Pflugers Arch - Eur J Physiol (2011) 462:219–233
DOI 10.1007/s00424-011-0970-1
CARDIOVASCULAR PHYSIOLOGY
Post-ischemic early acidosis in cardiac postconditioning
modifies the activity of antioxidant enzymes, reduces
nitration, and favors protein S-nitrosylation
Claudia Penna & Maria-Giulia Perrelli & Francesca Tullio & Francesca Moro &
Maria Laura Parisella & Annalisa Merlino & Pasquale Pagliaro
Received: 3 March 2011 / Revised: 14 April 2011 / Accepted: 18 April 2011 / Published online: 5 May 2011
# Springer-Verlag 2011
Abstract Postconditioning (PostC) modifies the early postischemic pH, redox environment, and activity of enzymes. We
hypothesized that early acidosis in PostC may affect superoxide dismutase (SOD) and catalase (CAT) activities, may reduce
3-nitrotyrosine (3-NT) protein levels, and may increase Snitrosylated (SNO) protein levels, thus deploying its protective
effects. To verify this hypothesis, we studied the early (7th min)
and late (120th min) phases of reperfusion (a) endogenous
SOD and CAT activities and (b) 3-NT protein levels and
SNO protein levels. Isolated rat hearts underwent 30-min
ischemia/120-min reperfusion (I/R) or PostC (5 cycles of 10-s
I/R at the beginning of 120-min reperfusion) either with or
without exogenous CAT or SOD infused during the initial
3 min of reperfusion. The effects of early reperfusion with
acid buffer (AB, pH 6.8) on endogenous antioxidant enzymes
were also tested. Pressure, infarct size, and lactate dehydrogenase release were also measured. At the 7th min, PostC
C. Penna : M.-G. Perrelli : F. Tullio : F. Moro : A. Merlino :
P. Pagliaro
Department of Biological and Clinical Sciences,
University of Torino,
Orbassano, Turin, Italy
C. Penna : M.-G. Perrelli : F. Tullio : F. Moro : P. Pagliaro
National Institute of Cardiovascular Research (INRC),
Bologna, Italy
M. L. Parisella
Department of Pharmaco-Biology, University of Calabria,
Arcavacata di Rende, Cosenza, Italy
P. Pagliaro (*)
Dipartimento di Scienze Cliniche e Biologiche,
Università di Torino,
Regione Gonzole 10,
10043 Orbassano, Turin, Italy
e-mail: pasquale.pagliaro@unito.it
induced a significant decrease in SOD activity with no major
change both in Mn and Cu/Zn SOD levels and in CAT
activity and level. PostC also reduced 3-NT and increased
SNO levels. Exogenous SOD, but not CAT, abolished PostC
cardioprotection. In late reperfusion (120-min), I/R increased
SOD activity but decreased CAT activity and Cu/Zn SOD
levels; these effects were reversed by PostC; 3-NT was not
affected, but SNO was increased by PostC. AB reproduced
PostC effects on antioxidant enzymes. The conclusions are as
follows: PostC downregulates endogenous SOD and preserves CAT activity, thus increasing SNO and reducing 3-NT
levels. These effects are triggered by early post-ischemic
acidosis. Yet acidosis-induced SOD downregulation may
limit denitrosylation, thus contributing to PostC triggering.
Hence, exogenous SOD, but not CAT, interferes with PostC
triggering. Prolonged SOD downregulation and SNO increase
may contribute to PostC and AB beneficial effects.
Keywords Cardioprotection . Infarction . Ischemia .
Postconditioning . Reperfusion injury
Introduction
Clearly, the only way to limit ischemia damage is organ
reperfusion. However, with reperfusion, injury amplification (i.e., reperfusion injury) occurs. In fact, in early postischemic phase, mitochondrial permeability transition pore
(mPTP) formation may be the event that would lead to
irreversible changes in cellular function and cell death, e.g.,
[4, 9, 26, 27, 34]. At the onset of a rapid reperfusion, when
a large increase in reactive oxygen species (ROS) formation
occurs along with pH recovery and Ca2+ overload, mPTP
opening is facilitated. This, in turn, favors massive ROS
formation by inhibiting the respiratory chain [26, 27, 34].
�220
Therefore a vicious cycle is likely to be established in the
so-called ROS-induced ROS release (RIRR) [26, 27, 34],
thus inducing ROS stress and reperfusion injury (for
reviews, see [46, 50]). Survival mechanisms in the heart
can be triggered by short, non-lethal periods of ischemia
and reperfusion, applied either before (preconditioning) or
immediately after (postconditioning, PostC) the index
ischemia [3, 10, 20, 25, 33, 44–46, 62]. Both in vivo and
in vitro ischemic and pharmacological preconditioning
triggering require protective ROS signaling. In fact, either
ROS generators or ROS scavengers, given before the index
ischemia, trigger or abolish preconditioning [2, 7, 10, 16,
23, 43, 47, 48, 61]. Therefore, ROS are double-edge swords
(ROS stress vs. ROS signaling). Also, PostC protection
requires ROS signaling and delayed recovery of intracellular pH during initial reperfusion. The mechanisms by which
PostC alters the pathophysiology of reperfusion injury
involve molecular and physiological mechanisms, such as
delaying re-alkalinization of tissue pH [8, 9, 17, 29, 30, 55],
triggering the release of ROS and autacoids [13, 46, 50–52,
54, 61], and activation of kinases that impact cellular and
subcellular targets or effectors, such as mPTP (e.g., [20, 46,
50, 52]). Importantly, acid buffer (AB) given for the first
few minutes of reperfusion is as protective as a PostC
protocol [8, 9, 13, 17, 29, 30, 34, 55]. This supports the
idea that the delayed recovery of intracellular pH during
initial reperfusion is mandatory to limit infarct size in PostC
mainly via the prevention of mPTP opening and prevention
of RIRR [8, 9, 17, 29, 30, 34, 55]. Both in vitro and in vivo
studies demonstrated that large-spectrum ROS scavengers
such as N-acetyl-L-cysteine (NAC) and/or N-(2-mercaptopropionyl)-glycine (MPG) given either during the PostC
maneuvers [8, 51, 54, 63] or during AB infusion [8–10, 13]
prevented their protective effects [13, 51, 54, 63]. Moreover, addition of alkaline buffer in early reperfusion
abolishes both AB and PostC protection [8, 9, 17, 29,
55]. Therefore, it is likely that interplays between redox and
acid/base conditions in early reperfusion exist. Clearly, the
PostC cycles (i.e., intermittent re-oxygenation) and the
early acidosis may be responsible of modifications of
enzyme activities and chemical reactions, which could lead
to produce a few ROS with signaling role instead of ROS
stress [13, 51, 53].
PostC protection is also influenced by the interplay
between endothelial and cardiac function, with a flow of
nitric oxide (NO•) from endothelium to myocardium [20,
46, 50, 67]. Indeed the persistence of acidosis is important
for non-enzymatic NO• production [59, 69] so that ROS in
concert with NO• and reactive nitrogen species (RNS) may
put the heart into a protected state [26, 38, 46, 49–52, 63].
Actually, in addition to activating cyclic guanosine
monophosphate/protein kinase G-dependent signaling pathways, NO• and RNS can modify sulfhydryl residues of
Pflugers Arch - Eur J Physiol (2011) 462:219–233
protein through S-nitrosylation, which has emerged as an
important post-translational protein modification [11, 24,
40, 56, 57]. Nitrosylation has been proposed to be
important in the preconditioning cardioprotection, also
modifying mitochondrial proteins and limiting oxidative
stress [6, 36, 56, 57]. Although PostC requires NO• [28, 29,
33, 49, 52], nitrosylation has not been studied under this
condition [56]. Yet, the studies on nitration of proteins with
3-nitrotyrosine concentration (a marker for ONOO− formation) achieved contradictory results: while Kupai et al. [32]
reported that PostC increases cardiac 3-NT after 5 min of
reperfusion, Iliodromitis et al. [28] observed that PostC
reduces the myocardial and circulating levels of 3-NT after
10 min of reperfusion. Wang et al. [65] also observed a
decrease in ONOO− formation after hypoxic PostC.
Moreover, we have been unable to reproduce cardioprotection with ROS generator given during early reperfusion
[51]. Since ROS scavengers (NAC or MPG) abolish ABand PostC-induced protection [8, 9, 51, 54, 63], it is likely
that the type, the concentration, and/or the compartmentalization of ROS/RNS may play a pivotal role in triggering
protection at early reperfusion time. To shed some light on
this scenario, we studied antioxidant enzymes, nitration,
and S-nitrosylation of proteins.
Many endogenous enzymes regulate the homeostasis of
ROS/RNS. In the myocardium, three iso-forms of superoxide dismutases (SOD), which convert superoxide (O2−)
to hydrogen peroxide (H2O2), have been described. The
steady-state levels of H2O2 by conversion to water are
regulated by enzymes such as catalase (CAT) and glutathione peroxidase (GPx) [35, 64]. Importantly, the activity and
levels of endogenous antioxidant iso-enzymes are differently affected by ischemia/reperfusion (I/R) in the various
tissues and compartments [12, 37]. Yet, little is known
about the activity of antioxidant enzymes during PostC in
the cardiac tissue.
While the optimal pH is 7.0 for CAT activity, it is 7.8 for
SOD. Intriguingly, SOD is also a de-nitrosylating enzyme
in different systems [21, 42, 56]. Therefore, we hypothesized that intracellular acidosis during PostC and AB in
early reperfusion may downregulate SOD activity and may
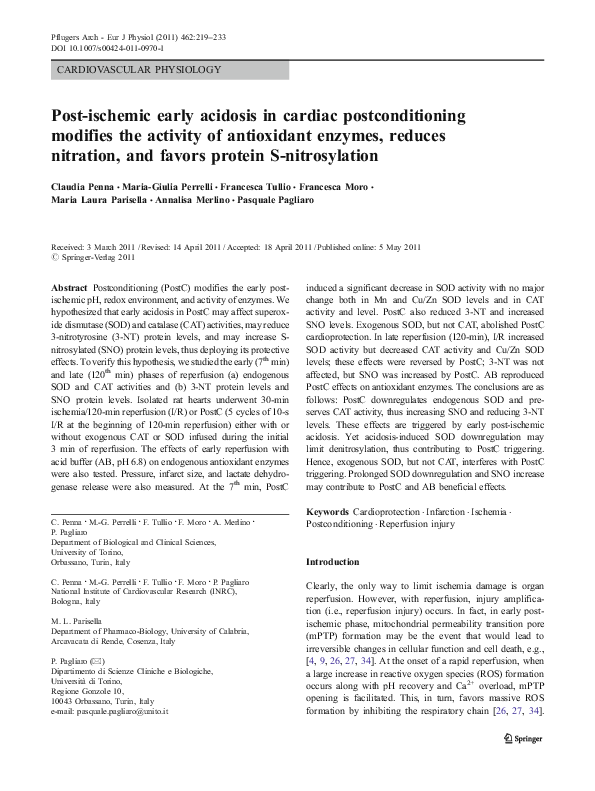
lead to modifications of 3-NT and SNO levels (Fig. 1). We
also hypothesized that a delicate balance between acidosis,
ROS/RNS, the S-nitrosylation, and nitration/oxidation may
occur in early reperfusion [52, 56]. It is, thus, likely that the
presence of additional specific antioxidant (SOD or CAT)
would alter differently the delicate balance induced by
PostC maneuvers in early reperfusion. It is also likely that
when post-ischemic pH is recovered in late reperfusion,
enzyme activity is also recovered.
Therefore, in the present study, we assessed: (1) the
ability of two specific antioxidant enzymes (exogenous
SOD or CAT) given during early reperfusion to abolish
�Pflugers Arch - Eur J Physiol (2011) 462:219–233
221
PostC (early acidotic reperfusion)
O2-
Intermittent reintroduction of O2
Early acidosis
Hypotheses
Flow of reactions
Established facts
Non en
z ym
produc atic
tion
SOD
H2 O2
CAT H2O
Early acidosis
NO.
Cysteine
oxidation
eNOS activation
ONOOP-Tyr-3-NO2
Tyrosine nitration
NO
De
N2O3
GS
SOD
ni
tro
sy
la
tio
n
Secondary
reaction
P-SNO
S-nitrosylation
Fig. 1 Suggested schematic chemical relationship among different
reactive oxygen species and reactive nitrogen species in PostC and early
acidotic reperfusion. The scheme represents a summary of (1) established
facts, (2) well-known flow of chemical reactions, and (3) hypotheses; two
dotted verticals lines divide the scheme in these three elements. The
scheme is built starting from the evidences that in early reperfusion
postconditioning (PostC) are characterized by intermittent reintroduction of O2, reactive oxygen species signaling, persistence of
acidosis, and nitric oxide (NO•) production by endothelial nitric oxide
synthase (eNOS) and non-enzymatic processes [8, 9, 17, 20, 28–30, 46,
50, 55, 56, 65]. Based on superoxide (SOD) optimal pH (7.8) and
catalase (CAT) optimal pH (7.0), the scheme suggests the hypotheses of
SOD down-regulation (arrow down) and CAT up-regulation (arrow up)
by the early acidosis, which may be a key event for PostC
cardioprotection [8, 9, 17, 29, 30, 55]. In the excess of NO•, the
secondary reaction between ONOO− and NO• may increase [60, 66] and
this might favor S-nitrosylation; SOD down-regulation may limit denitrosylation. Therefore, a reduction in tyrosine nitration (arrow down)
and an increase in S-nitrosylation (arrow up) are also suggested. In the
scheme, the processes, the enzyme activities and the reactions
hypothetically decreased/reduced by PostC/acidosis are in dashed lines.
GSNO S-nitrosoglutathione (see text for further explanation)
PostC triggering, (2) the activity and the level of endogenous SOD and CAT in early and late reperfusion either after
PostC or early AB infusion, and (3) the effects of PostC
with and without exogenous SOD on the levels of 3-NT and
SNO proteins in early and late reperfusion.
Male Wistar rats (5–6 months old) (Janvier S.A.S., St
Berthevin Cedex, France) received humane care in compliance with Italian law (DL-116, Jan. 27, 1992) and in
compliance with the Guide for the Care and Use of
Laboratory Animals published by the US National Institutes of Health (NIH Publication No. 85-23, revised 1996).
retrogradely perfused with oxygenated Krebs–Henseleit
buffer (127 mM NaCl, 17.7 mM NaHCO3, 5.1 mM KCl,
1.5 mM CaCl2, 1.26 mM MgCl2, 11 mM D-glucose
(Sigma-Aldrich Corp., St. Louis, MO, USA), and gassed
with 95% O2 and 5% CO2). A constant flow was adjusted
with a pump to obtain a perfusion pressure of 80–85 mmHg
during stabilization. Thereafter, the same flow level (9±
1 ml/min/g) was maintained throughout the experiment.
A balloon was placed into the left ventricle and
connected to an electromanometer to record left ventricular
pressure (LVP). The balloon was filled with saline to
achieve an end-diastolic LVP (EDLVP) of 5 mmHg.
Coronary perfusion pressure, coronary flow, EDLVP, and
developed LVP (DevLVP) were monitored to assess the
preparation conditions. The hearts were electrically paced at
280 bpm and kept in a temperature-controlled chamber (37°
C).
Isolated heart perfusion
Experimental protocols (Fig. 2)
The methods were similar to those previously described
[45, 50–54]. In brief, each animal was anesthetized. Then,
10 min after heparin treatment, the heart was rapidly
excised, weighed, attached to the perfusion apparatus, and
After 30 min of stabilization, hearts were subjected to a
specific protocol, which was the same for all groups and
included 30 min of global, normothermic ischemia and
120 min of reperfusion followed by 30 min of ischemia (see
Materials and methods
Animals
�222
Fig. 2 Experimental design. The
isolated, Langendorff-perfused
hearts were stabilized for 30-min
(Stab) and then subjected to
30 min of normothermic, global
ischemia (I) followed by 120-min
of reperfusion (R). Postconditioning (PostC) protocol (5
cycles 10-s ischemia/reperfusion)
is indicated by vertical lines at
the beginning of the reperfusion
period. Treatment with exogenous active or inactivated
antioxidant enzymes: either
catalase (CAT, CATi) or
superoxide dismutase (SOD,
SODi) has been infused for 3 min
during early reperfusion, as
indicated by horizontal black
lines. In additional experiments
(Sham, I/R, PostC, and acid
buffer), the activity of CAT and
SOD was tested at specific
time-points (baseline, 7 min, and
120 min after the beginning of
reperfusion; Sham hearts were
tested at corresponding
time-points of perfusion only as
indicated by the arrows; for
further explanation, see text)
Pflugers Arch - Eur J Physiol (2011) 462:219–233
Experimental Design
I/R, Group 1
Stab
I (30 min)
Stab
I (30 min)
R (120 min)
PostC, Group 2
R (120 min)
PostC+CAT, Group 3; PostC+SOD, Group 4;
Stab
I (30 min)
R (120 min)
I/R+CAT, Group 5; I/R+SOD, Group 6.
Stab
I (30 min)
R (120 min)
PostC+ CATi, Group 7; PostC+ SODi, Group 8
Stab
I (30 min)
R (120 min)
3 min
Additional experiments
Sham
Buffer Perfusion
I/R
Stab
I (30 min)
R (120 min)
PostC
Stab
I (30 min)
R (120 min)
AB
Stab
I (30 min)
baseline
below). Pacing was discontinued on initiation of ischemia
and restarted after the 3rd minute of reperfusion in all
groups [44, 50–54]. After stabilization, the hearts of the
control group (I/R, group 1, n=12) were exposed to 30 min
of ischemia and then to 120 min of reperfusion only. In
group 2 (PostC group; n=12), after the 30-min ischemia,
the hearts immediately underwent a protocol of PostC (i.e.,
5 cycles of 10-s reperfusion and ischemia) [50–54].
Antioxidants, either CAT or SOD (Sigma-Aldrich Corp.,
USA), were given at the beginning of reperfusion for 3 min,
with and without PostC, at doses previously used in
isolated rat hearts [1]. In particular, group 3 (PostC+CAT,
n=10) and group 4 (PostC+SOD, n=10) hearts underwent
I/R plus PostC, in the presence of CAT (100 U/ml) or SOD
(10 U/ml), respectively; group 5 (I/R+CAT, n=9) and group
6 (I/R+SOD, n=9) hearts underwent I/R only in the
presence of CAT (100 U/ml) or SOD (10 U/ml), respectively [1].
For comparative purposes, the hearts were also perfused
in the presence of PostC maneuvers with heat-inactivated
CAT (100 U/ml; PostC+CATi, group 7, n=6) or heat-
R (120 min)
7th
120th min
inactivated SOD (10 U/ml; PostC+SODi, group 8, n=6).
The inactivated enzymes were infused at the beginning of
reperfusion for 3 min. Heat inactivation was obtained as
previously described and confirmed by spectrophotometer
analysis. Non-heated exogenous enzymes were normally
active [14, 58].
In other experiments (n=4 for each group), hearts
underwent either I/R or PostC in the presence of SOD
(10 U/ml) plus CAT (100 U/ml) co-infused for an initial
3 min of reperfusion (not shown in Fig. 2).
CAT and SOD activities and levels
Additional hearts (Fig. 2; n=6 for each group) were
subjected to 180-min perfusion only (i.e., Sham), I/R only,
PostC, or AB (pH 6.8) in early reperfusion. AB method was
identical to that reported by Rodríguez-Sinovas et al. [55].
In these hearts, the activities and levels of endogenous CAT
and SOD were tested at specific time-points (baseline,
7 min, and 120 min after the beginning of reperfusion;
Sham hearts were tested at corresponding time-points of
�Pflugers Arch - Eur J Physiol (2011) 462:219–233
223
Homogenization protocol: in order to check the protein
levels, samples of Sham, I/R, PostC, and AB hearts (n=6
for each group) were homogenized on ice in RIPA lysis
buffer (Santa Cruz Biotechnology) using a polytron tissue
grinder. The homogenate was centrifuged at 4°C for 30 min
at 13,000 g, and the supernatant was collected to quantify
proteins with Bradford’s method [5]. Western blot analyses
were performed as previously described [53].
with Bradford’s method [5], and the biotin switch assay
with or without ascorbate (1 mM) was performed as
previously described [31]. In particular, blocking buffer
(225 mmol l−1 Hepes, pH 7.7, 0.9 mmol l−1 EDTA,
0.09 mmol l−1 neocuproine, 2.5% SDS, and 20 mmol l−1
MMTS) and HENS buffer (250 mmol l−1 Hepes, pH 7.7,
1 mmol l−1 EDTA, 0.1 mmol l−1 neocuproine, and 1%
SDS) were used (Sigma-Aldrich Corp) [31].
To detect biotinylated proteins by Western blot, samples
from the biotin switch assay were separated on 12% SDS–
PAGE gels, transferred to PVDF membranes (GE Healthcare
Biosciences Piscataway, NJ, USA), blocked with non-fat
dried milk (Santa Cruz, CA, USA), and incubated with
streptavidin peroxidase, diluted at 1/10,000 for 1 h. In order to
ascertain that variations of nitrosylation occur within cells, Snitrosylations of cardiac electron transfer flavoprotein α,β
(ETFAα,β) and von Willebrand Factor (vWF) were tested in
separated assays (two samples, for two hearts for each group):
after detection of biotin, the membranes were stripped and
reincubated with polyclonal antibodies against ETFAα,β
(Santa Cruz, CA, USA) and vWF (Dako, Denmark) [18,
19]. vWF was tested because of its localization within
endothelial cells and ETFAα,β was tested because the
mitochondrial proteins extracted from whole hearts originate
mainly from cardiomyocytes. To confirm equal protein
loading, membranes were incubated with an anti-β-actin
antibody (Sigma-Aldrich Corp). The S-immunoblotted proteins were visualized by using Immuno-Star HRP Substrate
Kit (Bio-Rad Laboratories) and quantified by Kodak Image
Station 440CF. Image analyses were performed by the
Kodak 1D 3.5 software.
S-nitrosylated and 3-nitrotyrosine myocardial protein levels
3-Nitrotyrosine assay
Hearts (n=6 for each group) subjected to I/R only, PostC,
PostC+SOD, or perfusion only (i.e., Sham) were used to
assess the levels of S-nitrosylated and 3-NT at baseline,
7 min after the beginning of reperfusion and at the end of
reperfusion; Sham hearts were tested at corresponding timepoints of perfusion only.
The protein concentrations of the samples were quantified with
Bradford’s method [5]. Nitrotyrosine, as a marker of nitrosative stress, was measured with a competitive enzyme
immunoassay: the levels of 3-NT were measured according
to the manufacturer’s directions using Cell Biolabs kit (Cell
Biolabs, Inc., San Diego, CA, USA). The detection sensitivity
range was 20 nM to 8 μM of 3-nitrotyrosine-BSA equivalent.
perfusion only). The 7-min reperfusion time-point was
employed on the basis of previous studies on PostC
triggering [4, 39, 62].
CAT and SOD activities by spectrophotometric analysis
Activity was analyzed according to the manufacturer’s
directions using Cayman chemical kits (Ann Arbor, MI,
USA). Briefly, tissues from the heart of rats were
homogenized, cell debris was pelleted, and the resulting
supernatants were used for the enzyme activity assays. CAT
and SOD activities were measured at 540- and 450-nm
wavelengths, respectively. A unit of CAT activity was
defined as the amount of enzyme that caused the formation
of 1.0 nmol of formaldehyde per minute at 25°C. A unit of
SOD activity was defined as the amount of SOD needed to
exhibit 50% dismutation of the produced superoxide radical
at 25°C. The final enzymatic activities were calculated by
normalizing the results to the total protein concentration of
the whole extract.
CAT and SOD levels by Western blot analysis
Biotin switch assay and Western blot for the detection
of S-nitrosylated proteins
Assessment of myocardial injury
All preparative procedures were performed in the dark to
prevent light-induced cleavage of nitrosylations [31]. Heart
samples, collected at specified time-points, were homogenized and centrifuged on ice in appropriate buffers
(20 mmol l−1 Tris, pH 7.5, 150 mmol l−1 NaCl, 1%
Igepal CA 630, 0.5% sodium deoxycholate, 1 mmol l−1
EDTA, 0.1% SDS, 200 mmol l−1 sodium orthovanadate,
and protease inhibitor cocktail (Sigma-Aldrich Corp.))
using a polytron tissue grinder. Proteins were quantified
Since in isolated hearts the pre- and postconditioning are
known to reduce the release of lactate-dehydrogenase
(LDH) during reperfusion, the release of LDH was
measured during the 2 h of reperfusion as previously
described [45, 49, 51, 53]. Infarct areas were also assessed
at the end of the experiment with the nitro-blu-tetrazolium
technique (Sigma-Aldrich) as described [45, 49, 51, 53,
54]. The necrotic mass was expressed as a percentage of
total left ventricular mass (i.e., risk area).
�224
Pflugers Arch - Eur J Physiol (2011) 462:219–233
Statistical analysis
All data are expressed as means±S.E.M. One-way ANOVA
and Newman–Keuls multiple comparison test (for postANOVA comparisons) were used to evaluate the statistical
significance among groups. A p value <0.05 was considered
as statistically significant.
Results
PostC improvement of cardiac function was abolished
by exogenous SOD
Table 1 shows I/R (group 1) as having markedly increased
CPP and EDLVP and drastically reduced DevLVP. PostC
(group 2) limited CPP increase and improved the recovery of
DevLVP by attenuating the increase in EDLVP during
reperfusion. While CAT (group 3) did not affect the PostCinduced improvement of function, SOD (group 4) abolished
these protective effects of PostC. The treatment with either
CAT or SOD during the first 3 min of reperfusion in the
I/R+CAT or I/R+SOD hearts (groups 5 and 6, respectively)
did not significantly change the deleterious effects of I/R on
mechanical function. Moreover, the treatment with inactivated enzymes (CATi or SODi) in the PostC+CATi or
PostC+SODi hearts (groups 7 and 8, respectively) did not
significantly change the beneficial effects of PostC on postischemic function.
PostC reduction in infarct size and LDH release
were reversed by exogenous SOD
Infarct size (Fig. 3a), expressed as a percentage of risk area,
was 61 ± 5% in control (group 1); PostC (group 2)
significantly reduced the infarct size to 34±5% (p<0.01
vs. control). PostC+CAT (group 3) induced a significant
reduction of infarct size to 37±5% (p<0.01 vs. control; NS
vs. PostC; Fig. 3a). In PostC+SOD (group 4), the infusion
of exogenous SOD abolished the cardioprotection by PostC
(infarct size 73±8%, p = NS vs. control).
The treatment with either CAT or SOD in the I/R+CAT or I/
R+SOD hearts (groups 5 and 6, respectively) did not
significantly change the infarct size (71±9% and 77±5%,
respectively) with respect to the control (Group 1). In hearts of
Groups 7 and 8 with inactivated enzymes (PostC+CATi and
PostC+SODi, respectively), PostC maneuvers still induced
cardioprotection. In particular, infarct size was 36±11% in
PostC+CATi and 22±8% of risk area in PostC+SODi (p = NS
vs. each other and vs. PostC, for both).
The infarct size data are corroborated by LDH release
during reperfusion (Fig. 3b). In fact, LDH release into the
coronary venous effluent was 969±53 U/g wet weight in
the control (group 1). LDH release was significantly
reduced by PostC (group 2; p<0.05 vs. control). Also in
PostC+CAT (group 3), a marked reduction of LDH release
(p<0.01 vs. control; p = NS vs. PostC) was observed.
However, in PostC+SOD (group 4), LDH release was not
different from that observed in control. In I/R+CAT (group
5) or I/R+SOD (group 6), LDH release was also similar to
that of control. In hearts of groups 7 and 8 (PostC+CATi
and PostC+SODi, respectively), PostC maneuvers still
reduced LDH release (p = NS vs. each other and vs. PostC,
for both; Fig. 3b).
In the experiments with the co-infusion of CAT+SOD
for an initial 3 min, either with or without PostC
maneuvers, both infarct size (78±5% and 69±4%, respectively) and LDH release (858±185 or 931±196 U/g,
respectively) resulted similar to those of control group
(data not reported in Fig. 3). Notably, once again, the
Table 1 Cardiac function parameters
Group
Before ischemia
CPP mmHg
At the end of reperfusion
LVEDP mmHg
DevLVP mmHg
CPP mmHg
LVEDP mmHg
DevLVP mmHg
Group 1 (I/R)
83±3
5±1
82±4
178±5
49±2
26±3
Group 2 (PostC)
82±3
5±2
84±5
115±7*
29±2*
45±3*
Group 3 (PostC+CAT)
80±2
6±2
74±5
125±9*
30±3*
46±2*
Group 4 (PostC+SOD)
85±4
4±1
73±1
180±3
47±2
22±1
Group 5 (I/R+CAT)
84±3
6±1
82±1
151±5
52±1
21±1
Group 6 (I/R+SOD)
86±3
5±1
77±9
170±4
45±2
26±1
Group 7 (PostC+CATi)
80±5
6±2
75±52
110±4*
31±5*
42±5*
Group 8 (PostC+SODi)
86±4
5±1
77±5
127±5*
30±2*
41±3*
There are no differences among groups before ischemia. At the end of reperfusion, all parameters are significantly (p<0.05 for all) different from
those observed before ischemia
CPP coronary perfusion pressure, LVEDP left ventricular end diastolic pressure, DevLVP developed left ventricular pressure
*p<0.05 vs. I/R group 1 at the end of reperfusion
�Pflugers Arch - Eur J Physiol (2011) 462:219–233
Infarct size
100
p = NS
75
**
PostC+CATi
I/R+SOD
I/R+CAT
PostC+SOD
PostC
25
I/R
**
**
**
PostC+
SODi
50
PostC+CAT
a
% of risk area
8
Gr
Gr
ou
p
ou
p7
ou
p
Gr
Gr
Gr
6
5
ou
p
4
ou
p
3
ou
p
2
Gr
LDH release
p = NS
p = NS
1500
p = NS
**
addition of exogenous SOD in reperfusion abolished PostC
protection.
Both PostC and AB reversed the increase in SOD activity
induced by I/R in early reperfusion
In the additional experiments, the basal activity of
endogenous CAT and SOD, detected after 30 min of
stabilization, was 106±2.4 mol/min/ml and 1.51±0.1 U/
ml, respectively. In Fig. 4, data are represented as percent
variation with respect to baseline level. No appreciable
changes in CAT and SOD activities with respect to baseline
level are observed on samples of Sham hearts collected
after a further 37 or 150 min of perfusion. These timepoints in Sham hearts correspond to the 7th and 120th min
of reperfusion in I/R and PostC hearts, i.e., the time-points
at which in the I/R, PostC, and AB groups the analysis of
enzyme activity was also measured.
As can be seen in the I/R samples, at the 7th minute of
reperfusion (Fig. 4a, b), the CAT activity was 98±2%
8
PostC+
SODi
PostC+CATi
**
ou
p
Gr
Gr
ou
p
7
I/R+SOD
ou
p6
ou
p
Gr
Gr
5
I/R+CAT
PostC+SOD
3
ou
p
Gr
ou
p
Gr
4
PostC
2
I/R
Gr
ou
p
1
0
*
PostC+CAT
*
500
ou
p
U/g ww
1000
Gr
b
Gr
ou
p
ou
p
1
0
Gr
Fig. 3 Analysis of ischemia/
reperfusion injury and cardioprotective effects on infarct size
and LDH release. a Infarct size
(percent of risk area). The
amount of necrotic tissue is
expressed as percent of the left
ventricle, which is considered as
the risk area. b LDH release.
The amount of LDH released
during reperfusion is expressed
as an international unit for
grams (wet weight) of hearts.
Groups are as in Fig. 1.
* p<0.05, **p<0.01 vs. Control
groups. NS non-significant.
Groups 1 and 2, n=12 each;
Groups 3 and 4, n=10 each;
Groups 5 and 6, n=9 each;
Groups 7 and 8, n=6 each
225
(p = NS vs. baseline and Sham) and SOD activity was
139±17% (p<0.05 vs. both baseline and Sham). Yet, in the
PostC samples, the CAT activity was 126±20% (p = NS vs.
its baseline and other groups) and SOD activity was 78±
4% of baseline (p<0.05 vs. baseline, Sham and I/R).
Notably, SOD activity resulted to about 50% lower than
that observed in I/R group. A similar trend in CAT and
SOD activity variation was observed after AB infusion
(Fig. 4a, b). In summary, at early reperfusion, PostC and
AB were associated with significant decreases in total SOD
activity with respect to I/R and with no significant change
in catalase activity.
Both PostC and AB prevented the decrease of CAT activity
and attenuated the increase in SOD activity induced by I/R
in late reperfusion
At the 120th minute of reperfusion (Fig. 4c, d), in the I/R
samples, the CAT activity was 50±10% (p<0.05 vs. baseline,
Sham and the 7th min) and SOD activity was 176±6%
�226
Antioxidant Enzyme Activity
a
c
Activity of catalase at 7th min
Activity of catalase at 120th min
p = NS
150
150
#
% of basal
% of basal
Fig. 4 Antioxidant enzyme activity in Sham, ischemia/reperfusion (I/R), postconditioning
(PostC) and acid buffer (AB)
hearts. a, b Catalase and superoxide dismutase (SOD), respectively, at the 7th min of
reperfusion. c, d Catalase and
superoxide dismutase (SOD),
respectively, at the 120th min of
reperfusion. Data are presented
as percent variation of baseline
level. §p<0.05, §§p<0.01 vs.
baseline level; *p<0.05,
**p<0.01 vs. Sham; #p<0.05
vs. I/R; $p<0.05, $$ p<0.01 vs.
corresponding group at the 7th
min of reperfusion. NS nonsignificant. n=6 for each group
Pflugers Arch - Eur J Physiol (2011) 462:219–233
100
50
§*$
50
0
0
Sham
PostC
AB
I/R
b
#
100
Activity of SOD at 7th min
d
Activity of SOD at 120th min
p = NS
p = NS
p = NS
200
200
§§** $$
100
50
0
(p<0.01 vs. baseline, Sham and the 7th min). That is, in I/R,
the variations of post-ischemic enzyme activities observed at
the 7th min are intensified at the 120th min. Yet, in the PostC
samples, the CAT activity was 88±9% (p = NS vs. baseline,
Sham and the 7th min; p<0.05 vs. I/R) and SOD activity was
123±5% (p<0.05 vs. baseline, Sham, I/R and the 7th min);
SOD and CAT activities were similarly affected by AB
infusion (Fig. 4c, d). That is, both PostC and AB prevent the
decrease of CAT activity and attenuate the increase in SOD
activity otherwise induced by I/R in late reperfusion.
Levels of CAT, Cu/Zn-SOD, and Mn-SOD were not
affected by either I/R, PostC, or AB in early reperfusion
An enzyme level analysis was performed before and after
(i.e., at the 7th and 120th min of reperfusion) the index
ischemia in I/R, PostC, and AB groups, as well as in
corresponding time-points in Sham group (Fig. 5). Notably,
Western blotting analysis of tissues revealed that, after the
7th min of reperfusion, there were no significant changes in
protein levels in all groups (Fig. 5a–c).
Levels of Cu/Zn-SOD were reduced only in I/R,
but not in PostC or AB, in late reperfusion
However, after 120 min of reperfusion, a significant
reduction (p<0.01 vs. Sham) of Cu/Zn-SOD was detected
#
§*#
% of basal
% of basal
§*
150
150
§*# $
*#
100
50
0
only in I/R; this was reversed by PostC and AB (p<0.01 vs.
I/R for both) (Fig. 5e). That is, in PostC, the levels of the
two SODs were similar to those of Sham and AB hearts.
The catalase levels were stable in all of the experimental
conditions tested. Data suggest that there is a leakage of the
cytoplasmatic Cu/Zn-SOD in late reperfusion, which was
prevented by PostC and AB. Other enzymes are confined in
the organelles and their levels do not change in any relevant
way. Alternatively, the initial variations in enzyme transcription activated by stress may be responsible of the
observed differences.
PostC reversed the reduction in S-nitrosylated protein levels
induced by I/R in a SOD-dependent manner in early
reperfusion
Nitrosylated protein levels were also studied before
ischemia, at the 7th and 120th min of reperfusion in I/R,
PostC, and PostC+SOD groups and at corresponding timepoints in Sham group (Fig. 6).
At the 7th min, the post-ischemic levels of S-nitrosylated
proteins were different from the baseline levels in both I/R
and PostC. As can be seen in Fig. 6a, in a broad range (5–
70 kDa), a lower amount of S-nitrosylated proteins was
present in I/R, whereas in PostC a higher grade of Snitrosylated proteins was observed. Their quantification is
shown in Fig. 6b: the amount of S-nitrosylated proteins was
�Pflugers Arch - Eur J Physiol (2011) 462:219–233
227
Fig. 5 Antioxidant enzyme protein levels analyzed by Western
blot in Sham, ischemia/reperfusion (I/R), postconditioning
(PostC), and acid buffer (AB)
hearts. a–c Mn/SOD, Cu–Zn/
SOD and catalase, respectively,
at 7th min of reperfusion. d–f
Mn/SOD, Cu–Zn/SOD and
Catalase, respectively, at 120th
min of reperfusion. Data in bar
graph are mean (± SE) and are
presented as percent variation of
baseline level. **p<0.01 vs.
Sham, ##p<0.01 vs. I/R. n=6 for
each group (for further explanation, see text)
low in I/R, markedly increased in PostC, and reduced by
the addition of SOD (PostC+SOD). Enhanced Snitrosylation of the intracellular proteins (mitochondrial
ETFAαβ and endothelial vWF) as a consequence of PostC
and the reduction of their levels by SOD addition are shown
in Fig. 7.
PostC limited the reduction in S-nitrosylated protein levels
induced by I/R in a SOD-dependent manner in late
reperfusion
At the end of reperfusion (Fig. 6c, d), the amount of
protein S-nitrosylated was reduced significantly (p<0.01)
in the I/R, PostC, and PostC+SOD with respect to the
Sham group. Although the levels of S-nitrosylated
proteins were significantly (p<0.05) lower than those
observed at the 7th min, the grade of nitrosylation observed
in the PostC group was still significantly (p<0.05) higher than
those observed in I/R and PostC+SOD groups
(p = NS, vs. each other).
PostC reversed the increase in 3-nitrotyrosine levels
induced by I/R in a SOD-independent manner in early
reperfusion only
In Fig. 8, 3-NT data are represented as percent variation
with respect to baseline level (1,653±107 nM). In I/R
group, 3-NT levels showed a significant (p<0.05) increase
at the 7th min of reperfusion with respect to corresponding
time-point in Sham (Fig. 8a). As observed by Iliodromitis et
al. [28], intramyocardial 3-NT levels were significantly
(p<0.05) decreased by PostC, being similar to Sham hearts
in our experiments, regardless of the presence of exogenous
SOD (Fig. 8a).
�228
Pflugers Arch - Eur J Physiol (2011) 462:219–233
Fig. 6 S-nitrosylated proteins in
Sham, ischemia/reperfusion (I/R),
postconditioning (PostC), and
PostC+SOD hearts. a–c Representative blots of S-nitrosylated
proteins in rat heart homogenates
at 7th and 120th min of reperfusion, respectively. To control the
specificity of the biotin switch
assay, ascorbate has been omitted
in Sham samples (−Asc). b, d
The bar graphs are means (± SE)
of band concentrations at 7th and
120th min of reperfusion,
respectively. Data are presented
as percent variation of baseline
level. *p<0.05, **p<0.01 vs.
Sham; #p<0.05 vs. I/R; §p<0.05
vs. PostC; $p<0.05 vs.
corresponding group at the 7th
min of reperfusion. NS nonsignificant. n=6 for each group
At the end of reperfusion (Fig. 8b), the levels of 3-NT in
the I/R, PostC, and PostC+SOD groups were similar to
those observed in Sham hearts.
Discussion
Here we show that postconditioning decreases protein
nitration and favors protein SNO in the early phase of
Fig. 7 S-nitrosylation of ETFAα,β and vWF in Sham, ischemia/
reperfusion (I/R), postconditioning (PostC), and PostC+SOD hearts.
The protein bands show an increase in S-nitrosylation during PostC
and a reduction during PostC+SOD at 7th min of reperfusion
reperfusion; this is associated with a significant decrease in
total SOD activity with respect to I/R. Intriguingly,
cardioprotection was abrogated by SOD addition during
PostC, supporting the idea that PostC triggering may be
involved in a redox mechanism, via an increase in O2−•
flux. This occurs in a moment in which PostC is prolonging
acidosis and favoring NO production [8, 9, 25, 29, 62, 65].
We suggest that, in acidosis, the simultaneous increase of
the flux of NO and O2−• favors protein S-nitrosylation and
reduces nitration, via a secondary reaction between ONOO−
and NO [60, 66] (see Fig. 1). Yet, since acidosis downregulates SOD, we also suggest a pivotal role for the
limited denitrosylation by SOD-downregulation in PostC
(Fig. 1) [41, 42, 56].
In the late reperfusion phase, SOD activity is increased
and catalase activity decreased in I/R, effects that are
reversed by PostC. Our results suggest that enzymes were
covalently modified in situ either by PostC maneuvers or
AB; in fact, the variation in activity started during early
reperfusion and persisted in late reperfusion and could be
observed also in tissue homogenate when pH was recovered. Hence, acidosis and reintroduction of O2 in early
reperfusion permitted ROS/RNS signaling (during PostC
�Pflugers Arch - Eur J Physiol (2011) 462:219–233
Fig. 8 Levels of 3-nitrotyrosine in Sham, ischemia/reperfusion (I/R),
postconditioning (PostC), and PostC+SOD hearts. a, b Mean (± SE)
of 3-NT levels in the ventricular tissue after 7 and 120 min of
reperfusion, respectively. Data are percent variations of baseline level.
§§p<0.01 vs. baseline level; **p<0.01 vs. Sham; #p<0.05 vs. I/R. NS
non significant. n=6 for each group
maneuvers or AB infusion) which could covalently target
enzymes, which in turn modify the redox environment (i.e.,
nitration/nitrosylation at 7th and 120th min).
Our hypotheses and analyses were focused on the PostC
triggering phase at the 7th min of reperfusion (early
reperfusion) [4, 39, 62]. At this time-point, we studied,
after I/R and PostC, both the levels and activities of CAT
and SOD and measured the levels of 3-NT and SNO
proteins. We also studied these parameters at 120-min
reperfusion (late reperfusion) to have information on the
persistence of effects and/or on variations of the compartmentalization of the redox environment in late reperfusion,
when post-ischemic pH variations should be recovered [8,
9, 17, 29, 30, 55]. The main effects observed in the early
and late reperfusion are summarized in Table 2.
Early reperfusion
Importantly, in early reperfusion, the enzyme levels are
similar in I/R and PostC. However, the activity of SOD
increases in I/R but is reduced immediately after PostC
maneuvers or acidosis. Hence, whenever we add in early
reperfusion an active exogenous SOD to the perfusate,
PostC is no longer protective. It is likely that the
implementation of this enzyme alters the scenario induced
229
by protective PostC, which per se reduces SOD activity. On
the contrary, 3 min of an active exogenous CAT does not
limit the cardioprotective effects of PostC, which, in fact,
per se tends to increase the activity of endogenous CAT
with respect to I/R. These data indicate that specific
antioxidant enzymes (SOD or CAT) can or cannot abrogate
PostC-triggering. However, large spectrum antioxidants
(NAC or MPG) abolish both preconditioning and PostC
protection in several settings [8–10, 13, 22, 38, 51, 54, 63].
Although the infused enzymes do not easily enter into the
cells, enough SOD enters, at least into endothelial cells, to
perturb the redox environment created by PostC (i.e., SOD
down-regulation), thus blocking protection. Indeed PostC
attenuates endothelial cell dysfunction by increasing eNOS
activity and NO bioavailability in neighboring cells [20,
67]. The increased availability of NO may, in turn,
contribute to SNO formation and PostC protection. It is
likely that exogenous SOD during PostC maneuvers may
also alter the necessary crosstalk between endothelium and
myocardium. The increased S-nitrosylation of endothelial
(vWF) and mitochondrial (ETFA α,β) proteins supports the
idea that the mechanism is due, at least in part, to a NO
signaling from endothelium to cardiomyocytes, which are
the richest cells in mitochondria.
A pivotal cardioprotective role for NO• from enzymatic
and non-enzymatic origin has been shown for both pre- and
postconditioning [13, 15, 25, 26, 46–50, 60, 66, 69]. In
fact, NO• is a cardiovascular protective molecule via
multiple effects, both in normoxia and particularly during
reperfusion [15, 50, 66]. Accordingly, in preconditioning, a
central role is played by protein SNO, which provides
protection preventing further cellular oxidative and nitrosative stress in reperfusion [24, 40, 56]. Yet, the high
reduction potential of NO• severely limits the formation of
peroxynitrite (ONOO−) in this context [46, 60, 66].
Actually, ONOO− has also been proposed to be cardioprotective at very low concentrations [15, 32, 65, 69]. In
particular, PostC in the presence of a peroxynitrite
decomposition catalyst (FeTPPS, 5,10,15,20-tetrakis-[4sulfonatophenyl]-porphyrinato-iron [III]) failed to reduce
infarct size in rat hearts [32]. This is an indirect observation
supporting the fact that an early increase in peroxynitriteinduced nitrosative stress is involved in the triggering
mechanism of cardioprotection by PostC. To the best of our
knowledge, no studies have shown that peroxynitrite given
at reperfusion may mimic the beneficial effects of PostC.
On the basis of our study, we suggest that, in protected
hearts, adequate levels of NO• can quench the transiently
formed ONOO− via a secondary reaction, thus forming
N2O3 and leading to protein SNO [40, 66] (Fig. 1).
According to Wang et al. [65] and Iliodromitis et al. [28],
who observed a marked decrease in 3-NT 10 min after the
beginning of reperfusion, but in contrast with Kupai et al. [32],
�230
Pflugers Arch - Eur J Physiol (2011) 462:219–233
Table 2 Variations of studied
parameters in the early (7th min)
and late stages (120th min) in I/
R and postC hearts in comparison with baseline levels
The arrows indicate significant
percent variations with respect
to baseline levels. The number
of arrows is related to the extent
of percent variation
= non-significant variation
SOD activity
CAT activity
Enzyme levels
Mn-SOD
Cu/Zn-SOD
CAT
S-nitrosylation
Tyrosine nitration
Early reperfusion (7th min)
Late reperfusion (120th min)
I/R
PostC
I/R
PostC
↑↑
=
↓↓
=
↑↑↑
↓↓
↑
=
=
=
=
↓↓
↑↑↑
=
=
=
↑↑
↑
=
↓
=
↓↓↓
=
=
=
=
↓
=
who observed an increase 5 min after the beginning of
reperfusion, we observed a decrease in 3-NT 7 min after the
beginning of reperfusion in PostC hearts. To reconcile these
apparent opposing results, we can speculate that, after an
initial formation of ONOO−, as the reaction product of O2−•
and NO•, a further increase in NO•—via enzymatic and nonenzymatic processes [54, 60, 69]—may allow a secondary
reaction between NO• and ONOO− [59, 60, 66]. This
secondary reaction may be responsible of both ONOO−
and 3-NT level lowering and SNO augmentation (Fig. 1).
The mechanism of NO-conferred prevention of
peroxynitrite-dependent damage has recently been reported
and is based on the formation of a nitrosating species in this
process [11]. We can argue that the simultaneous presence of
elevated levels of NO• and reduced activity of SOD may
favor the appropriate amount of protein SNO (Fig. 6a).
Actually, our data are in accordance with the reported
denitrosylase activity of SOD [21, 42, 56]. In fact, besides
an increased nitrosylating activity, an increased level of Snitrosylated protein in PostC hearts may be due to a
decreased rate of denitrosylation by SOD downregulation.
Indeed preconditioning also delays the denitrosylation that is
favored by the high oxygen availability [56, 57], typically of
reperfusion. Accordingly, preconditioning also delays the
normalization of tissue pH and requires ROS signaling in
early reperfusion after the index ischemia [22, 38].
Of note, persistence of acidosis is important for both nonenzymatic NO• production [60, 69] and PostC cardioprotection [8, 9, 17, 29, 34, 55]. In fact, a common mechanism by
which ischemic PostC protects the heart is by delaying the
normalization of tissue pH, and, in fact, early reperfusion
with an acidotic buffer reduces infarct size to the same extent
as PostC [8, 9, 17, 29, 34, 55] (and unpublished observations
of the authors). It is likely that low pH buffers act primarily
on the endothelial cells, supporting the importance of crosstalk between endothelium and cardiomyocytes. Full reperfusion quickly restores the intracellular pH and initiates several
adverse effects, which are collectively known as “pH
paradox”. PostC delays re-alkalinization of the heart during
early reperfusion, i.e., tissue pH remains acidic longer after
PostC compared with an abruptly reperfused heart [8, 9, 17,
29, 34, 55]. For instance, intracellular acidosis during early
reperfusion inhibits calpain activity and contributes to PostC
protection [29, 30]. Since the enzyme activities are strongly
influenced by the intracellular pH, we suggest that the acidic
intracellular environment maintained by PostC in the early
reperfusion plays an important role in the observed variation
of SOD (optimal pH 7.8) and CAT (optimal pH 7.0)
activities. In fact, the enzyme activities are similarly
influenced by AB infusion and PostC (Fig. 4). Notably,
protection by early reperfusion with an acidotic buffer is also
redox dependent [8, 9] (and unpublished observations) and
keeps a lower post-ischemic SOD activity for at least 2 h
(present study; Fig. 4). However, it is not easy to study how
the pH varies in different organelles during I/R and/or PostC.
For this reason, in a perspective of future investigations on
the role of pH, here we have opted for a study of the total
activity of SOD rather than a study of individual isoforms
confined in organelles. Nevertheless, in the early reperfusion,
there are no significant changes in the iso-enzyme levels in I/
R and PostC (Fig. 5). We suggest that the observed changes
in the activities of antioxidant enzymes contribute to PostC
triggering.
Overall, in early reperfusion, the observed changes in
enzyme activities, nitration, and nitrosylation may represent
a modification of the redox environment in a delicate
moment for the triggering of protection. This redox
mechanism includes an increase in NO• and derivative
production [9, 15, 20, 34, 49, 56] that increases the amount
of protein SNO, which is also maintained by reduced
nitrosylation breakdown by SOD downregulation (as
hypothesized; Fig. 1). The high protein S-nitrosylation
may provide “protection preventing further cellular oxidative and nitrosative stress” as well as channel opening [56].
Since the main sources of ROS are mitochondria, we can
argue that mitochondrial proteins can be among the main
targets for either SNO or 3-NT. Actually, several mitochondrial SNO proteins have been seen to be protective in
�Pflugers Arch - Eur J Physiol (2011) 462:219–233
preconditioning and reperfusion [11, 36, 56, 57]. In fact,
N2O3 has an increased stability in the hydrophobic milieu
of the mitochondria, where the high levels of reactive
cysteines would favor SNO formation [56]. Whether these
occur in PostC deserves future studies.
Late reperfusion
In late reperfusion, the activity of SOD is still reduced and
that of CAT increased by both PostC and AB, if compared
with their activities in I/R group (different covalent
modifications (?), see below). The increased activity of
CAT by PostC or AB in this phase may be important to
prevent the further reduction of H2O2 to hydroxyl radical
(OH•), which represents a dangerous step because an
increase in toxicity can occur. Yet, protection with PostC
and AB prevents the reduction of the levels of the cytosolic
Cu/Zn SOD, which are otherwise reduced after I/R. The
dichotomy on activities and levels between cytosolic and
organelle-confined enzymes [68] supports a role for
compartmentalization of the redox environment in late
reperfusion [52]. Importantly, SNO proteins are reduced by
I/R, but this reduction is limited by PostC and not by PostC
+SOD. Therefore, also in late reperfusion, SNO proteins are
still higher in PostC hearts. Whether compartmentalization
plays a role on both enzyme activity and protein nitrosylation needs to be studied further.
Preliminary data obtained with two hearts for each group
suggest that both the prolonged SOD upregulation by I/R
and the downregulation by PostC are likely due to different
covalent oxidations; in fact, a large spectrum scavenger
(MPG) prevents these modifications in activity. Preliminary
data obtained with three hearts for each group also show
that the activity of the cytoplasmatic enzyme GPx does not
change either after I/R, PostC, or AB (activity ranging
between 90% and 110% of the baseline level in all hearts).
Yet, GPx levels tend to decrease (about −20% vs. the
baseline level) in late reperfusion after I/R, but not after
PostC or AB (n=3 for each group). Also, the dichotomy of
effect (activity/level) on GPx supports a role for compartmentalization of the redox environment [52], which
deserves future studies. In fact, we argue that in different
compartments, where pH, enzyme activities, and/or levels
may be differently influenced, the redox environment may
be subtly/patchy varied. Nevertheless, overall reduced
activity of SOD by PostC is evident.
Methodological problems
We did not measure radicals but assessed SOD and CAT
activities and the levels of 3-NT and SNO proteins in vitro.
These may give information about the results of changing
ROS/RNS production and help to overcome the difficulties
231
in measuring the levels of changing radicals in situ. In fact,
the various radicals react reciprocally with an unpredictable
outcome in their levels. For example, we could measure
O2− and NO• but cannot easily predict whether ONOO− or
N2O3 formation will prevail (Fig. 1). Thus, by studying 3NT and SNO proteins, which are more stable products, we
could simultaneously have reliable indices of redox
environment and of reaction direction. However, enzyme
activities were studied at Vmax; thus, we cannot have
information on the efficacy of changed activities in situ.
Moreover, we have studied these redox effects in the
isolated hearts and could not predict whether the effects can
be replicated in vivo. Nevertheless, we have shown a redox
signaling in PostC in isolated heart [54] and this observation has been confirmed in vivo in different laboratories [8,
9, 63]. Also, these new results need to be confirmed in
vivo. Moreover, due to the variable amount of necrosis and
protein leakage from different compartments, the comprehensive interpretation of results requires future systems biology
studies, which should clarify the role of compartmentalization in enzyme/proteins, their specific nitration/nitrosylation,
and the consequent effects on their structure, activity, and/or
response to oxidative/nitrosative stress.
Finally, 3 min of CAT and/or SOD in our I/R setting is
not sufficient to limit per se infarct size and the recovery of
cardiac function, as more prolonged infusions can do in
some experimental settings [41]. Here, we specifically
tested the possibility to alter PostC-triggering with these
two different antioxidants and did not test longer infusions
which have already been largely studied.
In summary, in early reperfusion, PostC induces SOD
downregulation, which together with the persistence of
acidosis [8, 9, 17, 29, 30, 34] and the NO• augmentation
(enzymatic and non-enzymatic production [49, 60, 65,
69]) may favor nitrosylation and/or may limit protein
denitrosylation; these together with limited nitrosative
stress and preserved CAT activity accompany PostC
triggering. Intriguingly, exogenous SOD prevents PostC
triggering, whereas exogenous CAT does not interfere
with PostC protection. That is, the addition of exogenous
SOD does not allow the early reduction in SOD activity,
normally induced by PostC or AB. In late reperfusion,
SOD activity is still reduced and that of CAT increased by
PostC and AB, with respect to I/R. However, the levels of
cytoplasmatic enzymes (e.g., Cu/Zn-SOD) are reduced by
I/R and preserved by PostC, whereas the levels of
enzymes confined in the organelles (e.g., CAT, MnSOD) are not significantly affected by either I/R or PostC.
Yet, the levels of nitrosylated proteins are still higher in
PostC.
In conclusion, variations in the activity of redox
enzymes, reduced levels of 3-NT, and increased levels of
SNO proteins may contribute to cardioprotection.
�232
Acknowledgments This work was funded by: National Institutes of
Cardiovascular Research (INRC; FM, PP), Regione Piemonte, PRIN, ex60%, and Compagnia di San Paolo. We thank Prof. Donatella Gattullo for
her invaluable support and Jennifer Lee for language revision. We also
thank Prof. Marco Galloni for providing antibodies against vWF. The
authors declare that they have no conflicts of interest.
References
1. Altug S, Demiryürek AT, Cakici I, Kanzik I (1999) The beneficial
effects of peroxynitrite on ischaemia–reperfusion arrhythmias in
rat isolated hearts. Eur J Pharmacol 384:157–162
2. Baines CP, Goto M, Downey JM (1997) Oxygen radicals released
during ischemic preconditioning contribute to cardioprotection in
the rabbit myocardium. J Mol Cell Cardiol 29:207–216
3. Boengler K, Dodoni G, Rodriguez-Sinovas A, Cabestrero A,
Ruiz-Meana M, Gres P, Konietzka I, Lopez-Iglesias C,
Garcia-Dorado D, Di Lisa F, Heusch G, Schulz R (2005) Connexin43 in cardiomyocyte mitochondria and its increase by ischemic
preconditioning. Cardiovasc Res 67:234–244
4. Bopassa JC, Ferrera R, Gateau-Roesch O, Couture-Lepetit E,
Ovize M (2006) PI3-kinase regulates the mitochondrial transition
pore in controlled reperfusion and postconditioning. Cardiovasc
Res 69:178–185
5. Bradford MM (1976) A rapid and sensitive method for the
quantitation of microgram quantities of protein utilizing the
principle of protein–dye binding. Anal Biochem 7:248–254
6. Burwell LS, Nadtochiy SM, Tompkins AJ, Young S, Brookes PS
(2006) Direct evidence for S-nitrosation of mitochondrial complex
I. Biochem J 394:627–634
7. Carroll R, Gant VA, Yellon DM (2001) Mitochondrial KATP channel
opening protects a human atrial-derived cell line by a mechanism
involving free radical generation. Cardiovasc Res 51:691–700
8. Cohen MV, Yang XM, Downey JM (2007) The pH hypothesis of
postconditioning: staccato reperfusion reintroduces oxygen and
perpetuates myocardial acidosis. Circulation 115:1895–1903
9. Cohen MV, Yang XM, Downey JM (2008) Acidosis, oxygen, and
interference with mitochondrial permeability transition pore
formation in the early minutes of reperfusion are critical to
postconditioning’s success. Basic Res Cardiol 103:464–471
10. Cohen MV, Yang XM, Liu GS, Heusch G, Downey JM (2001)
Acetylcholine, bradykinin, opioids, and phenylephrine, but not
adenosine, trigger preconditioning by generating free radicals and
opening mitochondrial KATP channels. Circ Res 89:273–278
11. Daiber A, Schildknecht S, Müller J, Kamuf J, Bachschmid MM,
Ullrich V (2009) Chemical model systems for cellular nitros(yl)
ation reactions. Free Radic Biol Med 47:458–467
12. Danielisová V, Gottlieb M, Némethová M, Burda J (2008) Effects
of bradykinin postconditioning on endogenous antioxidant
enzyme activity after transient forebrain ischemia in rat. Neurochem Res 33:1057–1064
13. Downey JM, Cohen MV (2006) A really radical observation—a
comment on Penna et al. in Basic Res Cardiol. Basic Res Cardiol
101:180–189
14. Ekanayake PM, Kang H-S, De Zyosa M, Jee Y, Lee Y-H, Lee J
(2006) Molecular cloning and characterization of Mn-superoxide
dismutase from disk abalone (Haliotis discus discus). Comp
Biochem Physiol 145:318–324
15. Ferdinandy P, Schulz R (2003) Nitric oxide, superoxide, and
peroxynitrite in myocardial ischaemia–reperfusion injury and
preconditioning. Br J Pharmacol 138:532–543
16. Forbes RA, Steenbergen C, Murphy E (2001) Diazoxide induced
cardioprotection requires signaling through a redox-sensitive
mechanism. Circ Res 88:802–809
Pflugers Arch - Eur J Physiol (2011) 462:219–233
17. Fujita M, Asanuma H, Hirata A, Wakeno M, Takahama H, Sasaki
H, Kim J, Takashima S, Tsukamoto O, Minamino T, Shinozaki Y,
Tomoike H, Hori M, Kitakaze M (2007) Prolonged transient
acidosis during early reperfusion contributes to the cardioprotective effects of postconditioning. Am J Physiol Heart Circ Physiol
292:H2004–H2008
18. Gonzales DR, Fernandez IC, Ordenes PP, Treuer AV, Eller G, Boric
MP (2008) Differential role of S-nitrosylation and the NO-cGMPPKG pathway in cardiac contractility. Nitric Oxide 18:157–167
19. Gonzales DR, Treuer AV, Castellanos J, Dulce RA, Hare JM
(2010) Impaired S-nitrosylation of the ryanodine receptor caused
by xanthine oxidase activity contributes to calcium leak in heart
failure. J Biol Chem 285:28938–28945
20. Granfeldt A, Lefer DJ, Vinten-Johansen J (2009) Protective
ischemia in patients: preconditioning and postconditioning.
Cardiovasc Res 83:234–246
21. Grisham MB (1999) Effect of superoxide dismutase on the
stability of S-nitrosothiols. Arch Biochem Biophys 361:323–330
22. Hausenloy DJ, Wynne AM, Yellon DM (2007) Ischemic
preconditioning targets the reperfusion phase. Basic Res Cardiol
102:445–452
23. Heinzel FR, Luo Y, Li X, Boengler K, Buechert A, García-Dorado
D, Di Lisa F, Schulz R, Heusch G (2005) Impairment of
diazoxide-induced formation of reactive oxygen species and loss
of cardioprotection in connexin-43-deficient mice. Circ Res
97:583–586
24. Hess DT, Matsumoto A, Kim SO, Marshall HE, Stamler JS (2005)
Protein S-nitrosylation: purview and parameters. Nat Rev Mol
Cell Biol 6:150–166
25. Heusch G (2009) No risk, no…cardioprotection? A critical
perspective. Cardiovasc Res 84:173–175
26. Heusch G, Boengler K, Schulz R (2008) Cardioprotection: nitric oxide,
protein kinases, and mitochondria. Circulation 118:1915–1919
27. Heusch G, Boengler K, Schulz R (2010) Inhibition of mitochondrial permeability transition pore opening: the Holy Grail of
cardioprotection. Basic Res Cardiol 105:151–154
28. Iliodromitis EK, Andreadou I, Prokovas E, Zoga A, Farmakis D,
Fotopoulou T, Ioannidis K, Paraskevaidis IA, Kremastinos DT
(2010) Simvastatin in contrast to postconditioning reduces infarct
size in hyperlipidemic rabbits: possible role of oxidative/nitrosative stress attenuation. Basic Res Cardiol 105:193–203
29. Inserte J, Barba I, Hernando V, Abellán A, Ruiz-Meana M,
Rodríguez-Sinovas A, Garcia-Dorado D (2008) Effect of acidic
reperfusion on prolongation of intracellular acidosis and myocardial
salvage. Cardiovasc Res 77:782–790
30. Inserte J, Ruiz-Meana M, Rodríguez-Sinovas A, Barba I,
Garcia-Dorado D (2011) Contribution of delayed intracellular
pH recovery to ischemic postconditioning protection. Antioxid
Redox Signal 14:923–939
31. Jaffrey SR, Snyder SH (2001) The biotin switch method for the
detection of S-nitrosylated proteins. Sci STKE 86:PL1
32. Kupai K, Csonka C, Fekete V, Odendaal L, van Rooyen J, de
Marais W, Csont T, Ferdinandy P (2009) Cholesterol diet-induced
hyperlipidemia impairs the cardioprotective effect of postconditioning: role of peroxynitrite. Am J Physiol Heart Circ Physiol
297:H1729–H1735
33. Lacerda L, Somers S, Opie LH, Lecour S (2009) Ischaemic
postconditioning protects against reperfusion injury via the SAFE
pathway. Cardiovasc Res 84:201–208
34. Lim SY, Davidson SM, Hausenloy DJ, Yellon DM (2007)
Preconditioning and postconditioning: the essential role of the
mitochondrial permeability transition pore. Cardiovasc Res
75:530–535
35. Liochev SI, Fridovich I (2007) The effects of superoxide
dismutase on H2O2 formation. Free Radic Biol Med 42:1465–
1469
�Pflugers Arch - Eur J Physiol (2011) 462:219–233
36. Liu B, Tewari AK, Zhang L, Green-Church KB, Zweier JL, Chen
YR, He G (2009) Proteomic analysis of protein tyrosine nitration
after ischemia reperfusion injury: mitochondria as the major
target. Biochim Biophys Acta 1794:476–485
37. Liu XH, Kato H, Nakata N, Kogure K, Kato K (1993) An
immunohistochemical study of copper/zinc superoxide dismutase
and manganese superoxide dismutase in rat hippocampus after
transient cerebral ischemia. Brain Res 625:29–37
38. Liu Y, Yang XM, Iliodromitis EK, Kremastinos DT, Dost T,
Cohen MV, Downey JM (2008) Redox signaling at reperfusion is
required for protection from ischemic preconditioning but not
from a direct PKC activator. Basic Res Cardiol 103:54–59
39. Manintveld OC, Te Lintel Hekkert M, van den Bos EJ,
Suurenbroek GM, Dekkers DH, Verdouw PD, Lamers JM,
Duncker DJ (2007) Cardiac effects of postconditioning depend
critically on the duration of index ischemia. Am J Physiol Heart
Circ Physiol 292:H1551–H1560
40. Martìnez-Ruiza A, Lamas S (2004) S-nitrosylation: a potential
new paradigm in signal transduction. Cardiovasc Res 62:43–52
41. Naslund U, Haggmark S, Johansson G, Pennert K, Reiz S,
Marklund SL (1992) Effects of reperfusion and superoxide
dismutase on myocardial infarct size in a closed chest pig model.
Cardiovasc Res 26:170–178
42. Okado-Matsumoto A, Fridovich I (2007) Putative denitrosylase
activity of Cu, Zn-superoxide dismutase. Free Radic Biol Med
43:830–836
43. Oldenburg O, Cohen MV, Yellon DM, Downey JM (2002)
Mitochondrial KATP channels: role in cardioprotection. Cardiovasc
Res 55:429–437
44. Oldenburg O, Qin Q, Sharma AR, Cohen MV, Downey JM,
Benoit JN (2002) Acetylcholine leads to free radical production
dependent on KATP channels, Gi proteins, phosphatidylinositol 3kinase and tyrosine kinase. Cardiovasc Res 55:544–552
45. Pagliaro P, Mancardi D, Rastaldo R, Penna C, Gattullo D, Miranda
KM, Feelisch M, Wink DA, Kass DA, Paolocci N (2003) Nitroxyl
affords thiol-sensitive myocardial protective effects akin to early
preconditioning. Free Radic Biol Med 34:33–43
46. Pagliaro P, Moro F, Tullio F, Perrelli MG, Penna C (2011)
Cardioprotective pathways during reperfusion: focus on redox
signaling and other modalities of cell signaling. Antioxid Redox
Signal 14:833–850
47. Pagliaro P, Rastaldo R, Losano G, Gattullo D (2001) Mitochondrial
ATP-sensitive channel opener does not induce vascular preconditioning, but potentiates the effect of a preconditioning ischemia on
coronary reactive hyperemia in the anesthetized goat. Pflügers Arch
Eur J Physiol 443:166–174
48. Pain T, Yang XM, Critz SD, Yue Y, Nakano A, Liu GS, Heusch
G, Cohen MV, Downey JM (2000) Opening of mitochondrial K
(ATP) channels triggers the preconditioned state by generating
free radicals. Circ Res 87:460–466
49. Penna C, Cappello S, Mancardi D, Raimondo S, Rastaldo R, Gattullo
D, Losano G, Pagliaro P (2006) Post-conditioning reduces infarct
size in the isolated rat heart: role of coronary flow and pressure and
the nitric oxide/cGMP pathway. Basic Res Cardiol 101:168–179
50. Penna C, Mancardi D, Raimondo S, Geuna S, Pagliaro P (2008)
The paradigm of postconditioning to protect the heart. J Cell Mol
Med 12:435–458
51. Penna C, Mancardi D, Rastaldo R, Losano G, Pagliaro P (2007)
Intermittent activation of bradykinin B2 receptors and mitochondrial
KATP channels trigger cardiac postconditioning through redox
signaling. Cardiovasc Res 75:168–177
52. Penna C, Mancardi D, Rastaldo R, Pagliaro P (2009) Cardioprotection: a radical view. Free radicals in pre and postconditioning.
Biochim Biophys Acta 1787:781–793
233
53. Penna C, Perrelli MG, Raimondo S, Tullio F, Merlino A, Moro F,
Geuna S, Mancardi D, Pagliaro P (2009) Postconditioning induces
an anti-apoptotic effect and preserves mitochondrial integrity in
isolated rat hearts. Biochim Biophys Acta 1787:794–801
54. Penna C, Rastaldo R, Mancardi D, Raimondo S, Cappello S,
Gattullo D, Losano G, Pagliaro P (2006) Post-conditioning
induced cardioprotection requires signaling through a redoxsensitive mechanism, mitochondrial ATP-sensitive K+ channel
and protein kinase C activation. Basic Res Cardiol 101:180–189
55. Rodríguez-Sinovas A, Cabestrero A, García del Blanco B, Inserte
J, García A, García-Dorado D (2009) Intracoronary acid infusion
as an alternative to ischemic postconditioning in pigs. Basic Res
Cardiol 104:761–771
56. Sun J, Murphy E (2010) Protein S-nitrosylation and cardioprotection. Circ Res 106:285–296
57. Sun J, Picht E, Ginsburg KS, Bers DM, Steenbergen C, Murphy E
(2006) Hypercontractile female hearts exhibit increased Snitrosylation of the L-type Ca2+ channel alpha1 subunit and
reduced ischemia/reperfusion injury. Circ Res 98:403–411
58. Switala J, Loewen PC (2002) Diversity of properties among
catalases. Arch Biochem Biophys 401:145–154
59. Switzer CH, Flores-Santana W, Mancardi D, Donzelli S,
Basudhar D, Ridnour LA et al (2009) The emergence of
nitroxyl (HNO) as a pharmacological agent. Biochim Biophys
Acta 1787:835–840
60. Thomas DD, Ridnour LA, Isenberg JS, Flores-Santana W, Switzer
CH, Donzelli S, Hussain P, Vecoli C, Paolocci N, Ambs S, Colton
CA, Harris CC, Roberts DD, Wink DA (2008) The chemical
biology of nitric oxide: implications in cellular signaling. Free
Radic Biol Med 45:18–31
61. Tritto I, Ambrosio G (2001) Role of oxidants in the signaling
pathway of preconditioning. Antioxid Redox Signal 3:3–10
62. Tsang A, Hausenloy DJ, Mocanu MM, Yellon DM (2004)
Postconditioning: a form of “modified reperfusion” protects the
myocardium by activating the phosphatidylinositol 3-kinase-Akt
pathway. Circ Res 95:230–232
63. Tsutsumi YM, Yokoyama T, Horikawa Y, Roth DM, Patel HH
(2007) Reactive oxygen species trigger ischemic and pharmacological postconditioning: in vivo and in vitro characterization. Life
Sci 81:1223–1227
64. Ursini F, Maiorino M, Brigelius-Flohe R, Aumann KD, Roveri A,
Schomburg D, Flohé L (1995) Diversity of glutathione peroxidases.
Methods Enzymol 252:38–53
65. Wang HC, Zhang HF, Guo WY, Su H, Zhang KR, Li QX, Yan W,
Ma XL, Lopez BL, Christopher TA, Gao F (2006) Hypoxic
postconditioning enhances the survival and inhibits apoptosis of
cardiomyocytes following reoxygenation: role of peroxynitrite
formation. Apoptosis 11:1453–1460
66. Wink DA, Miranda KM, Katori T, Mancardi D, Thomas DD,
Ridnour L, Espey MG, Feelisch M, Colton CA, Fukuto JM,
Pagliaro P, Kass DA, Paolocci N (2003) Orthogonal properties of
the redox siblings nitroxyl and nitric oxide in the cardiovascular
system: a novel redox paradigm. Am J Physiol Heart Circ Physiol
285:H2264–H2276
67. Zhao ZQ, Corvera JS, Halkos ME, Kerendi F, Wang NP, Guyton
RA, Vinten-Johansen J (2003) Inhibition of myocardial injury by
ischemic postconditioning during reperfusion: comparison with
ischemic preconditioning. Am J Physiol Heart Circ Physiol 285:
H579–H588
68. Zhou Z, Kang YJ (2000) Cellular and subcellular localization of
catalase in the heart of transgenic mice. J Histochem Cytochem
48:585–594
69. Zweier JL, Talukder MA (2006) The role of oxidants and free
radicals in reperfusion injury. Cardiovasc Res 70:181–190
�
 Francesca Moro
Francesca Moro