehabilitation
(peak work rate <40% predicted)
Quit from smoking at least 6 month before
Understanding of risks and benefits
Heterogeneous enphysiema
Marked hyperinflation
DLCO <50% >20% as percent of predicted
FEV1 < 35% >20% as percent of predicted
Normal ejection fraction
Abbreviations: DLCO, diffusing capacity of the lung for carbon monoxide;
FEV, forced expiratory volume in one second
International Journal of COPD 2006:1(4)
surgery (5.2% vs 1.5%) (Fishman et al 2003). Only the subset
of patients with upper lobe predominant emphysema and low
exercise capacity (24%) had a significant reduction in total
mortality with surgery (7% vs 15% per year, risk ratio 0.47).
In this study, low exercise capacity was defined as less than
40% of the gender–specific predicted work rate (40 W in
men and 25 W in women) (Fishman et al 2003).
Recently LVRS has been attempted by bronchoscopically
placing one-way valves in airways associated with areas of
severe emphysema and hyperexpansion. These valves allow
air and secretions to move from alveoli to the central airways,
but prevent air from entering the distal airspaces. Over time,
this results in collapse of the affected regions. Experience in
humans is limited, but one series of 19 patients who underwent unilateral valve placement noted decreased air-trapping
and improvement in exercise tolerance one month after the
procedure (Hopkinson et al 2005).
LVRS produces less functional improvement than lung
transplant (Gaissert et al 1996), but since patients who undergo
LVRS are not automatically excluded from receiving a subsequent lung transplant both treatments might be sequentially
applied (Nathan et al 2004).
Large bullae which can potentially benefit from surgical
resection are uncommon clinically. An important challenge
for the clinician is to select the patient for bullectomy who
can have the greatest benefit with the lowest morbidity and
mortality. The most common indication for bullectomy is
severe dyspnea in the setting of a large bulla occupying at
least 30%–50% of the hemithorax. Another indication is
history of a pneumothorax. The physiologic outcome after
surgery is determined largely by the size of the bulla and
the severity of the underlying emphysema, and patients with
severe generalized emphysema tend to do poorly (Nickoladze
1992). The surgical risk is increased when the FEV1 is less
than 40% of predicted, and the presence of severe dyspnea,
a markedly reduced FEV1, hypercapnia, or cor pulmonale
makes the risk of surgery almost prohibitive (Gunstensen
and McCormack 1973).
Relieving the inspiratory threshold
load
Pursed-lip breathing
We have reviewed the effects of PLB above. In addition to
reducing respiratory rate, it likely reduces dynamic airways
compression by generating an extratoracic resistance and thus
creates PEEP.
393
�Puente-Maestu and Stringer
Positive end-expiratory pressure
Intrinsic PEEP is frequent in mechanically ventilated patients
with obstructive airways disease. Several studies indicate that
in patients with flow limitation by dynamic airway collapse, the
application of small amounts of external PEEP can be beneficial
since intrinsic PEEP can account for about one-third of the total
work of breathing (Coussa et al 1993). Hyperinflation may not
be affected when applied PEEP is below 85% of the measured
auto-PEEP (Ranieri et al 1993), however not all patients with
auto-PEEP and DH have expiratory flow limitation (Armaganidis et al 2000) and care has to be taken to reduce the impact
of a narrow diameter or kinked endotracheal tube, inspisated
secretions, exhalation/PEEP valves, and asynchrony due to pain
or agitation. The incidence of expiratory flow limitation has
been reported to be as high as 93% upon initiation of mechanical ventilation, but it is reduced by half over time with therapy
(Alvisi et al 2003). It seems to be more likely when patients are
supine instead of semirecumbent (Valta et al 1994).
A recent meta-analysis of 7 studies including a total of
65 patients with COPD shows a modest beneficial effect of
ventilatory support on exercise tolerance as well (van ‘t Hul
et al 2002), probably in part because continuous positive
airway pressure (CPAP) unloads inspiratory muscles from
the inspiratory threshold load imposed by intrinsic PEEP
(Pepe and Marini 1982; Haluszka et al 1990; Petrof et al
1990; Lougheed et al 1995). In severe COPD patients CPAP
of 0.5kPa resulted in a significant reduction in dyspnea and
an increase in exercise endurance time (O’Donnell, Sanii,
Giesbrecht, et al 1988; O’Donnell, Sanii, Younes, et al 1988),
however excessive CPAP increases the perception of breathing
effort (O’Donnell, Sanii, Giesbrecht, et al 1988) and hence it
should be titrated individually. Inspiratory pressure support
(IPS) a form of pressure-targeted mechanical ventilation which
each breath is patient triggered and supported has been shown
to improve exercise tolerance (Keilty et al 1994; Maltais et al
1995; Kyroussis et al 2000; Polkey et al 2000; van’t Hul et al
2004) and reduce lactate production (Polkey et al 2000).
Proportional assisted ventilation, a mode of partial ventilatory
assistance adapted to the intensity and timing of spontaneous
ventilatory pattern by providing inspiratory pressure in proportion to a patient’s spontaneous effort, has been shown also
to increase exercise tolerance (Dolmage and Goldstein 1997;
Bianchi et al 1998). The role of pressure support in severely
limited COPD patients is not yet clear. In a recent double-blind
controlled study of 29 patients with moderate-severe COPD
and ventilatory limitation during an incremental exercise test,
394
37 patients were exercised with either IPS 1kPa (19 subjects)
versus 0.5kPa (18 subjects) in the control group. Statistically
significant differences were found in favor of the IPS in shuttle
walking distance, cycle endurance, and reduction in minute
ventilation during exercise (van’t Hul et al 2004).
Measuring flow limitation and
dynamic hyperinflation
Spirometry
Spirometry is a central parameter in the diagnosis and staging
of COPD, yet it is poorly correlated with dyspnea and exercise
capacity (Hay et al 1992; Bauerle et al 1998) and has limited
individual value to predict the increase in exercise tolerance in
patients with severe COPD (Tobin et al 1984; O’Donnell et al
1998), however resting IC seems to be better index of exercise
capacity (Diaz et al 2000) and changes in IC are better indicator
of the reduction of dyspnea and exercise tolerance (RamirezVenegas et al 1997; Hadcroft and Calverley 2001; Boni et al
2002; Celli et al 2003; O’Donnell, Fluge, et al 2004; Stevenson
et al 2005), furthermore the use of IC as an adjunct criterion for
a bronchodilator test apparently increases the sensitivity to detect
functional changes clinically relevant (Newton et al 2002; Parker
et al 2005). Although there is no defined criterion to evaluate
changes in IC (Pellegrino et al 2005), changes after bronchodilators have been usually larger than 15% (Ramirez-Venegas et al
1997; Hadcroft and Calverley 2001; Boni et al 2002; Celli et al
2003; O’Donnell, Fluge, et al 2004). Other useful indexes of air
trapping are FRC, RV, and their relationship with TLC (Diez
Herranz 1995), although they are more complex to obtain and
not as widely available as spirometry.
Flow volume loops
The conventional method used to detect expiratory flow limitation using tidal breathing was one proposed by Hyatt and
Wilcox (1963). It consists of superimposing a flow–volume
loop of a tidal breath within a maximum flow–volume curve.
Expiratory flow limitation is not present when the patient
breathes below the maximal expiratory flow–volume curve
(Pride 1999). This method to detect expiratory flow limitation
has several methodological deficiencies such as intrathoracic
gas compression artefacts (which only can be detected with a
constant pressure body plethysmograph (Ingram and Schilder
1966), incorrect alignment of tidal with maximal expiratory
flow–volume curve considering the TLC as a fixed reference
point, which is not always valid (Younes and Kivinen 1984;
International Journal of COPD 2006:1(4)
�Hyperinflation in COPD
D’Angelo et al 1993). Respiratory mechanics and the intrathoracic pressure swinging are different during the tidal
and maximal expiratory efforts and exercise may result in
changes in airways tone (Beck et al 1994). Another important
limitation of the conventional method is that it requires patient
cooperation.
The negative expiratory
pressure technique
The negative expiratory pressure technique (NEP) method is
based on the principle that the increase in pressure caused by
NEP should result in increased expiratory flow. By contrast,
in flow-limited subjects, application of NEP should not change
the expiratory flow (Koulouris et al 1995). For technical details
we refer the reader elsewhere. This method does not require
FVC maneuvers, collaboration on the part of the patient, or
use of a body plethysmograph, and can be used during spontaneously breathing subjects during exercise (Calverley and
Koulouris 2005).
Measurement of dynamic hyperinflation
Since TLC remains essentially unaltered during exercise
(Stubbing et al 1980; Younes and Kivinen 1984) changes
in EELV during exercise can be reliably tracked by serial
IC measurements (Figure 5). Exercise IC measurements are
reproducible, provided care is taken with their measurement. In one study of 29 patients the variability coefficient
was 17% at rest and approximately 20% during exercise
with intra-class correlation coefficients of 0.77 and 0.73
respectively (O’Donnell et al 1998). In another study of 15
patient esophageal pressures were found reproducible during
IC maneuvers during exercise at different work-rates, the
reduction in IC during exercise correlates well with esophageal balloon-derived measurements of dynamic compliance
(O’Donnell, Chau, et al 1997). In another study, three methods
of measuring IC were tested in 10 severe COPD subjects. IC
calculated, after correction of the expiratory part of the signal,
as the difference between the mean EELV of the six breaths
that preceded the IC prompt and the peak inspiratory volume
was found to be the most reproducible method (Dolmage and
Goldstein 2002). In an unpublished multicentric study of 463
patients with moderate to severe COPD, the intra-class correlation of exercise IC measurements during serial exercise
tests exceeded 0.85 (O’Donnell, He, et al 2004). The extent
of the reduction in IC with exercise in COPD is variable. In
a population of 105 patients with moderate to severe COPD,
International Journal of COPD 2006:1(4)
IC at end-exercise was reduced by 20% of its already-reduced
resting value (O’Donell et al 2001). In another smaller group
of 27 severe COPD patients a similar reduction was found
at maximum ventilation at the end of high intensity exercise
(Puente-Maestu et al 2005). Similar changes were found in
severe COPD in 15 severe COPD (Yan et al 1997). However,
guidelines for standardization of IC measurement have not
yet been issued. Recently a new complex method called optoelectronic plethysmography has been developed for research
purposes (Aliverti et al 2004)
Conclusion
Flow limitation and DH are crucial pathophysiological
mechanisms in the development of exercise intolerance,
dyspnea, and respiratory failure in COPD patients. As the
disease advances with progression of symptoms and impairment, the flow limitation and DH proportionally worsens.
Several methods of treatment may palliate its impact of
flow limitation and DH on the patient, including physical
therapy, bronchodilators, ventilatory support, oxygen, heliox,
or surgery. Measurement of DH may be done indirectly by
spirometry or by more direct approaches that have known
limitations or are not widely available. Clinical use is limited by the lack of a standard method to measure DH or flow
limitation during exercise.
References
[ACCP/AACVPR] Pulmonary Rehabilitation Guidelines Panel,
American College of Chest Physicians, American Association of
Cardiovascular and Pulmonary Rehabilitation. 1997. Pulmonary
rehabilitation: joint ACCP/AACVRR evidence based guidelines.
Chest, 112:1363–96.
Agostoni E, Hyatt RE. 1986. Static behaviour of the respiratory system.
In: Handbook of physiology. The respiratory system, sect. 3,
vol. III, part 1. Bethesda, MD: American Physiological Society,
pp 113–130.
Aldrich TK, Shapiro SM, Sherman MS, et al. 1989. Alveolar pressure and
airway resistance during maximal and submaximal respiratory efforts.
Am Rev Respir Dis, 140:899–906.
Aliverti A, Stevenson N, Dellaca RL. et al. 2004. Regional chest wall
volumes during exercise in chronic obstructive pulmonary disease.
Thorax, 59:210–16.
Alvisi V, Romanello A, Badet M, et al. 2003. Time course of expiratory flow
limitation in COPD patients during acute respiratory failure requiring
mechanical ventilation. Chest, 123:1625–32.
Armaganidis A, Stavrakaki-Kallergi K, Koutsoukou A, et al. 2000. Intrinsic
positive end-expiratory pressure in mechanically ventilated patients
with and without tidal expiratory flow limitation. Crit Care Med,
28:3837–42.
Babb TG, DeLorey DS, Wyrick BL. 2003. Ventilatory response to exercise
in aged runners breathing He-O2 or inspired CO2. J Appl Physiol,
94:685–93.
Babb TG, Viggiano R, Hurley B, et al. 1991. Effect of mild-to-moderate airflow
limitation on exercise capacity. J Appl Physiol, 70:223–30.
395
�Puente-Maestu and Stringer
Barach AL. 1955. Breathing exercises in pulmonary emphysema and alied
chronic respiratory disease. Arch Phys Med Reahab, 36:379–90.
Bauerle O, Chrusch CA, Younes M. 1998. Mechanisms by which COPD
affects exercise tolerance. Am J Respir Crit Care Med, 157:57–68.
Beck KC, Offord KP, Scanlon PD. 1994. Bronchoconstriction occurring
during exercise in asthmatic patients. Am J Respir Crit Care Med,
149:352–7.
Beeh KM, Beier J, Kornmann O, et al. 2003. Long-term repeatability of
induced sputum cells and inflammatory kers in stable, moderately severe
COPD. Chest, 123:778–83.
Bellee F, Grassino A. 1982. Effect of pressure and timing of contraction on
human diaphragm fatigue J Appl Physiol, 53:1190–5.
Bellee F, Grassino. 1983. A Force reserve of the diaphragm in patients
with chronic obstructive pulmonary disease. J Appl Physiol,
55:8–15.
Belman MJ, Botnick WC, Shin JW. 1996. Inhaled bronchodilators
reduce dynamic hyperinflation during exercise in patients with
chronic obstructive pulmonary disease. Am J Respir Crit Care Med,
153:967–75.
Bianchi L, Foglio K, Pagani M, et al. 1998. Effects of proportional assist
ventilation on exercise tolerance in COPD patients with chronic
hypercapnia. Eur Resp J, 11:422–7.
Bianchi R, Gigliotti F, Romagnoli I, et al. 2004. Chest wall kinematics and
breathlessness during pursed-lip breathing in patients with COPD.
Chest, 125:459–65.
Black LF, Hyatt RE. 1969. Maximal respiratory pressures: normal values and
relationship to age and sex. Am Rev Respir Dis, 99:696–702.
Boni E, Corda L, Franchini D, et al. 2002. Volume effect and exertional
dyspnoea after bronchodilator in patients with COPD with and without
expiratory flow limitation at rest. Thorax, 57:528–32.
Bowen JB, Votto JJ, Thrall RS, et al. 2000. Functional Status and Survival
Following Pulmonary Rehabilitation. Chest, 118:697–703.
Brantigan OC, Mueller E, Kress MB. 1959. A surgical approach to pulmonary
emphysema. Am Rev Respir Dis, 80:194–202.
Brenner M, Hanna NM, Mina-Araghi R, et al. 2004. Innovative approaches
to lung volume reduction for emphysema. Chest, 126:238–48.
Calverley PMA and Koulouris NG. 2005. Flow limitation and dynamic
hyperinflation: key concepts in modern respiratory physiology. Eur
Respir J, 25:186–99
Casaburi R, Gosselink R, Ramer M, et al. 1999. American Thoracic
Society/European Respiratory Society skeletal muscle dysfunction in
chronic obstructive pulmonary disease. Am J Respir Crit Care Med,
159:S1–S40.
Casaburi R, Porszasz J, Burns MR, et al. 1997. Am J Respir Crit Care
Med, 155:1541–51.
Casaburi R. 2001. Special considerations for exercise training. In: ACSM
resource manual for guidelines for exercise testing and prescription.
4th ed. ACSM, pp 346–52.
Casanova C, Cote C, de Torres JP, et al. 2005. Inspiratory-to-total lung
capacity ratio predicts mortality in patients with chronic obstructive
pulmonary disease. Am J Respir Crit Care Med, 171:591–7.
Celli B, ZuWallack R, Wang S, et al. 2003. Improvement in resting inspiratory capacity and hyperinflation with tiotropium in COPD patients with
increased static lung volumes. Chest, 124:1743–8.
Celli BR, Cote CG, Marin JM, et al. 2004. The body mass index, airflow
obstruction, dyspnoea, and exercise capacity index in chronic obstructive pulmonary disease. N Engl J Med, 350:1005–12.
Cherniack RM, Hodson A. 1963. Compliance of the Chest wall in chronic
bronchitis and emphysema. J Appl Physiol, 18:707–11.
Citterio G, Agostoni E, Del Santo A, et al. 1981. Decay of inspiratory muscle
activity in chronic airway obstruction. J Appl Physiol, 51:1388–97.
Cooper JD, Trulock EP, Triantafillou AN, et al. 1995. Bilateral pneumectomy (volume reduction) for chronic obstructive pulmonary disease.
J Thorac Cardiovasc Surg, 109:106–16.
Cosio MG, Hale KA, Niewoehner DE. 1980. Morphologic and morphometric effects of prolonged cigarette smoking on the small airways. Am
Rev Respir Dis, 122:265–21.
396
Coussa ML, Guerin C, Eissa NT, et al. 1993. Partitioning of work of
breathing in mechanically ventilated COPD patients. J Appl Physiol,
75:1711–19.
D’Angelo E, Prandi E, Milic-Emili J. 1993. Dependence of maximal
flow-volume curves on time-course of preceding inspiration. J Appl
Physiol, 75:1155–9.
Dean NC, Brown JK, Himelman RB, et al. 1992. Oxygen may improve dyspnoea and endurance in patients with chronic obstructive pulmonary
disease and only mild hypoxemia. Am Rev Respir Dis, 146:941–5.
deBoisblanc BP, DeBleiux P, Resweber S, et al. 2000. Randomized trial
of the use of heliox as a driving gas for updraft nebulization of bronchodilators in the emergent treatment of acute exacerbations of chronic
obstructive pulmonary disease. Crit Care Med, 28:3177–80.
Di Marco J, Milic-Emili J, Boveri P, et al. 2003. Effect of inhaled bronchodilators on inspiratory capacity and dyspnoea at rest in COPD. Eur
Respir J, 21:86–94.
Diaz O, Villafranca C, Ghezzo H, et al. 2000. Exercise tolerance in COPD
patients with and without tidal expiratory flow limitation at rest. Eur
Respir J, 16:269–75.
Diehl JL, Mercat A, Guerot E, et al. 2003. Helium/oxygen mixture reduces
the work of breathing at the end of the weaning process in patients
with severe chronic obstructive pulmonary disease. Crit Care Med,
31:1415–20.
Diez Herranz A. 1995. RV/TLC% ratio: alternative criteria of normality.
Eur Respir J, 8:1812–13.
Dodd DS, Brancatisano T, Engel LA. 1984. Chest wall mechanics during
exercise in patients with severe chronic air-flow obstruction. Am Rev
Respir Dis, 129:33–8.
Dolmage TE, Goldstein RS. 1997. Proportional assist ventilation and exercise tolerance in subjects with COPD. Chest, 111:948–54.
Dolmage TE, Goldstein RS. 2002. Repeatability of inspiratory capacity
during incremental exercise in patients with severe COPD. Chest,
121:708–14.
Dolmage TE, Waddell TK, Maltais F, et al. 2004. The influence of lung
volume reduction surgery on exercise in patients with COPD. Eur
Respir J, 23:269–74.
Donahoe M, Rogers RM, Wilson DO, et al. 1989. Oxygen consumption of the
respiratory muscles in normal and in malnourished patients with chronic
obstructive pulmonary disease. Am Rev Respir Dis, 140:385–91.
Eltayara L, Becklake MR, Volta CA, et al. 1996. Relationship between
chronic dyspnoea and expiratory flow limitation in patients with
chronic obstructive pulmonary disease. Am J Respir Crit Care Med,
154:1726–34.
Fessler HE, Permutt S. 1998. Lung volume reduction surgery and airflow
limitation. Am J Respir Crit Care Med, 157:715–22.
Fishman A, Martinez F, Naunheim K, et al; National Emphysema Treatment
Trial Research Group. 2003. A randomized trial comparing lungvolume-reduction surgery with medical therapy for severe emphysema.
N Engl J Med, 348:2059–73.
Gaissert HA, Trulock EP, Cooper JD, et al. 1996. Comparison of early functional
results after volume reduction or lung transplantation for chronic obstructive
pulmonary disease. J Thorac Cardiovasc Surg, 111:296–306.
Gallagher CG. 1994. Exercise limitation and clinical exercise testing in chronic
obstructive pulmonary disease. Clin Chest Med, 15:305–26.
Garrod R, Dallimore K, Cook J, et al. 2005. An evaluation of the acute
impact of pursed lips breathing on walking distance in nonspontaneous
pursed lips breathing chronic obstructive pulmonary disease patients.
Chron Respir Dis, 2:67–72.
Geddes D, Davies M, Koyama H, et al. 2000. Effect of lung-volumereduction surgery in patients with severe emphysema. N Engl J Med,
343:239–45.
Gerardi DA, Lovett L, Benoit-Connors ML, et al. 1996. Variables related
to increased mortality following out-patient pulmonary rehabilitation.
Eur Respir J, 9:431–5.
Gerbeaux P, Gainnier M, Boussuges A, et al. 2001. Use of heliox in patients
with severe exacerbation of chronic obstructive pulmonary disease. Crit
Care Med, 29:2322–4.
International Journal of COPD 2006:1(4)
�Hyperinflation in COPD
Gigliotti F, Coli C, Bianchi R, et al. 2003. Exercise training improves
exertional dyspnoea in patients with COPD: evidence of the role of
mechanical factors. Chest, 123:1794–802.
Gigliotti F, Coli C, Bianchi R, et al. 2005. Arm exercise and hyperinflation
in patients with COPD: effect of arm training. Chest, 128:1225–32.
Gottlieb DJ, Stone PJ, Sparrow D, et al. 1996. Urinary desmosine excretion in
smokers with and without rapid line of lung function: the Normative Aging
Study. Am J Respir Crit Care Med, 154:1290–5.
Green M, Pride MB. 1997. Normal respiratory mechanics. In:
Scadding JG, Cumming G, Thrubeck WM (eds). Scientific foundations of respiratory medicine. London: William Heinemann Medical
books, pp 113–29.
Grimby G, Bunn J, Mead J. 1968. Relative contribution of rib cage and abdomen to ventilation during exercise. J Appl Physiol, 24:159–66.
Gross D, Ladd HW, Riley EJ, et al. 1980. The effect of training on strength and
endurance of the diaphragm in quadriplegia. Am J Med, 68:27–35.
Gunstensen J, McCormack RJ. 1973. The surgical management of bullous
emphysema. J Thorac Cardiovasc Surg, 65:920–5.
Haas F, Salazar-Schichi J, Axen K. 1993. Desensitization to dyspnoea in
chronc obstructive pulmonary disease. In: Casaburi R, Petty TL (eds).
Principles and practice of pulmonary rehabilitation. Philadelphia: WB
Saunders Company, pp 241–51.
Hadcroft J, Calverley PM. 2001. Alternative methods for assessing bronchodilator reversibility in chronic obstructive pulmonary disease.
Thorax, 56:713–20.
Haluszka J, Chartrand DA, Grassino AE, et al. 1990. Intrinsic PEEP and
arterial PCO2 in stable patients with chronic obstructive pulmonary
disease. Am Rev Respir Dis, 141:1194–7.
Hamilton AL, Killian KJ, Summers E, et al. 1996. Symptom intensity and
subjective limitation to exercise in patients with cardiorespiratory
disorders. Chest, 110:1255–63.
Hay JG, Stone P, Carter J, et al. 1992. Bronchodilator reversibility, exercise
performance and breathlessness in stable chronic obstructive pulmonary
disease. Eur Respir J, 5:659–64.
Hazelrigg SR, Boley TM, Naunheim KS, et al. 1997. Effect of bovine
pericardial strips on air leak after stapled pulmonary resection. Ann
Thorac Surg, 63:1573–5.
Henke KG, Sharratt M, Pegelow D, et al. 1988. Regulation of end-expiratory lung
volume during exercise. J Appl Physiol, 64:135–46.
Hiraga T, Maekura R, Okuda Y, et al. 2003. Prognostic predictors for survival
in patients with COPD using cardiopulmonary exercise testing. Clin
Physiol Funct Imaging, 23:324–9.
Hopkinson NS, Toma TP, Hansell DM, et al. 2005. Effect of bronchoscopic lung
volume reduction on dynamic hyperinflation and exercise in emphysema.
Am J Respir Crit Care Med, 171:453–60.
Hyatt RE, Wilcox RE. 1963. The pressure-flow relationships of the intrathoracic airway in man. J Clin Invest, 42:29–39.
Hyatt RE. 1961. The interrelationships of pressure, flow, and volume during
various respiratory maneuvers in normal and emphysematous subjects.
Am Rev Respir Dis, 83:676–83.
Hyatt RE. 1983. Expiratory flow limitation. J Appl Physiol, 55:1–8.
Im Hof V, West P, Younes M. 1986. Steady-state response of normal subjects
to inspiratory resistive load. J Appl Physiol, 60:1471–81.
Ingenito EP, Loring SH, Moy ML, et al. 2001. Interpreting improvement in
expiratory flows after lung volume reduction surgery in terms of flow
limitation theory. Am J Respir Crit Care Med, 163:1074–80.
Ingram RH Jr, Schilder DP. 1966. Effect of gas compression on pulmonary
pressure, flow, and volume relationship. J Appl Physiol, 21:1821–6.
Ingram RH Jr, Schilder DP. 1967. Effect of pursed lips expiration on the
pulmonary pressure-flow relationship in obstructive lung disease. Am
Rev Respir Dis, 96:381–8.
Jaber S, Carlucci A, Boussarsar M, et al. 2001. Helium-oxygen in the
postextubation period decreases inspiratory effort. Am J Respir Crit
Care Med, 164:633–7.
Jaber S, Fodil R, Carlucci A, et al. 2000. Noninvasive ventilation with
helium-oxygen in acute exacerbations of chronic obstructive pulmonary
disease. Am J Respir Crit Care Med, 161:1191–200.
International Journal of COPD 2006:1(4)
Johnson BD, Reddan WG, Seow KC, et al. 1991. Mechanical constraints
on exercise hyperpnea in a fit aging population. Am Rev Respir Dis,
143:968–77.
Jolliet P, Tassaux D, Thouret JM, et al.1999. Beneficial effects of helium:
oxygen versus air: oxygen noninvasive pressure support in patients
with descompensated chronic obstructive pulmonary disease. Crit
Care Med, 27:2422–9
Jolly E, Aguirre L, Jorge E, et al. 1996. Acute effect of lorazepam on respiratory muscles in stable patients with chronic obstructive pulmonary
disease. Medicina (B Aires), 56:472–8.
Keatings VM, Collins PD, Scott DM, et al.1996. Differences in interleukin-8
and tumor necrosis factor-alpha in induced sputum from patients with
chronic obstructive pulmonary disease or asthma. Am J Respir Crit
Care Med, 153:530–4.
Keenan RJ, Landreneau RJ, Sciurba FC, et al. 1996. Unilateral thoracoscopic
surgical approach for diffuse emphysema. J Thorac Cardiovasc Surg,
111:308–15.
Keilty SE, Ponte J, Fleming TA, et al. 1994. Effect of inspiratory pressure
support on exercise tolerance and breathlessness in patients with severe
stable chronic obstructive pulmonary disease. Thorax, 49:990–6.
Kervio G, Carre F, Ville NS. 2003. Reliability and intensity of the sixminute walk test in healthy elderly subjects. Med Sci Sports Exerc,
35:169–74.
Killian KJ, Jones NL. 1994. Mechanisms of exertional dyspnoea. Clin
Chest Med, 15:247–57.
Killian KJ, Leblanc P, Tin DH, et al.1992. Exercise capacity and ventilatory,
circulatory, and symptom limitation in patients with chronic airflow
limitation. Am Rev Respir Dis, 146:935–40.
Kim MJ, Druz WS, Danon J, et al. 1976. Mechanics of the canine diaphragm.
J Appl Physiol, 41:369–82.
Knox AJ, Morrison JF, Muers MF. 1998. Reproducibility of walking test results
in chronic obstructive airways disease. Thorax, 43:388–92.
Koulouris NG, Valta P, Lavoie A, et al. 1995. A simple method to detect
expiratory flow limitation during spontaneous breathing. Eur Respir
J, 8:306–13.
Kyroussis D, Polkey MI, Hamnegard CH, et al. 2000. Respiratory muscle
activity in patients with COPD walking to exhaustion with and without
pressure support. Eur Respir J, 15:649–55.
Leith DE, Bradley M. 1976. Ventilatory muscle strength and endurance
training. J Appl Physiol, 41:508–16.
Levison H, Cherniack RM. 1968. Ventilatory cost of exercise in chronic
obstructive pulmonary disease. J Appl Physiol, 25:21–7.
Liesker JJ, Wijkstra PJ, Ten Hacken NH. 2002. A systematic review of the
effects of bronchodilators on exercise capacity in patients with COPD.
Chest, 121:597–608.
Light RW, Muro JR, Sato RI, et al. 1989. Effects of oral morphine on
breathlessness and exercise tolerance in patients with chronic obstructive pulmonary disease. Am Rev Respir Dis, 139:126–33.
Light RW, Stansbury DW, Webster JS. 1996. Effect of 30 mg of morphine
alone or with promethazine or prochlorperazine on the exercise capacity
of patients with COPD. Chest, 109:975–81.
Liu AN, Mohammed AZ, Rice WR, et al. 1999. Perforin-independent
CD8(+) T-cell-mediated cytotoxicity of alveolar epithelial cells is
preferentially mediated by tumor necrosis factor-alpha: relative insensitivity to Fas ligand. Am J Respir Cell Mol Biol, 20:849–58.
Lougheed MD, Webb KA, O’Donnell DE. 1995. Breathlessness during
induced hyperinflation in asthma: role of the inspiratory threshold load.
Am J Respir Crit Care Med, 152:911–20.
Mahler DA, Brent BN, Loke J, et al. 1984. Right ventricular performance and
central circulatory hemodynamics during upright exercise in patients with
chronic obstructive pulmonary disease. Am Rev Respir Dis, 130:722–9.
Maltais F, Hamilton A, Marciniuk D, et al. 2005. Improvements in symptomlimited exercise performance over 8 h with once-daily tiotropium in
patients with COPD. Chest, 128:1168–78.
Maltais F, LeBlanc P, Jobin J, et al. 1997. Intensity of training and physiologic adaptation in patients with chronic obstructive pulmonary disease.
Am J Respir Crit Care Med, 155:555–61.
397
�Puente-Maestu and Stringer
Maltais F, Reissmann H, Gottfried SB. 1995. Pressure support reduces
inspiratory effort and dyspnoea during exercise in chronic airflow
obstruction. Am J Respir Crit Care Med, 151:1027–33.
Man WD, Mustfa N, Nikoletou D, et al. 2005. Effect of salmeterol on
respiratory muscle activity during exercise in poorly reversible COPD.
Thorax, 59:471–6.
Mannix ET, Manfredi F, Farber MO. 1999. Elevated O2 cost of ventilation
contributes to tissue wasting in COPD. Chest, 115:708–13.
Marhsall R. 1962. Relationships between stimulus and work of breathing at
different lung volumes J Appl Physiol, 17:917–21.
Marin JM, Carrizo SJ, Gascon M, et al. 2001. Inspiratory capacity, dynamic
hyperinflation, breathlessness, and exercise performance during the
6-minute-walk test in chronic obstructive pulmonary disease. Am J
Respir Crit Care Med, 163:1395–9.
McGregor M, Becklake MR. 1961. The relationship of oxygen cost of
breathing to respiratory mechanical work and respiratory force. J Clin
Invest, 40:971–80.
Mead J, Turner JM, Macklem PT, et al. 1967. Significance of the relationship between lung recoil and maximum expiratory flow. J Appl
Physiol, 22:95–108.
Milic-Emili J. 2004. Provocative hypothesis: does mechanical injury the
peripheral airways play a role in the genesis of COPD in smokers?
J Chron Obstruc Pulm Dis, 1:1–8.
Miller JD, Berger RL, Malthaner RA, et al. 2005. Lung volume reduction
surgery vs medical treatment: for patients with advanced emphysema.
Chest, 127:1166–77.
Miller JD, Pegelow DF, Jacques AJ, et al. 2005. Effects of augmented respiratory
muscle pressure production on locomotor limb venous return during calf
contraction exercise. J Appl Physiol, 99:1802–15.
Montes de Oca M, Rassulo J, Celli BR. 1996. Respiratory muscle and cardiopulmonary function during exercise in very severe COPD. Am J Respir
Crit Care Med, 154:1284–9.
Mueller R, Chanez P, Campbell AM, et al. 1996. Different cytokine patterns in bronchial biopsies in asthma and chronic bronchitis. Respir
Med, 90:79–85.
Mueller RE, Petty TL, Filley GF. 1970. Ventilation and arterial blood gas
changes induced by pursed lips breathing. J Appl Physiol, 28:784–9.
Myers J, Prakash M, Froelicher V, et al. 2002. Exercise capacity and mortality
among men referred for exercise testing. N Engl J Med, 346:793–801.
Nathan SD, Edwards LB, Barnett SD, et al. 2004. Outcomes of COPD
lung transplant recipients after lung volume reduction surgery. Chest,
126:1569–74.
Neder A, Jones PW, Nery LE, et al. 2000. Determinants of the exercise
endurance capacity in patients with chronic obstructive pulmonary
disease. Am J Respir Crit Care Med, 162:497–504.
[NETT] National Emphysema Treatment Trial Research Group. 2001.
Patients at high risk of death after lung-volume-reduction surgery.
N Engl J Med, 345:1075–83.
Newton MF, O’Donnell DE, Forkert L. 2002. Response of lung volumes
to inhaled salbutamol in a large population of patients with severe
hyperinflation. Chest, 121:1042–50.
Nickoladze GD. 1992. Functional results of surgery for bullous emphysema.
Chest, 101:119–22.
Nield M, Arora A, Dracup K et al. 2003. Comparison of breathing patterns
during exercise in patients with obstructive and restrictive ventilatory
abnormalities. J Rehabil Res Dev, 40:407–14.
Niewoehner DE, Kleinerman J, Rice DB. 1974. Pathologic changes in
the peripheral airways of young cigarette smokers. N Engl J Med,
291:755–8.
Nishimura K, Izumi T, Tsukino M, et al. 2002. Dyspnoea is a better predictor of 5-year survival than airway obstruction in patients with COPD.
Chest, 121:1434–40.
Nishiyama O, Taniguchi H, Kondoh Y, et al. 2005. Factors in maintaining
long-term improvements in health-related quality of life after pulmonary
rehabilitation for COPD. Qual Life Res, 14:2315–21.
398
O’Donnell DE, Chau LKL, Bertley JC, et al. 1997. Qualitative aspects of
exertional breathlessness in chronic airflow limitation: pathophysiologic
mechanisms. Am J Respir Crit Care Med, 155:109–15.
O’Donnell DE, He Z, Lam M, et al. 2004. Reproducibility of measurements
of inspiratory capacity, dyspnoea intensity and exercise endurance in
multicentre trials in COPD. Eur Respir J, 24:323s
O’Donnell DE, Revill S, Webb KA. 2001. Dynamic hyperinflation and
exercise intolerance in COPD. Am J Respir Crit Care Med, 164:770–7.
O’Donnell DE, Webb KA. 2003. Chapter 18: Exercise. In: Calverley P,
MacNee W, Rennard S, et al. (eds). Chronic obstructive lung disease,
2nd ed. London: Edward Arnold Ltd, pp 243–65.
O’Donnell CE, Fluge T, Gerken F, et al. 2004. Effects of tiotropium on
lung hyperinflation, dyspnoea and exercise tolerance in COPD. Eur
Respir J, 23:832–40.
O’Donnell DE, Bain DJ, Webb KA. 1997. Factors contributing to relief of
exertional breathlessness during hyperoxia in chronic airflow limitation.
Am J Respir Crit Care Med, 155:530–5.
O’Donnell DE, D’Arsigny C, Fitzpatrick M, et al. 2002. Exercise hypercapnia in advanced chronic obstructive pulmonary disease. The role of
lung hyperinflation. Am J Respir Crit Care Med, 166:663–8.
O’Donnell DE, Lam M, Webb KA. 1998. Measurement of symptoms, lung
hyperinflation, and endurance during exercise in chronic obstructive
pulmonary disease. Am J Respir Crit Care Med, 158:1557–65.
O’Donnell DE, Sanii R, Giesbrecht G, et al. 1988. Effect of continuous positive airway pressure on respiratory sensation in patients with chronic
obstructive pulmonary disease during submaximal exercise. Am Rev
Respir Dis, 138:1185–91.
O’Donnell DE, Sanii R, Younes M. 1988. Improvement in exercise endurance in patients with chronic airflow. Limitation using continuous
positive airway pressure. Am Rev Respir Dis, 138:1510–14.
O’Donnell DE, Voduc N, Fitzpatrick M, et al. 2004. Effect of salmeterol on
the ventilatory response to exercise in chronic obstructive pulmonary
disease. Eur Respir J, 24:86–94.
O’Donnell DE, Webb KA. 1993. Exertional breathlessness in patients with
chronic airflow limitation. The role of lung hyperinflation. Am Rev
Respir Dis, 148:1351–7.
Oga K, Nishimura K, Tsukino M, et al. 2000. The effects of oxitropium bromide on exercise performance in patients with stable chronic obstructive
pulmonary disease. a comparison of three different exercise tests. Am
J Respir Crit Care Med, 161:1897–901.
Oga T, Nishimura K, Tsukino M, et al. 2002. Relationship between different indices of exercise capacity and clinical measures in patients with
chronic obstructive pulmonary disease. Heart Lung, 31:374–81.
Oga T, Nishimura K, Tsukino M, et al. 2003. Analysis of factors related to mortality in chronic obstructive pulmonary disease: role
of exercise capacity and health status. Am J Respir Crit Care Med,
167:544–49.
Ortiz LA, Gambelli F, McBride C, et al. 2003. Mesenchymal stem cell
engraftment in lung is enhanced in response to bleomycin exposure and ameliorates its fibrotic effects. Proc Natl Acad Sci U S A,
100:8407–11.
Oswald-Mammosser M, Apprill M, Bachez P, et al. 1991. Pulmonary
hemodynamics in chronic obstructive pulmonary disease of the
emphysematous type. Respiration, 58:304–10.
Oswald-Mammosser M, Kessler R, Massard G, et al. 1998. Effect of lung
volume reduction surgery on gas exchange and pulmonary hemodynamics at rest and during exercise. Am J Respir Crit Care Med,
158:1020–5.
Palange P, Valli G, Onorati P, et al. 2004. Effect of heliox on lung dynamic
hyperinflation, dyspnea, and exercise endurance capacity in COPD
patients. J Appl Physiol, 97:1637.
Parker M, Voduc N, Aaron SD, et al. 2005. Physiological changes during
symptom recovery from moderate exacerbations of COPD. Eur Respir
J, 26:420–8.
Pauwels RA, Buist AS, Calverley PMA, et al. 2001. Am J Respir Crit Care
Med, 163:1256–76.
International Journal of COPD 2006:1(4)
�Hyperinflation in COPD
Pecchiari M, Pelucchi A, D’Angelo E, et al. 2004. Effect of heliox breathing
on dynamic hyperinflation in COPD patients. Chest, 125:2075–82.
Peinado VI, Barbera JA, Abate P, et al. 1999. Inflammatory reaction in pulmonary muscular arteries of patients with mild chronic obstructive pulmonary
disease. Am J Respir Crit Care Med, 159:1605–11.
Pellegrino R, Viegi G, Brusasco V, et al. 2005. Interpretative strategies for
lung function tests. Eur Respir J, 26:948–68.
Pellegrino R, Villosio C, Milanese U, et al. 1999. Breathing during exercise
in subjects mild-to-moderate airflow obstruction: effects of physical
training. J Appl Physiol, 1697–704.
Pepe PE, Marini JJ. 1982. Occult positive end-expiratory pressure in mechanically ventilated patients with airflow obstruction: the auto-PEEP
effect. Am Rev Respir Dis, 126:166–70.
Pesci A, Balbi B, Majori M, et al. 1998. Inflammatory cells and mediators
in bronchial lavage of patients with chronic obstructive pulmonary
disease. Eur Respir J, 12:380–6.
Peto R, Speizer FE, Cochrane AL, et al. 1983. The relevance in adults of airflow
obstruction, but not of mucous hypersecretion, to mortality from chronic
lung disease. Am Rev Respir Dis, 128:491–500.
Petrof BJ, Calderini E, Gottfried SB. 1990. Effect of CPAP on respiratory
effort and dyspnoea during exercise in severe COPD. J Appl Physiol,
69:179–88.
Pinto-Plata VM, Cote C, Cabral H, et al. 2004. The 6-min walk distance:
change over time and value as a predictor of survival in severe COPD.
Eur Respir J, 23:28–33.
Polkey MI, Hamnegard CH, Hughes PD. 1998. Influence of acute lung
volume change on contractile properties of human diaphragm. J Appl
Physiol, 85:1322–8.
Polkey MI, Hawkins P, Kyroussis D, et al. 2000. Inspiratory pressure support prolongs exercise induced lactataemia in severe COPD. Thorax,
55:547–9.
Poon CS, Younes M, Gallagher CG. 1987. Effects of expiratory resistive
load on respiratory motor output in conscious humans. J Appl Physiol,
63:1837–45.
Porszasz J, Emtner M, Goto S, et al. 2005. Exercise training decreases
ventilatory requirements and exercise-induced hyperinflation at submaximal intensities in patients with COPD. Chest, 128:2025–34.
Potter WA, Olafsson S, Hyatt RE. 1971. Ventilatory mechanics and expiratory
flow limitation during exercise in patients with obstructive lung disease.
J Clin Invest, 50:910–19.
Pride NB, Green M. 1997. Abnormalities of respiratory mechanics. In:
Scadding JG, Cumming G, Thrubeck WM (eds). Scientific foundations of respiratory medicine. London: William Heinemann Medical
Bks, pp 669–88.
Pride NB, Macklem PT. 1986. Lung mechanics in disease. In: Fishman
AP (ed). Handbook of physiology, Section 3, Volume III, Part 2: The
respiratory system. Bethesda MD: American Physiological Society,
pp 659–92.
Pride NB. 1999. Tests of forced expiration and inspiration. In: Hughes
JMB, Pride NB (eds). Lung function tests: physiological principles and
clinical applications. London, WB Saunders, pp 3–25.
Puente-Maestu L, García J, Martínez-Abad Y, et al. 2005. Dyspnoea, ventilatory pattern, and changes in dynamic hyperinflation related to the
intensity of constant work rate exercise in COPD. Chest, 128:651–56.
Puente-Maestu L, Martínez Y, Pedraza F, et al. 2006. A controlled trial of
the effects of leg training on breathing pattern and dynamic hyperinflation in severe COPD. Lung, 184:159–67.
Puente-Maestu L, SantaCruz A, Vargas T, et al. 2003. Effects of training on
the tolerance to high-intensity exercise in patients with severe COPD.
Respiration, 70:367–70.
Puente-Maestu L, Sánz ML, Sánz P, et al. 2000. Comparison of effects of
supervised versus self-monitored training programs in patients with chronic
obstructive pulmonary disease. Eur Respir J, 15: 517–25.
Ramirez-Venegas A, Ward J, Lentine T, et al. 1997. Salmeterol reduces
dyspnoea and improves lung function in patients with COPD. Chest,
112:336–40.
International Journal of COPD 2006:1(4)
Ranieri VM, Dambrosio M, Brienza N. 1996. Intrinsic PEEP and
cardiopulmonary interaction in patients with COPD and acute
ventilatory failure. Eur Respir J, 9:1283–92.
Ranieri VM, Giuliani R, Cinnella G, et al. 1993. Physiologic effects of positive
end-expiratory pressure in patients with chronic obstructive pulmonary
disease during acute ventilatory failure and controlled mechanical
ventilation. Am Rev Respir Dis, 147:5–13.
Rodrigo G, Rodrigo C, Pollack C, et al. 2001. Helium-oxygen mixture for
nonintubated acute asthma patients (Cochrane Review). Cochrane
Database Syst Rev, 1:CD002884.
Rodrigo GJ, Rodrigo C, Pollack CV, et al. 2003. Use of helium-oxygen
mixtures in the treatment of acute asthma: a systematic review. Chest,
123:891–6.
Rogers RM, DuBois AB, Blakemore WS. 1968. Effect of removal of bullae
on airway conductance and conductance volume ratios. J Clin Invest,
47:2569–79.
Rossi A, Ganassini A, Polese G, et al. 1997. Pulmonary hyperinflation and
ventilator-dependent patients. Eur Respir J, 10:1663–74.
Roussos C, Macklem PT. 1982. The respiratory muscles. N Engl J Med,
307:786–97.
Ruiz de Oña Lacasta JM, Garcia de Pedro J, Puente-Maestu L, et al. 2004.
Effects of muscle training on breathing pattern in patients with severe
chronic obstructive pulmonary disease. Arch Bronconeumol, 40:20–3.
Saetta M, Baraldo S, Corbino L, et al. 1999. Am J Respir Crit Care Med,
160:711–17.
Saetta M, Turato G, Maestrelli P, et al. 2001. Cellular and structural bases
of chronic obstructive pulmonary disease. Am J Respir Crit Care Med,
163:1304–9.
Saksena FB, Burrows B. 1966. Thoracic compliance in chronic obstructive
lung disease. J Lab Clin Med, 68:427–32.
Salvi S, Blomberg A, Rudell B, et al. 1999. Acute inflammatory responses
in the airways and peripheral blood after short-term exposure to diesel
exhaust in healthy human volunteers. Am J Respir Crit Care Med,
159:702–9.
Schumaker GL, Epstein SK. 2004. Managing acute respiratory failure
during exacerbation of chronic obstructive pulmonary disease. Respir
Care, 49:766–82.
Shapiro SD, Senior RM. 1999. Matrix metalloproteinases: matrix degradation and more. Am J Respir Cell Mol Biol, 20:1100–2.
Sharp JT, Van Lith P, Vej Nughprayoon C, et al. 1968. The thorax in chronic
obstructive lung disease. Am J Med, 44:39–46.
Shindoh C, Hida W, Kikuchi Y, et al. 1994. Oxygen consumption of respiratory muscles in patients with COPD. Chest, 105:790–7.
Similowski T, Yan S, Gauthier AP, et al. 1991. Contractile properties of
the human diaphragm during chronic hyperinflation. N Engl J Med,
325:917–23.
Somfay A, Porszasz J, Lee SM, et al. 2001. Dose-response effect of oxygen
on hyperinflation and exercise endurance in nonhypoxaemic COPD
patients. Eur Respir J, 18:77–84.
Spahija J, de Marchie M, Grassino A. 2005. Effects of imposed pursed-lips
breathing on respiratory mechanics and dyspnoea at rest and during
exercise in COPD. Chest, 128:640–50.
Stevenson NJ, Calverley PM. 2004. Effect of oxygen on recovery from
maximal exercise in patients with chronic obstructive pulmonary
disease. Thorax, 59:668–72.
Stevenson NJ, Walker PP, Costello RW, et al. 2005. Lung mechanics and
dyspnoea during exacerbations of chronic obstructive pulmonary
disease. Am J Respir Crit Care Med, 172:1510–16.
Stockley RA. 1999. Neutrophils and protease/antiprotease imbalance. Am
J Respir Crit Care Med, 160:S49–S52.
Stocks J, Quanjer PH. 1995. Reference values for residual volume, functional
residual capacity and total lung capacity. ATS Workshop on Lung
Volume Measurements. Official Statement of the European Respiratory
Society. Eur Respir J, 8:492–506.
Stubbing DG, Pengelly LD, Morse JL, et al. 1980. Pulmonary mechanics
during exercise in normal males. J Appl Physiol, 49:506–10.
399
�Puente-Maestu and Stringer
Suratt BT, Cool CD, Serls AE, et al. 2003. Human pulmonary chimerism
after hematopoietic stem cell transplantation. Am J Respir Crit Care
Med, 168:318–22.
Swidwa DM, Montenegro HD, Goldman MD, et al. 1985. Helium-oxygen
breathing in severe chronic obstructive pulmonary disease.Chest,
87:790–5.
Takayama T, Shindoh C, Kurokawa Y, et al. 2003. Effects of lung volume
reduction surgery for emphysema on oxygen cost of breathing. Chest,
123:1847–52.
Tassaux D, Jolliet P, Roeseler J, et al. 2000. Effects of helium-oxygen on
intrinsic positive end-expiratory pressure in intubated and mechanically
ventilated patients with severe chronic obstructive pulmonary disease.
Crit Care Med, 28:2721–8.
Thoman RL, Stoker GL, Ross JC. 1966. The efficacy of pursed-lips breathing in patients with chronic obstructive pulmonary disease. Am Rev
Respir Dis, 93:100–6.
Thurlbeck W. 1991. Pathology of chronic airflow obstruction. In: Cherniack
N (ed). Chronic obstructive pulmonary disease. Philadelphia: WB
Saunders, pp 3–20.
Thurlbeck WM. 1985. Chronic airflow obstruction. Correlation of structure
and function. 1985 in Petty TL (ed). Chronic obstructive pulmonary
disease. New York: Marcel Dekker, pp 129–204.
Tiep BL, Burns M, Kao D, et al. 1986. Pursed lips breathing training using
ear oximetry. Chest, 90:218–21.
Tobin MJ, Hughes JA, Hutchison DC. 1984. Effects of ipratropium
bromide and fenoterol aerosols on exercise tolerance. Eur J Respir
Dis, 65:441–6.
Tojo N, Ichioka M, Chida M, et al. 2005. Pulmonary exercise testing predicts
prognosis in patients with chronic obstructive pulmonary disease.
Intern Med, 44:20–5.
Valta P, Corbeil C, Lavoie A, et al. 1994. Detection of expiratory flow
limitation during mechanical ventilation. Am J Respir Crit Care Med,
150:1311–17.
van’t Hul AJ, Kwakkel G, Gosselink R. 2002. The acute effects of noninvasive ventilatory support during exercise on exercise endurance and
dyspnoea in patients with COPD: a systematic review. J Cardiopulm
Rehabil, 22:290–7.
van’t Hul A, Gosselink R, Hollander P, et al. 2004. Acute effects of
inspiratory pressure support during exercise in patients with COPD.
Eur Respir J, 23:34–40.
400
Vestbo J, Prescott E, Lange Pl; the Copenhagen City Heart Study Group.
1996. Association of chronic mucus hypersecretion with FEV1 line
and chronic obstructive pulmonary disease morbidity. Am J Respir
Crit Care Med, 153:1530–5.
Vogiatzis I, Georgiadou O, Golemati S, et al. 2005. Patterns of dynamic
hyperinflation during exercise and recovery in patients with severe
chronic obstructive pulmonary disease. Thorax, 60:723–9.
Vogiatzis I, Nanas S, Kastanakis E, et al. 2004. Dynamic hyperinflation
and tolerance to interval exercise in patients with advanced COPD.
Eur Respir J, 24:385–90.
Vogiatzis I, Nanas S, Roussos C. 2002. Interval training as an alternative
modality to continuous exercise in patients with COPD. Eur Respir
J, 20:12–19.
Von Essen SG, O’Neill DP, McGranaghan S, et al. 1995. Neutrophilic
respiratory tract inflammation and peripheral blood neutrophilia after
grain sorghum dust extract challenge. Chest, 108:1425–33.
Wakabayashi A, Brenner M, Kayaleh RA, et al. 1991. Thoracoscopic carbon
dioxide laser treatment of bullous emphysema. Lancet, 337:881–3.
Woodcock AA, Gross ER, Geddes DM. 1981. Oxygen relieves breathlessness in “pink puffers”. Lancet, i:907–9.
Woodcock AA, Gross ER, Gellert A, et al. 1981. Effects of dihydrocodeine,
alcohol, and caffeine on breathlessness and exercise tolerance in patients
with chronic obstructive lung disease and normal blood gases. N Engl
J Med, 305:1611–16.
Yamamoto C, Yoneda T, Yoshikawa M, et al. 1997. Airway inflammation in COPD assessed by sputum levels of interleukin-8. Chest,
112:505–10.
Yan S, Kaminski D, Sliwinski P. 1997. Reliability of inspiratory capacity
for estimating end-expiratory lung volume changes during exercise in
patients with chronic obstructive pulmonary disease. Am J Resp Crit
Care Med, 156:55–9.
Younes M, Kivinen G. 1984. Respiratory mechanics and breathing pattern
during and following maximal exercise. J Appl Physiol, 57:1773–82.
Younes M, Riddle W. 1981. A model for the relation between respiratory
neural and mechanical outputs. I. Theory. J Appl Physiol, 51:963–78.
Younes M. 1991.Determinants of thoracic excursion during exercise. In:
Whipp BJ, Wasserman K (eds). Exercise pulmonary physiology and
physiopathology. New York: Marcel Dekker, pp 1–65.
International Journal of COPD 2006:1(4)
�
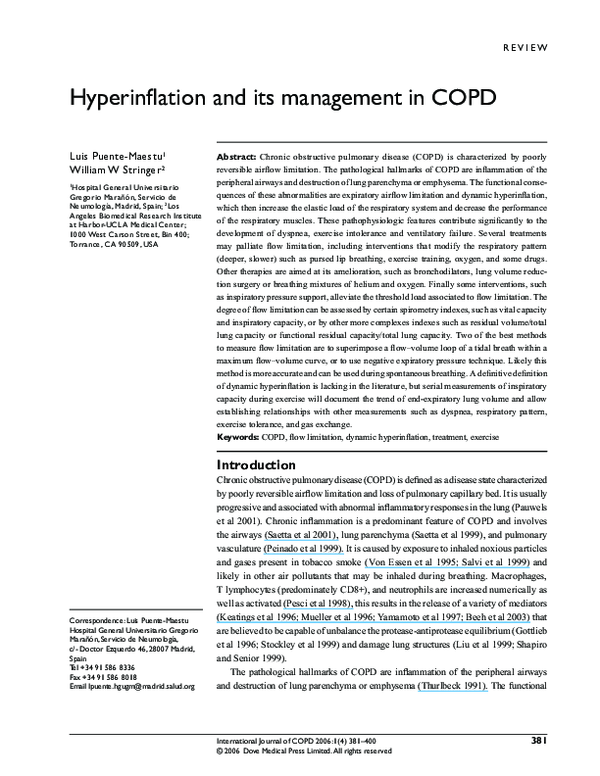
 Luis Puente-maestu
Luis Puente-maestu