Drug-Eluting Medical Implants
Meital Zilberman, Amir Kraitzer, Orly Grinberg, and Jonathan J. Elsner
Contents
1
Drug-Eluting Vascular Stents . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 300
1.1 Introduction: Restenosis and Drug-Eluting Stents . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 300
1.2 The First Generation of Drug-Eluting Stents (DES-I) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 301
1.3 The Second Generation of Drug-Eluting Stents (DES-II) . . . . . . . . . . . . . . . . . . . . . . . . . . . 308
1.4 Biodegradable Stents . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 311
1.5 Novel Drug-Eluting Highly Porous Stent Coatings . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 316
2 Drug-Eluting Wound Dressings . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 318
2.1 Introduction: Infection, Wound Dressings and Local Antibiotic Release . . . . . . . . . . . 318
2.2 Wound Dressings Based on Synthetic Polymers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 320
2.3 Wound Dressings Based on Natural Polymers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 321
2.4 Composite Fiber Structures Loaded with Antibacterial Drugs for Wound Healing
Applications . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 323
3 Protein-Eluting Scaffolds for Tissue Regeneration . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 330
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 332
Abstract Drug-eluting medical implants are actually active implants that induce
healing effects, in addition to their regular task of support. This effect is achieved
by controlled release of active pharmaceutical ingredients (API) into the surrounding tissue. In this chapter we focus on three types of drug-eluting devices: drugeluting vascular stents, drug-eluting wound dressings and protein-eluting scaffolds
for tissue regeneration, thus describing both internal and external implants. Each of
these drug-eluting devices also presents an approach for solving the drug release
issue. Most drug-eluting vascular stents are loaded with water-insoluble antiproliferative agents, and their diffusion from the device to the surrounding tissue is
relatively slow. In contrast, most drug-eluting wound dressings are loaded with
M. Zilberman (*)
Dept. of Biomedical Engineering, Faculty of Engineering, Tel-Aviv University, Tel-Aviv 69978,
Israel
e-mail: meitalz@eng.tau.ac.il
M. Schäfer-Korting (ed.), Drug Delivery,
Handbook of Experimental Pharmacology 197,
DOI 10.1007/978-3-642-00477-3_11, # Springer-Verlag Berlin Heidelberg 2010
299
�300
M. Zilberman et al.
highly water-soluble antibacterial agents and the issue of fast release must therefore
be addressed. Growth factor release from scaffolds for tissue regeneration offers a
new approach of incorporating high-molecular-weight bioactive agents which are
very sensitive to process conditions and preserve their activity during the preparation stage. The drug-eluting medical implants are described here in terms of matrix
formats and polymers, incorporated drugs and their release profiles from the
implants, and implant functioning. Basic elements, such as new composite core/
shell fibers and structured films, can be used to build new antibiotic-eluting devices.
As presented in this chapter, the effect of the processing parameters on the microstructure and the resulting drug release profiles, mechanical and physical properties,
and other relevant properties, must be elucidated in order to achieve the desired
properties. Newly developed implants and novel modifications of previously developed approaches have enhanced the tools available for creating clinically important
biomedical applications.
Keywords Drug eluting stents � Stent coatings � Wound dressings � Composite
structures � Scaffolds � Tissue regeneration
1 Drug-Eluting Vascular Stents
1.1
Introduction: Restenosis and Drug-Eluting Stents
The re-narrowing, or restenosis, of a treated artery is the result of a complex series
of biological events in response to the initial injury to the vessel which was caused
by balloon expansion and the presence of a permanent stent implant. Restenosis is
mainly characterized by intimal hyperplasia, i.e., an abnormal increase in the vascular smooth muscle cells (SMC) and vessel remodeling (Babapulle and Eisenberg
2002), causing a reduction in the lumen size and consequently restricting blood
flow after an intravascular procedure. The process of in-stent restenosis peaks
about the third month and reaches a plateau about six months after the procedure
(Freed et al. 1996). See Table 1 for definitions and distinct measurements of clinical
restenosis.
Bare-metal coronary stents improve clinical and angiographic outcomes by
reducing both restenosis and repetitive revascularization procedures compared to
balloon angioplasty (Fischman et al. 1994; Serruys et al. 1994). However, despite
their advantages, high in-stent restenosis (ISR) rates of 22% (Serruys et al. 1994)
and 31.6% (Fischman et al. 1994) have been reported, with even higher rates
(>50%) in cases of long and complex lesions, small vessels, multiple stenting,
and diabetes mellitus (Elezi et al. 1998; Kastrati et al. 1997).
The introduction of drug-eluting stents (DES) represents a breakthrough in the
treatment of coronary artery disease owing to their ability to reduce the incidence
�Drug-Eluting Medical Implants
301
Table 1 Clinical restenosis definitions and distinct measurements
Measurement
Definition
Target lesion
The rate of reported re-intervention procedures inside the target
revascularization (TLR)
lesion
Target vessel
The rate of re-intervention procedures inside any lesion located in
revascularization (TVR)
the same coronary vessel of treatment
Late lumen loss
The resulting luminal length reduction during follow-up
In-stent restenosis (ISR)
Angiographic measurement during follow-up as stenosis in the
treated segment >50% of the treated patients
In-segment restenosis
Angiographic measurement during follow-up as stenosis in the
treated segment including the 5 mm segment distal and proximal
to the stent edges >50% of the treated patients
Major adverse cardiac
Complications in cardiac trials such as death, Q-wave and non-Qevents (MACEs)
wave infarction, and target lesion/vessel revascularizations
Stent thrombosis
Basically defined by the presence of angiographic thrombus in a
stent during follow-up. However, it has variable definitions, such
as probable or definite stent thrombosis. Recently, a set of
definitions were developed by an academic research consortium
(ARC) which included all unexplained deaths occurring early
(<30 days), late (31–360 days), or very late (>360 days) after the
procedure
of in-stent restenosis to less than 5% (Colombo et al. 2003; Holmes et al. 2004),
and to reduce target lesion revascularization (TLR) and major adverse cardiac
events (MACE) by 70 and 50%, respectively (Stone et al. 2004), compared to
bare-metal stents. Use of DES has therefore increased in the USA from 19.7%
following their approval, to 78.2% of percutaneous procedures by the end of 2004
(Rao et al. 2006). DES were used in all lesion subsets, off-label usage, and highrisk patients where the results were less favorable (Beohar et al. 2007; Rao et al.
2006). Longer term studies in broader populations, which indicated the emergence
of troubling clinical issues, led to a surge of manuscripts that tempered enthusiasm
towards DES (Rao et al. 2008). However, recovery in the use of DES was noted in
2008, together with market approval of a new generation of DES. It should be
noted that a new surge of manuscripts supports the safety and efficacy of DES in
higher-risk patients (Turco et al. 2007). In the past five years of DES practice,
manufacturers have studied their pitfalls and have enhanced their stent technology
accordingly. We sought to learn from this rich experience, and distinguish
between the first generation of drug-eluting stents (DES-I) and the second generation (DES-II).
1.2
The First Generation of Drug-Eluting Stents (DES-I)
The first commercially available DES (in both the USA and Europe) and certainly
the most studied are CypherTM (Cordis, J&J, sirolimus-eluting stent) and TaxusTM
�302
M. Zilberman et al.
(Boston Scientific, paclitaxel-eluting stent). These stents outperformed many DES
of their generation that employed various technologies. DES consist of three
components that can radically affect their safety and efficacy: the bioactive agent,
the stent platform, and the controlled drug release mechanism. Most DES-I used a
standard bare-metal stent platform and an immunosuppressant, anticoagulant, antiinflammatory or antiproliferative agent. The drug release platforms were either
simply the drug itself, or a ceramic or polymer coating.
1.2.1
Agents
The first generation of DES used a variety of agents for the prevention of restenosis,
including anticoagulant, immunosuppressant, anti-inflammatory and antiproliferative agents. The effective and safe biological agents were those that prevented
smooth muscle cell (SMC) proliferation but preserved vascular endothelial healing.
The vascular endothelium is a key participant in the mechanism of post-procedure
thrombosis prevention (Finn et al. 2007; Hofma et al. 2006). The active pharmaceutical ingredient (API) should have a wide therapeutic window and should not
induce thrombosis or inflammation (Sousa et al. 2003a). Drug uptake into the vessel
wall usually occurs by passive diffusion and convection and is facilitated by
hydrophobic compounds that establish substantial partitioning and spatial gradients
across the tissue (Chorny et al. 2000; Creel et al. 2000). Certain drugs failed to show
antirestenotic properties, while others were effective and safe in reducing in-stent
restenosis. This may also emphasize the differences in outcomes between animal
and human models (Kutryk 2003).
Cypher is a sirolimus-eluting stent which will be addressed in the following
paragraphs in greater detail. Sirolimus, also known as rapamycin, is a macrolide
that easily crosses the cell membrane and binds to an intracellular protein
(FKBP12) which activates the protein mTOR (Gershlick 2005). This results in
an inhibition of the cell cycle in the transition from G1 to S, thus blocking cell
proliferation without inducing cell death (Moreno and Macaya 2005), allowing
minimal vascular damage compared to other antirestenosis drugs. Taxus is a
paclitaxel-eluting stent which will be addressed in the following paragraphs
in greater detail. Paclitaxel is a potent antiproliferative agent, and is known to
inhibit mitosis in dividing cells by binding to microtubules (Grube and Bullesfeld 2002), thus interfering with the pathological proliferation of SMC (Heldman
et al. 2001). Paclitaxel provided profound inhibition of neointimal thickening
depending on delivery duration and drug dosage under clinical investigation
(Grube and Bullesfeld 2002). Studies (Grube and Bullesfeld 2002; Sousa et al.
2003b) indicate the need for a controlled drug release of paclitaxel due to the
narrow therapeutic window and the high hydrophobicity of this compound. High
paclitaxel dosages may lead to an inflammatory vessel response, medial thinning, and thrombosis, due to delayed re-endothelialization (Grube and Bullesfeld
�Drug-Eluting Medical Implants
303
2002). Dose control, delivery profile, and tissue pharmacokinetics are therefore
essential.
Several other APIs selected for localized release presented less favorable outcomes. Antinomycin D is an antineoplastic drug that prevents cell division. Multilink tetra-D polymer/antinomycin D-coated stents (Guidant) presented critical
clinical safety performance which led to suspension of the use of this drug
(Woods and Marks 2004). Batimastat is a matrix metalloproteinase inhibitor that
acts to prevent cell migration and proliferation. Batimastat incorporated in
phosphorylcholine-coated DES (Biocompatibles) was studied in the BRILLIANT
trial. Early MACE rates led to suspension of the development of this stent (Salam
et al. 2006).
Anti-inflammatory and anticoagulant agents presented less favorable outcomes
than antiproliferative drugs. Dexamethasone is a glucocorticoid that modifies
protein synthesis, thereby inhibiting inflammatory responses (Liu et al. 2003) and
has a rather low effect on endothelial and SMC proliferation (Daemen and Serruys
2007). DexametTM (Abbott Vascular) is a phosphorylcholine-eluting BiodivYsio
(Biocompatibles) coronary stent that releases dexamethasone and was found safe
and effective in the STRIDE trial (Liu et al. 2003); however, DexametTM was not
found to have an antirestenosis effect (Ribichini et al. 2007).
1.2.2
Drug Release Mechanisms
Vascular injury induces cellular and sub-cellular mediators of restenosis that can be
found in the arterial wall within hours, and which may persist for days to weeks
(Kraitzer et al. 2007). Therefore, a sufficient amount of API should be released with
appropriate kinetics that are maintained for several weeks after the procedure in
order to eventually eliminate in-stent restenosis while maintaining a confluent
endothelial coverage that will suppress thrombosis. In general, DES-I offered
three drug-release mechanisms: metal stent with API bound to the metal, porous
metal, and metal-coated with durable polymers.
QuaDDS-QP2 (Quanam) was the first antiproliferative polymer-coated DES that
was developed in order to achieve controlled drug release. The stent used an
existing platform, a Quest stent covered with thin rigid sleeves equally placed
along the stent. The polymer sleeves were loaded with 7-hexanoyltaxol (QP2),
a paclitaxel derivative microtubule inhibitor (Woods and Marks 2004). The SCORE
clinical trial presented superiority over bare-metal stents in reduced in-stent
restenosis. However, marked safety issues led to termination of both the trial
and the stent program. The high surface area of the sleeves and the long duration
of the drug elution were assessed as the causes of these outcomes (Grube and
Bullesfeld 2002). We will return to DES coated with polymers in the following
paragraphs.
Paclitaxel-eluting non-polymer-coated stents were developed with the intention
of avoiding the safety concerns related to polymeric coating as inferred from trials
such as the SCORE trial. Dip-coated paclitaxel DES such as Supra G (Cook) and
�304
M. Zilberman et al.
V-Flex Plus (Cook) were found to be superior to bare-metal stents in the ASPECT
(Grube and Bullesfeld 2002) and ELUTES (Gershlick et al. 2004) trials, respectively. ACHIEVE (Guidant) demonstrated only minor improvement over baremetal stents in the DELIVER trial (Lansky et al. 2004). A direct comparison of
polymer and non-polymer-based paclitaxel-eluting stents demonstrated that the
polymer-based paclitaxel-eluting stents resulted in superior outcomes compared
to the non-polymer based paclitaxel-eluting stent (Iofina et al. 2006). Indirect
comparison indicated higher late loss rates of non-polymer-coated stents compared
to polymer-coated paclitaxel stents (Daemen and Serruys 2007; Iofina et al. 2006).
Dip-coated stents are characterized by fast washout during implantation and limited
control over the drug release profile (Halkin and Stone 2004; Iofina et al. 2006).
This release mechanism might be suitable for drugs with a wider therapeutic index
than paclitaxel. The importance of controlled release of paclitaxel was emphasized
in a clinical trial where elution <30 days was associated with higher in-stent
restenosis and MACE (Serruys et al. 2005).
Durable polymer coatings were developed and applied on the Taxus and the
Cypher DES in an attempt to achieve better control while minimizing stent/tissue
interactions. Cypher was the first approved DES, receiving the CE Mark in 2002
and FDA approval in 2003 following extensive successful clinical trials (Woods
and Marks 2004). Cypher is a tubular stainless steel Bx Velocity stent coated with a
5-mm-thick layer of non-erodible polymer (50:50 mixture of polyethylene-vinylacetate and poly-n-butyl methacrylate) containing 70–300 mg sirolimus and an
additional topcoat cover over the drug polymer matrix to serve as a diffusion barrier
(Duda et al. 2003; Venkatraman and Boey 2007). The API is released slowly over
4–6 weeks, where approximately 80% is released after four weeks, and 100% after
6 weeks (Woods and Marks 2004). Cypher drastically reduced the in-stent restenosis rate compared to bare-metal stents as confirmed in: RAVEL (Morice et al.
2002), SIRIUS (Moses et al. 2003), E-SIRIUS (Schofer et al. 2003), SES-SMART
(Ardissino et al. 2004) in high-risk populations, and C-SIRIUS (Schampaert et al.
2004) studies (Fig. 1).
TaxusTM was the second DES to be commercially approved following extensive
successful clinical trials (Heldman et al. 2001). In its first version, Taxus was based
on a 316L stainless steel NIRx stent coated with a poly(lactide-co-e-carpolactone)
copolymer loaded with paclitaxel (Tanabe et al. 2003). The release profile was
characterized by an initial burst release over the first 48 h followed by very slow
release with ~2 mg being released within 15 days (Venkatraman and Boey 2007),
and 92.5% of the drug remain in the matrix for a long period (Serruys et al. 2005).
The NIRx platform was replaced with ExpressTM tandem architecture between the
Taxus III and IV trials. This platform combines scaffolding with flexibility and
deliverability which improve drug release homogeneity, especially in tortuous
vessels as opposed to the closed cell structure (Halkin and Stone 2004). Taxus
stents have demonstrated a reduced rate of restenosis and revascularization events
in Taxus I (Halkin and Stone 2004), II (Colombo et al. 2003), IV (Halkin and Stone
2004), VI (Dawkins et al. 2005) (Fig. 2) and were not associated with increased risk
of stent thrombosis, at least when dual antiplatelet treatment with aspirin and
�Drug-Eluting Medical Implants
305
Fig. 1 Selected Cypher pivotal studies: (a) angiographic in-segment restenosis, (b) target lesion
revascularization (BMS, bare metal stent; SES, sirolimus eluting stent)
clopidogrel was administered (Halkin and Stone 2004; Moreno and Macaya 2005;
Venkatraman and Boey 2007).
1.2.3
Real World
The clinical superiority of Cypher and Taxus over bare-metal stents has continued
after four (Aoki et al. 2005a) and five (Corporation 2007; Morice et al. 2007) years
of the pivotal randomized trials. However, continued neointimal formation over
time is a phenomenon observed with DES, as opposed to bare-metal stents in which
neointimal formation peaks at about six months and then regresses. Nonetheless, as
more and more data emerge for complex lesions, longer-term follow-ups and a
broader real world range of patients (Rogers 2004), DES outcomes appear to be less
�306
M. Zilberman et al.
Fig. 2 Selected Taxus pivotal studies: (a) angiographic in-stent restenosis (ISR), (b) target lesion
revascularization (BMS, bare metal stent; PES, paclitaxel eluting stent)
favorable (Venkatraman and Boey 2007). Between 50% (Beohar et al. 2007) and
75% (Planer et al. 2008) of all DES use occurs in off-label or untested settings
(Beohar et al. 2007). Patients who receive DES for off-label and untested indications tend to present more severe clinical profiles (Beohar et al. 2007). A 3-year
follow-up conducted by the Israeli arm of the e-Cypher registry showed that 87% of
stent thromboses and 85% of all MACEs occurred in off-label indications (Planer
et al. 2008). Figure 3 presents the increased rates of TLR, in-stent restenosis of such
“real world” registries: world e-Cypher (Urban et al. 2006), Israeli arm e-Cypher
(Planer et al. 2008), RESEARCH (Daemen et al. 2006), REALITY (Morice et al.
2006), REWARDS (Roy et al. 2008). No major differences were found in the
clinical trials or angiographic outcomes that presented equivalent safety and efficacy, when comparing Taxus and Cypher in the real world (Morice et al. 2006;
Roy et al. 2008).
�Drug-Eluting Medical Implants
307
Fig. 3 Real world Cypher and Taxus studies, target lesion revascularization results (BMS, bare
metal stent; PES, paclitaxel eluting stent; SES, sirolimus eluting stent)
Cypher and Taxus were associated with an increased rate of late stent thrombosis
(LST) (Lagerqvist et al. 2007) and hypersensitivity reactions on a smaller scale
(Virmani et al. 2004). DES implantation may increase death and myocardial rates at
6–18 months compared with bare-metal stents, particularly after discontinuation of
anti-platelet therapy (Joner et al. 2006). Stent thrombosis is a low frequency event,
with serious life-threatening consequences. A pooled 4-year data analysis indicates
that out of patients who had definite or probable stent thrombosis 30.9%s died and
83.8% underwent myocardial infraction (Mauri et al. 2007). The difficulty of
uniquely defining thrombosis rates has posed an analysis bias. A set of definitions
was recently developed by an academic research consortium (ARC) to serve as
standard criteria for stent thrombosis in cases which were not taken into account in
previous definitions (Planer et al. 2008). The incidence of definite or probable stent
thrombosis according to any ARC thrombosis criteria was found to be three times
higher than the incidence obtained by the previous definitions in a 4-year pooled
data from RAVEL, SIRIUS, C, E-SIRIUS, Taxus I, II, IV, V (Mauri et al. 2007).
Late stent thrombosis is mostly predicted by partial, heterogenic endothelial coverage characterized by persistent fibrin deposition and delayed re-endothelialization
(Finn et al. 2007; Joner et al. 2006). The mechanisms by which DES induce nonuniform incomplete healing are not fully understood; however, the main suspects
are lesion type, the antiproliferative drug itself, and its dose and distribution (Finn
et al. 2007). Hofma et al. (2006) found that the sirolimus-eluting stent had an
adverse effect on local endothelium-dependent vasomotor responses at six months.
Late stent thrombosis may also result as a consequence of hypersensitive reactions
caused by the durable polymer coating (Virmani et al. 2004).
A summary of the cumulative experience with DES-I indicates a complex
interplay between drug selection and drug-release mechanism which determines
�308
M. Zilberman et al.
the safety and optimizes the local therapeutic benefit (Duda et al. 2003; Sousa et al.
2003a). The DES era also poses new challenges as a result of the growing complexity of lesions that are treated percutaneously, which require better deliverability
and higher flexibility (Daemen and Serruys 2007). DES-I offered limited control
over the drug release period, drug content, and homogenous release in cases of
complex anatomical circumstances (Rogers 2004; Wang et al. 2006).
1.3
The Second Generation of Drug-Eluting Stents (DES-II)
DES-II were designed in light of safety and efficacy issues of DES-I, offering an
enhanced platform, release matrix, and more targeted antiproliferative agents. The
enhanced platform aims to increase clinical outcomes in high-risk populations and
challenging anatomies. The offered release matrices improve the polymer/tissue reaction as well as drug release kinetics. Cypher and Taxus have set a standard for the
development of DES-II and their clinical outcomes are frequently used for comparison.
1.3.1
Platforms
DES-II platforms are designed for better deliverability, higher flexibility (Daemen
and Serruys 2007), as well as drug release homogeneity and a low strut profile.
Taxus Liberté (Turco et al. 2007), and Cypher SelectTM (Gao et al. 2008), the
advanced versions of Taxus and Cypher, were designed for this purpose. Their
platforms consist of a closed-cell, continuous structure, in order to provide both
uniform scaffolding and homogenous drug distribution within the carrier. The
safety and efficacy of Cypher Select and Taxus Liberté were found comparable to
their predecessor in the CCSR (Gao et al. 2008) and ATLAS (Turco et al. 2007)
studies, respectively. Most DES-II platforms hold thin flexible struts in order to
reduce stent/tissue interactions and allow endothelial cells to bridge across the
struts (Lewis et al. 2002). DES-II shifted from the 316L stainless steel to a
chromium stent platform, since cobalt alloy is 45% stronger than stainless steel,
thus allowing thinner struts while maintaining radial strength (Popma 2007).
1.3.2
New Agents
Six Limus family agnets: sirolimus, everolimus, biolimus (A9), zotarolimus (ABT578), tacrolimus, and pimecrolimus are used extensively in DES-II. Sirolimus,
everolimus, biolimus, and zotarolimus bind to the intracellular binding protein
FKBP12, which subsequently binds to the mammalian target of rapamycin (mTOR)
and blocks the cell cycle in the G1 to S phase (Daemen and Serruys 2007).
Tacrolimus and pimecrolimus bind to FKBP506 but do not block the activation
of mTOR. However, they result in inhibition of T-cell activation and lower smooth
�Drug-Eluting Medical Implants
309
muscle cell selectivity (Daemen and Serruys 2007). Xience V (Abbott Vascular) is
an everolimus-eluting stent embedded in a durable fluoropolymer coating a thinstrut cobalt chromium platform (Stone et al. 2008). Everolimus proved rapid
endothelialization with this stent compared to the sirolimus-eluting stent and the
paclitaxel-eluting stent in rabbits (Joner et al. 2008). The everolimus-eluting stent
was superior in performance compared to bare-metal stents in the SPIRIT I (Serruys
2005) trial, and non-inferior to the paclitaxel-eluting stent in terms of safety and
effectiveness in the SPIRIT II (Serruys 2006) and III trials (Stone et al. 2008).
Endeavor (Medtronic) is a zotarolimus-eluting stent on a Driver thin-strut cobalt
chromium platform with a phosphorylcholine coating (Fajadet et al. 2006). The
zotarolimus-eluting stent proved sustained clinical effectiveness up to four years in
the ENDEAVOR I (Meredith et al. 2007a) trial, and superiority over bare-metal
stents in the ENDEAVOR II (Fajadet et al. 2006) trial, but demonstrated lack of
non-inferiority to the sirolimus-eluting stent in the ENDEAVOR III trial (Miyazawa
et al. 2008). This may be explained by the fast drug release rate, since the zotarolimus is released within 2 days (Daemen and Serruys 2007).
New agents, dual DES release, and a new pro-healing approach, are notable in
DES-II. Sahajanand Medical Technologies designed a dual-layer heparin sirolimuseluting stent, which combines the antiproliferative action of sirolimus with the
excellent biocompatibility and hemocompatibility of the heparin coating (Daemen
and Serruys 2007). Pimecrolimus, primarily an anti-inflammatory agent, was
loaded on a Conor stent and tested in a porcine model in two phases: pimecrolimus alone and combined with paclitaxel (Berg et al. 2007). The stent inhibited
neointimal proliferation compared to bare-metal stents and proved the safety and
efficacy of the dual concept. Genistein is a potent isoflavone, which possesses
dose-dependent antiplatelet and antiproliferative properties (Daemen and Serruys
2007). A dual sirolimus genistein-eluting stent is currently under investigation. Furthermore, a new pro-healing endothelial progenitor cell capture stent
consists of antibodies attached to a stainless steel stent which specifically target endothelial progenitor cells in the vascular circulation. The HEALING-FIM
(Aoki et al. 2005b) trial demonstrated that the endothelial progenitor cell capture stent is safe and feasible. The HEALING-II trial reported 6-month in-stent
restenosis rates of 17.2% with an associated in-stent late luminal loss of
0.78 � 0.39 mm that was reduced to 0.59 � 0.06 mm at 18 months (Daemen
and Serruys 2007).
1.3.3
New Drug-Release Mechanisms
The DES-II exhibited improved drug release matrix designs such as durable
biodegradable polymers and layered release matrices for controlled release. EndeavorTM Resolute (Medtronic) is a new zotarolimus-eluting stent based on a novel
BioLinxTM copolymer optimal for extended drug release (Meredith et al. 2007b).
BioLinx is a unique blend of three different polymers: a hydrophobic polymer
for delayed drug release, a lipophilic polymer for enhanced biocompatibility, and
�310
M. Zilberman et al.
a hydrophilic polymer for release burst. The Resolute stent elutes 85% of its
zotarolimus content during the first 60 days and the remainder in 180 days in vivo
(Meredith et al. 2007b). ZoMaxx (Abbott Laboratories) is another example of
a smart matrix which elutes zotarolimus via a tri-layer coating consisting of a
phosphorylcholine basecoat and a topcoat wrapped around a zotarolimus layer for
slow elution (Abizaid et al. 2007). ZoMaxx also uses a novel Tri-Maxx stent
platform which has a thin 3-layer tantalum sandwiched between two layers of
stainless steel for enhanced fluoroscopic radiopacity. However, ZoMaxx was associated with a significantly high late loss and in-stent restenosis compared to Taxus
in the ZoMaxx-I trial, which led Abbott to discontinue its program (Daemen and
Serruys 2007).
Biodegradable polymer-coated metal stents were first introduced in DES-II in an
attempt to overcome the late risk associated with durable polymers. Guidant’s
everolimus program consisted of the Biosensors Champion stent with a biodegradable polylactic acid coated S-stent with an elution profile of 70% drug release in
30 days (Grube et al. 2004), and 85% in 90 days (Tsuchiya et al. 2006). The
FUTURE I (Grube et al. 2004), and II (Tsuchiya et al. 2006) trials reported
superiority over bare-metal stents (Salam et al. 2006). However, the program
was eventually discontinued by Guidant (Peterson 2004). The biolimus-eluting
BioMatrix stent (Biosensors International) is coated with a poly-lactic acid bioabsorbable polymer that gradually releases the drug over 6–9 months. BioMatrix was
tested in the STEALTH-1 (Daemen and Serruys 2007) trial, and exhibited superiority over bare-metal stents, non-inferiority with the paclitaxel-eluting stent
(Chevalier et al. 2007) in the Nobori-I study, safety and efficacy in the NOBORI
CORE trial (Ostojik et al. 2008) and non-inferiority with the sirolimus-eluting stent
in the LEADERS trial in a 9-month follow-up (Windecker et al. 2008). Paclitaxeleluting InfinniumTM DES (Sahajanand Medical Technologies) is a slotted-tube
stainless steel stent with lower strut thickness coated with three layers of biodegradable polymer: poly(DL-lactic acid-co-glycolic acid) (PDLGA) 50/50, PDLGAco-caprolactone (PDLGPCL) 75/25, and polyvinyl pyrrolidone (Vranckx et al.
2006). Paclitaxel is released in three release regimes: fast release during the first
five days, followed by medium release in the next six days, and slow release until
day 48. SIMPLE-I and II trials proved that InfinniumTM was safe and effective
(Daemen and Serruys 2007).
A classic approach offering an improved control over drug release was suggested by Conor Medsystems. Both their Conor Medstent (316L stainless steel
based) (Serruys et al. 2005), and Conor Co-star (cobalt chromium based) (Krucoff
et al. 2008) allow programmable and controlled paclitaxel release using a biodegradable polymer layer deposited in laser-cut holes embedded in the stent platform.
Paclitaxel distribution and kinetics is obtained by using a poly-lactic-co-glycolic
acid (PLGA) copolymer deposited within the different layers (Krucoff et al. 2008).
The PISCES study proved that the Conor Medstent was safe and that the duration of
release had a greater impact on the inhibition of the in-stent neointimal hyperplasia
than the dose (Serruys et al. 2005). COSTAR I evaluated three dose-release
formulations and reported that the low-dose slow-release formulation (10 mg
�Drug-Eluting Medical Implants
311
Fig. 4 DES-II selected clinical target vessel revascularization outcomes (EES everolimus-eluting
stent, ZES – zotarolimus-eluting stent, BES – biolimus-eluting stent, COSTAR paclitaxel-eluting
stent, SES – sirolimus-eluting stent (DES-I), PES – paclitaxel-eluting stent (DES-I), BMS – baremetal stent)
paclitaxel release over 30 days) achieved the best clinical and angiographic outcomes (Kau 2007). The EUROSTAR (Dawkins et al. 2007) trial confirmed Co-star
safety and efficacy in the low-dose slow-release formulation compared to the highdose slow-release formulation. Nonetheless, the COSTAR II study could not
conclude that the CoStar DES is non-inferior in clinical and angiographic performance compared to the paclitaxel-eluting stent (Krucoff et al. 2008), leading to
discontinuation of the program (Medsystems 2007).
The promising Xtent (Biosensors International) biolimus-eluting cobalt
chromium, polylactic acid coated stent combines all of the above-stated DES-II
characteristics. It is tailored for long/multiple lesions and multivessel disease and
allows in situ customization of stent length. The CUSTOM-I evaluation study
reports 12-month safety and efficacy with Xtent (Grube 2008). The CUSTOM-II
trial presented favorable 1-year follow-up results in high-risk multi-vessel-treated
patients demonstrating safe in situ customization (Stella et al. 2008).
Figure 4 presents clinical outcomes of selected second-generation stents and
Fig. 5 illustrates selected drug-eluting matrix concepts of current DES. Table 2
summarizes selected metal drug-eluting stent designs.
1.4
Biodegradable Stents
Biodegradable stents are now in an advanced stage of research and development,
and are considered by many as the next generation of DES. Metal stents have
thrombogenic properties (Tepe et al. 2002), and may therefore cause permanent
physical irritation, with the risk of long-term endothelial dysfunction or
�312
M. Zilberman et al.
Fig. 5 Selected drug-eluting matrix illustrations (source: Kutryk 2003). (1) Boston Scientific;
polystyrene-polyisobutylene polystyrene copolymer intermediate layer. (2) Cook; non-polymerized
albumin coating. (3) Guidant; ethylene-vinyl acetate intermediate layer. (4) Conor-Medsystems:
PDLGA copolymer intermediate layer. (5) Cordis: ethylene-vinyl acetate and poly(n-butyl methacrylate) polymer intermediate layers. (6) Abbot/Jomed: ethylene-vinyl acetate intermediate layer.
(7) Sorin: no coating. (8) Jomed: nanoporous ceramic. (9) Igaki–Tamai: poly(L-lactic acid) stent.
(10) BiodivYsio Matrix LO (for drugs with a molecular weight of <1200 Da); phosphorylcholine
coating. (11) BiodivYsio Matrix HI (for drugs with a molecular weight of <1200 Da); phosphorylcholine coating
inflammation (Farb et al. 1999). Permanent stents also pose a barrier for possible
future bypass surgery (Waksman 2006) and noninvasive imaging. These disadvantages may be avoided by using a temporary scaffold, considering that the need for a
permanent prosthesis decreases dramatically six months post-implantation (Tamai
et al. 2000). Completely biodegradable stents may eliminate early and late complications of bare-metal stents and DES implantation by degrading into non-toxic substances after maintaining luminal integrity only during the period of high risk
restenosis in the first 9–12 months (Commandeur et al. 2006). Finally, biodegradable
stents have a higher capacity for drug incorporation, and allow more complex
release kinetics by altering the biodegradation profile of the polymer (Commandeur
et al. 2006). The main challenge in designing a biodegradable DES is overcoming
the trade-off between mechanical properties and drug loading, since the radial
compression strength of the stent is dramatically affected by the drug load.
A second challenge is to effectively incorporate the drug during fabrication without
damaging the molecules.
The early bioresorbable stents (1980s) were designed as simple scaffolds and did
not contain drugs. The bioresorbable materials used were PDLGA, polycaprolactone (PCL), poly(hydroxybutyrate hydroxyvalerate), and polyorthoester. All were
associated with a significant inflammatory response and neointimal proliferation
(Saito et al. 2002; Stack et al. 1988; Zidar et al. 1999). Tamai et al. (1999), Tamai
et al. (2000) were the first to study a bioresorbable stent in clinical trials. The Igaki–
Tamai stent is a poly L-lactic acid (PLLA) zig-zag helical coil design, and presented
�Endeavor Resolute/Medtronic
PROMUSTM/Boston Scientific
Cypher SelectTM Plus/Cordis (J&J)
Infinnium/Sahajanand Medical
Technologies
CoStarTM/Conor Medsystems
BioMatrix1/Biosensors
International
NOBORITM TERUMO
ACHIEVETM/Cook-Guidant
V Flex Plus PTXTM/ Cook
JANUS/Sorin Biomedica
GenousTM/OrbusNeich
DexametTM/Abbott vascular
XTENT1/Biosensors International
Supralimus-CoreTM/Sahajanand
Medical Technology
Platform
BX Velocity
Matrix type
Durable polymer
Express 2
Durable polymer
Driver1
Phosphorylcholine
Multi-Link
Durable polymer
Vision 1
BioLinxTM
Zotarolimus
Cobalt chromium
Driver1
A private-label version of Abbott’s XIENCETM V Everolimus Eluting Coronary Stent System
Sirolimus
316L Stainless steel
Undisclosed
Durable hydrophilic coating
(Rapamycin)
Biodegradeable polymers
Paclitaxel
316L Stainless steel
Millennium
Matrix1
Paclitaxel
Cobalt chromium
CoStarTM
Biodegradable PDLGA layers
Biolimus1
316L Stainless steel
S-StentTM
Biodegradable PLA
NOBORITM is marketed with licensing agreement with biosensor under its technology.
Paclitaxel
316L Stainless steel
MULTI LINK Polymer-free
PENTATM
Paclitaxel
316L Stainless steel
V-Flex Plus
Polymer-free
Tacrolimus
316L Stainless steel
Carbostent
Nanoporous ceramic coating
Endothelial
316L Stainless steel
R-Stent
Polysaccharide, covalently
progenitor cell
coupled to stent surface
capture
Dexamethasone
316L Stainless steel
Biodiv YsioTM Phosphorylcholine
1
Biolimus
Cobalt chromium
Custom NX1
Biodegradable PLA
Sirolimus
316L Stainless steel
Millennium
Biodegradable Polymers
Matrix1
Status
FDA, CE Mark
FDA, CE Mark
FDA, CE Mark
FDA, CE Mark
CE Mark
FDA
CE Mark
Drug-Eluting Medical Implants
Table 2 Selected Coated Metal Drug Eluting Stent (DES-I and DES-II)
DES/manufacturer
Drug
Stent material
316L Stainless steel
Cypher/Cordis (J&J)
Sirolimus
(Rapamycin)
Paclitaxel
316L Stainless steel
Taxus LibertéTM/Boston Scientific
Zotarolimus
Cobalt chromium
Endeavor1/Medtronic
Everolimus
Cobalt chromium
XIENCETM V/Abbott vascular
CE Mark
CE Mark
CE Mark
CE Mark
CE Mark
CE] Mark
CE Mark
CE Mark
approved in
Taiwan
CE Mark
Trial
Trial
(continued)
313
�Drug
Zotarolimus
Stent material
Stainless steel/
tantalum/ stainless
steel
316L Stainless steel
Platform
Tri-Max
Matrix type
Phosphorylcholine
Status
Suspended
BiodivYsioTM
Phosphorylcholine
Suspended
QueST
Batimastet BiodivYsio
(Biocompatibles and British
Biotech)
QuaDDS-QP2/Quanam Medical
and Boston Scientific
Antinomycin D stent/ Guidant
Batimastet
7-hexanoyltaxol
(QP2)
Antinomycin D
316L Stainless steel
Jomed Flexmaster/Jomed
Tacrolimus
316L Stainless steel
316L Stainless steel
Rigid polymer/drug sleeve
cover
MULTILINK
Durable polymer (Ethylene
tetra-D stent
vinyl acetate)
Jomed
Nanoporous ceramic layer
Flexmaster
314
Table 2 (continued)
DES/manufacturer
Zomaxx/Abbott Labratories
Suspended
Suspended
Suspended
M. Zilberman et al.
�Drug-Eluting Medical Implants
315
intimal hyperplasia in rates comparable to bare-metal stents in six months, and 18%
TVR in a 4-year follow-up (Waksman 2006). Lincoff et al. (1997) demonstrated
that high-molecular-weight PLLA performance was more favorable than lowmolecular-weight PLLA in terms of an inflammatory reaction. Biodegradation of
PLLA is achieved by hydrolytically unstable ester linkages in the backbone of
the polymer, which result in chain scission into oligomers and eventually erosion
with an overall degradation time which depends on the initial molecular weight
(Commandeur et al. 2006). The oligomers are then broken down into lactic acid,
and are completely metabolized via the Krebs cycle (Ormiston et al. 2008)
Early biodegradable drug-eluting stent designs were based on fiber or film
structures. Yamawaki et al. (1998) incorporated Tranilast (ST638) or ST494 (an
inactive metabolite of ST638) agents into the Igaki–Tamai stent. The stent
presented significantly less neointimal formation and geometric remodeling
with ST638 than with ST494. Uurto et al. (2005) evaluated a monofilamentbased stent made of a polymer consisting of 96% L-lactic acid and 4% D-lactic
acid coated with a 50/50 ratio of two bioactive agents: dexamethasone and
simvastatin. The stent presented acceptable results in a porcine model. Vogt
et al. (2004) reported paclitaxel-loaded poly(D,L-lactic acid) (PDLLA) doublehelical stent exhibiting sufficient mechanical stability with a very slow release
pattern of paclitaxel in a porcine model. Their 2-month evaluation demonstrated
effective proliferation inhibition, but also local inflammatory effects due to
polylactide resorption. Alexis et al. (2004) incorporated paclitaxel and rapamycin
into PDLLA and PDLGA non-expandable helical stents prepared from film strips
exhibiting a homogenous, burst-free drug release. Ye et al. (1998) demonstrated
the successful transfer and expression of a nuclear-localizing b-Gal reporter gene
in cells in the arterial wall of rabbits after the implantation of biodegradable
stents made of PLLA/PCL films. These stents were made of a porous tubular
structure impregnated with a recombinant adenovirus carrying that gene and demonstrated an exciting possibility for restenosis prevention. The multiple lobe
PLLA fiber-based stent (Nguyen et al. 2004) was coated with drug-loaded microspheres in order to combine good mechanical properties with the desired drug
release profile (Zilberman et al. 2004). These microsphere reservoirs, which were
prepared by the double-emulsion technique, can be loaded with biologically
active aqueous or non-aqueous molecules. Since mild materials and processing
steps are used, these microspheres can be loaded with all drugs, proteins and gene
transfer vectors.
Current drug-eluting biodegradable stents in the stage of clinical trials are
described below. The everolimus bioasbsorbable stent (BVS, Abbott Vascular)
consists of a bioabsorbable PLLA base coated with a more rapidly degrading
PDLLA coating and releases 80% of its drug in 28 days and is kept at 20� C in
order to extend its shelf-life (Ormiston et al. 2008). The first in-men ABSORB trial
(n ¼ 30) demonstrated high procedural success, with a collapse pressure similar to
a stainless steel stent, with 0% TLR, 0% stent thrombosis, one patient had a
myocardial infraction, and late loss of 0.44 � 0.35 mm in one year (Ormiston
et al. 2008). The REVA bioresorbable stent uses a tyrosine-derived polycarbonate
�316
M. Zilberman et al.
platform and utilizes a slide and lock mechanism rather than deforming during
usage. REVA Medical announced the enrollment of first-in-man RESORB study
for paclitaxel-coated REVA (REVA Medical 2007) backed by promising animal
trials (Waksman 2006). An interesting new approach was presented by Bioabsorbable Therapeutics, Inc. (BTI): a sirolimus-eluting biodegradable stent composed of
salicylic acid (active ingredient in aspirin) chemically incorporated into polyanhydride layers (Buchbinder 2007).
1.5
Novel Drug-Eluting Highly Porous Stent Coatings
As mentioned above, one of the issues that should be addressed in the field of DES
is the very slow release rate of highly hydrophobic antiproliferative drugs, such as
paclitaxel. We developed and studied paclitaxel-eluting porous coatings (shell) for
both metal and polymeric (biodegradable) stents in order to address this issue
(Kraitzer and Zilberman 2007). The coating preparation is based on the freezedrying of inverted emulsions technique. The investigation of these new coatings
focused on the effects of the emulsion’s composition (formulation) and process
kinetics on the long-term drug release from fibers, in light of the shell’s morphology
and degradation profile. The paclitaxel release exhibited three phases, which
corresponded to the degradation profile of the host PDLGA. We found that the
effect of the emulsion formulation on the release profile is more significant than
the effect of the process kinetics. The copolymer composition had the most dominant effect on the drug release profile from the composite fibers. An increase in the
glycolic acid content of the copolymer (or decrease in lactic acid content) resulted
in a tremendous increase in the release rate during the second phase, which was
attributed mainly to the increased degradation rate and decreased drug attachment
to the host polymer (Fig. 6a). The paclitaxel release profile was improved and we
concluded that emulsions with a less hydrophobic nature are favorable for effective
controlled release of the hydrophobic paclitaxel from the porous shell.
Farnesylthiosalicylate (FTS, Salirasib) is a rather specific non-toxic new agent
which was recently developed at the Tel-Aviv University, Israel (Kloog and Cox
2004). It acts as a Ras antagonist (George et al. 2004; Kloog and Cox 2004) and has
a mild hydrophobic nature. In its active form (GTP-bound) Ras promotes enhanced
cell proliferation, tumor cell resistance to drug-induced cell death, cell migration
and invasion. Ras is therefore considered an important target for cancer therapy as
well as for therapy of other proliferation diseases, including restenosis. The apparent selectivity of FTS towards active (GTP-bound) Ras and absence of toxic or
adverse side-effects was proven in animal models (George et al. 2004) and in
human trials (phase I performed at MD Anderson Cancer Center). FTS was found
to be a potent inhibitor of intimal thickening in the rat carotid artery injury model
which serves as a model for restenosis where it does not interfere with endothelial
proliferation (George et al. 2004). The incorporation of the new drug FTS in a stent
�Drug-Eluting Medical Implants
317
Fig. 6 The effect of copolymer composition on the cumulative drug release profile from core/shell
fiber structures (~ – PDLGA 50/50, ● – PDLGA 75/25): (a) paclitaxel release, (b) FTS release.
Source (a) Kraitzer et al. 2008, (b) Kraitzer et al. 2009
coating may overcome the incomplete healing and lack of endothelial coverage
associated with current DES.
Our novel porous coatings were loaded with the new agent FTS (Kraitzer et al.
2009). Our results show that the most important parameter affecting release in this
system was again the copolymer composition. An increase in the glycolic acid
content of the PDLGA copolymer enhanced the burst effect and release rate during
the first two weeks, mainly due to higher water uptake and swelling but also due to a
higher degradation rate of the host polymer (Fig. 6b). The FTS release from our
highly porous coatings is faster, more adjustable and totally different from that of
�318
M. Zilberman et al.
paclitaxel. Paclitaxel is more hydrophobic than FTS and creates more specific
interactions with the host polyesters. Therefore, paclitaxel’s diffusion through the
host polymer is much slower and all changes in formulation parameters affect its
release profile mainly after 10 weeks of degradation. In paclitaxel-eluting systems
the emulsion formulation influences diffusion by producing binding regions for the
drug as more hydrophobic materials are introduced into the emulsion, thus delaying
the drug molecules. The release profile of FTS from our composite fibers is
therefore more suitable for the stent application. Furthermore, since FTS is less
toxic, some burst release can be tolerated and may be beneficial.
In summary, in this section we described the two vascular drug-eluting metal
stent generations, DES-I and DES-II, in terms of stent platform, incorporated APIs,
drug-release profile and stent functioning. We also discussed biodegradable drugeluting stents and our novel drug-eluting porous coatings, which can be applied on
both metal and biodegradable stents. It can be concluded that the field of drugeluting vascular stents has progressed significantly over the past several years. The
combination of the above-described new coatings and new APIs that have recently
been developed will further improve this life-saving device.
2 Drug-Eluting Wound Dressings
2.1
Introduction: Infection, Wound Dressings and Local
Antibiotic Release
The skin is regarded as the largest organ of the body and has many different
functions. Wounds with tissue loss include burn wounds, wounds caused as a result
of trauma, diabetic ulcers and pressure sores. The regeneration of damaged skin
includes complex tissue interactions between cells, extracellular matrix (ECM)
molecules and soluble mediators in a manner that results in skin reconstruction.
The moist, warm, and nutritious environment provided by wounds, together with
diminished immune functioning secondary to inadequate wound perfusion, may
allow build-up of physical factors such as devitalized, ischemic, hypoxic, or
necrotic tissue and foreign material, all of which provide an ideal environment
for bacterial growth (Jones et al. 2004). In burns, infection is the major complication after the initial period of shock. It is currently estimated that about 75% of the
mortality following burn injuries is related to infections rather than to osmotic
shock and hypovolemia (Revathi et al. 1998).
Infection is defined as a homeostatic imbalance between the host tissue and the
presence of microorganisms at concentrations that exceeds 105 organisms per gram
of tissue or the presence of beta-hemolytic streptococci (Sussman and Bates-Jensen
2001; Xu et al. 2004). The main goal of treating the various types of wound
infections should be to reduce the bacterial load in the wound to a level at which
wound healing processes can take place. Otherwise, the formation of an infection
�Drug-Eluting Medical Implants
319
can seriously limit the wound healing process, can interfere with wound closure and
may even lead to bacteremia, sepsis and multi-system failure. Evidence of bacterial
resistance is on the rise, and complications associated with infections are therefore
expected to increase in the general population.
Various wound dressings aim to restore the milieu required for skin regeneration
and to protect the wound from environmental threats and penetration of bacteria.
Although traditional gauze dressings offer some protection against bacteria, this
protection is lost when the outer surface of the dressing becomes moistened by
wound exudates or external fluids. Furthermore, traditional gauze dressings exhibit
low restriction of moisture evaporation which may lead to dehydration of the
wound bed. This may lead to adherence of the dressing, particularly as wound
fluid production diminishes, causing pain and discomfort to the patient during
removal.
Most modern dressings are designed according to the well-accepted bilayer
structural concept: an upper dense “skin” layer to prevent bacterial penetration
and a lower spongy layer designed to adsorb wound exudates and accommodate
newly formed tissue. Unfortunately, dressing material adsorbed with wound discharges provides conditions that are also favorable for bacterial growth. This has
given rise to a new generation of wound dressings with improved curative properties that provide a local antimicrobial effect by eluting various germicidal compounds.
Local delivery of antibiotics and disinfectants addresses the major disadvantages
of the systemic approach, namely poor penetration into ischemic and necrotic tissue
typical of post-traumatic and postoperative tissue, renal and liver complications,
and need for hospitalized monitoring (Price et al. 1996; Ruszczak and Friess 2003)
by maintaining a high local antibiotic concentration for an extended duration of
release without causing systemic toxicity (Gristina 1987; Springer et al. 2004;
Zalavras et al. 2004). The effectiveness of such devices is strongly dependent on
the rate and manner in which the drug is released (Wu and Grainger 2006). These
are determined by the host matrix into which the antibiotic is loaded, the type of
drug/disinfectant and its clearance rate. If the agent is released quickly, the entire
drug could be released before the infection is arrested. If release is delayed,
infection may set in further, thus making it difficult to manage the wound. The
release of antibiotics at levels below the minimum inhibitory concentration (MIC)
may lead to bacterial resistance at the release site and intensify infectious complications (Gold and Moellering 1996; Gransden 1997).
A local antibiotic release profile should therefore generally exhibit a considerable initial release rate in order to respond to the elevated risk of infection from
bacteria introduced during the initial shock, followed by a sustained release of
antibiotics at an effective level, long enough to inhibit latent infection (Ruszczak
and Friess 2003). The location, size and degree of injury as well as the rate of
tissue regeneration affect the wound healing process, and are reported to typically
last 3–7 weeks (Roenigk and Roenigk 1989). This section describes the main
features of wound dressings based on both synthetic and natural polymers.
�320
2.2
M. Zilberman et al.
Wound Dressings Based on Synthetic Polymers
A variety of dressings that contain and release antibiotic/disinfectant agents at the
wound surface have been introduced to the market. Most of these dressings have
been designed to provide controlled release of silver ions through a slow but
sustained release mechanism which helps avoid toxicity yet ensures delivery of a
therapeutic dose of silver ions to the wound (Heggers et al. 2005). Various
dressing formats, such as foams (Contreet1 antimicrobial foam, Coloplast), membranes (PolyMem Silver, Ferris), hydrocolloids (Urgotul SSD, Urgo), alginates
(Silvercel1, Johnson & Johnson), and hydrofibers (Aquacel, ConvaTec) are available. For instance, Acticoat1 (Smith and Nephew) is a 3-ply gauze dressing made
of an absorbent rayon polyester core, with upper and lower layers of a nanocrystalline silver-coated high-density polyethylene mesh (Fraser et al. 2004). It is applied
wet and is then moistened with water several times daily to allow the release of the
silver ions so as to provide an antimicrobial effect for three days. Concerns have
been raised by clinicians regarding the safety of the silver ions included in most of
these products. For example, it was found that a young person with 30% mixed
depth burns who received one week of local treatment with Acticoat1 exhibited
hepatotoxicity and argyria-like symptoms and the silver levels in his plasma and
urine as well as the liver enzymes were clearly elevated during the treatment
period. The authors therefore raised concern about potential silver toxicity and
suggested monitoring the silver levels in the plasma or urine during treatment
(Trop 2006).
In order to address this issue, the silver in Actisorb1 (Johnson & Johnson) is
impregnated into an activated charcoal cloth, after which it is encased in a nylon
sleeve which does not enable the silver in the product to be freely released at the
wound surface but nevertheless eradicates bacteria that adsorb onto the activated
charcoal component.
Suzuki et al. (Suzuki et al. 1997, 1998) presented a new concept for an antibiotic
delivery system that releases gentamicin only in the presence of wounds infected by
Pseudomonas aeruginosa. Gentamicin is bound to a polyvinyl alcohol derivative
(PVA) hydrogel through a specially developed peptide linker cleavable by a
proteinase. This allows gentamicin to be released at specific times and locations,
namely when and where P. aeruginosa infection occurs. PVA-(linker)-gentamicin
demonstrated selective release of gentamicin in P. aeruginosa-infected wound
fluid, and caused a significant reduction in its growth in vitro.
The substantial disadvantage of the majority of the available synthetic wound
dressings is the fact that like textile wound dressings, the necessary change of
dressings may be painful and increases the risk of secondary contamination.
Bioresorbable dressings successfully address this shortcoming since they degrade
from the wound surface once they have fulfilled their role. Film dressings made of
lactide caprolactone copolymers such as Topkin1 (Biomet, Europe) and Oprafol1 (Lohmann & Rauscher, Germany) are currently available (Jürgens et al.
2006). Biodegradation of the film occurs via hydrolysis of the copolymer into lactic
�Drug-Eluting Medical Implants
321
acid and 6-hydroxycaproic acid. During the hydrolytic process the pH shifts
towards the acidic range, with pH values as low as 3.6 measured in vitro (Jürgens
et al. 2006). Although these two dressings do not contain antibiotic agents, it is
claimed that the low pH values induced by the polymer’s degradation help reduce
bacterial growth (Varghese et al. 1986) and also promote epithelialization (Eisinger
et al. 1979). Furthermore, local lactate concentrations can stimulate local collagen
synthesis (Hutchinson and Furr 1985). Film dressings are better suited for small
wounds, since they lack an absorbing capacity and are impermeable to water vapors
and gasses, which may cause accumulation of wound fluids on larger wound
surfaces.
Fiber-based wound dressings with antibiotic delivery offer a good alternative to
the previously described films by providing a high surface area for controlled
release and improved absorbency and pliability. Antibiotics are typically
incorporated into these fibers during the process of fiber spinning (e.g., electrospinning or solution spinning). Katti et al. (2004) focused on the development of a
biodegradable non-woven PDLGA fiber mesh dressing, made by means of an
electrospinning process. Briefly, the process of electrospinning involves use of a
polymer solution that is contained in a syringe and held at the end of the needle by
its surface tension. Charge is induced on the solution by an external electric field to
overcome the surface tension and form a charged jet of solution. As this jet travels
through air, it experiences instabilities and follows a spiral path. Evaporation of the
solution leaves behind a charged polymer fiber that is collected on a grounded metal
screen. It was shown that the antibiotic cefazolin can be successfully incorporated
into the fibers in this way, and even though its release from these fibers has not yet
been reported, the effects of process parameters such as orifice diameter, applied
voltage and polymer and drug solution concentrations were investigated. Chang
et al. (2008) created gentamicin-eluting fibers by gravity spinning of a PCL with
gentamicin. The in vitro release of gentamicin from their fibers lasted 50 days
(Chang et al. 2008).
2.3
Wound Dressings Based on Natural Polymers
Natural polymers such as collagen (Lee et al. 2002; Park et al. 2004; Prabu et al.
2006; Shanmugasundaram et al. 2006; Sripriya et al. 2004), chitosan (Aoyagi et al.
2007; Chung et al. 1994; Mi et al. 2002; Muzzarelli et al. 1990; Rossi et al. 2007)
and alginate (Knill et al. 2004) have been investigated in various forms for wound
dressing applications as either main or additional components of the dressing
structure which are able to impact the local wound environment beyond moisture
management and elicit a cellular response. Collagen is the main structural protein of
the ECM, and was one of the first natural materials to be utilized for skin reconstruction and dressing applications. Collagen-based products have been available
commercially for over a decade, ranging from gels, pastes and powders to more
elaborate sheets, sponges, and composite structures. Collagen’s limitations as a
�322
M. Zilberman et al.
wound dressing ingredient are mainly due to its rapid biodegradation by collagenase and its susceptibility to bacterial invasion (Cairns et al. 1993; Maruguchi et al.
1994; Pruitt and Levine 1984; Trafny et al. 1998). Drug-eluting collagen sponges
have been found useful in both partial-thickness and full-thickness burn wounds.
Collatamp1 (Innocoll GmbH, Germany), Syntacoll (AG, Switzerland), Sulmycin1Implant (Schering-Plough, USA) and Septocoll1 (Biomet Merck, Germany) are
several such products which have been found to accelerate both granulation tissue
formation and epithelialization, as well as to protect the recovering tissue from
potential infection or re-infection by eluting gentamicin. In vitro, the drug is
released by a combination of diffusion and natural enzymatic breakdown of the
collagen matrix (Radu et al. 2002). A comprehensive clinical study of gentamicin
collagen sponges demonstrated their ability to induce high local concentrations of
gentamicin (up to 9,000 mg mL 1) at the wound site for at least 72 h while serum
levels remained well below the established toxicity threshold of 10–12 mg mL 1
(Ruszczak and Friess 2003).
Simple collagen sponge entrapment systems are characterized by high drug
release upon the wetting of the sponge, typically within 1–2 h of application.
Sripriya et al. (2004) have suggested improving the release profile of such systems
by using succinylated collagen which can create ionic bonds with the cationic
antibiotic ciprofloxacin so as to restrain its diffusion. It is claimed that in this way
ciprofloxacin release corresponds to the nature of the wound in line with the amount
of wound exudates absorbed in the sponge. Effective in vitro release from their
system was found to last five days, and was proven successful in controlling
infection in rats. Other studies have aimed to better control drug release or
improve wound healing properties by combining collagen with other synthetic
or natural biodegradable elements. Prabu et al. (2006) focused on achieving a
more sustained release of the antimicrobial agent and described a dressing made
from a mixture of collagen and PCL loaded with gentamicin and amikacin,
whereas Shanmugasundaram et al. (2006) chose to impregnate collagen with alginate
microspheres loaded with the antibacterial agent silver sulfadiazine (AgSD).
Other studies which focused on improving wound healing capabilities tried to
incorporate tobramycin, ciprofloxacin (Park et al. 2004) and AgSD (Lee et al. 2002)
into collagen hyaluronan-based dressings. The two latter studies did not show
conclusive evidence of improved healing properties compared to their control.
However, hyaluronan, a structure-stabilizing component of the ECM, is thought
to play a role in several aspects of the healing process with hyaluronan-based
dressings, and exhibited promising results in the management of chronic wounds
such as venous leg ulcers (Colletta et al. 2003; Taddeucci et al. 2004).
A wide range of studies describe the employment of the polysaccharide chitosan
and its partially deacetylated derivative chitin as structural materials analogous to
collagen for wound dressings. Both materials offer good wound protection and have
also been found to promote wound healing without excessive granulation tissue and
scar formation (Chung et al. 1994). Chitosan has also been documented as displaying considerable intrinsic antibacterial activity against a broad spectrum of bacteria
(Muzzarelli et al. 1990). Ignatova et al. (2006) reported the electrospinning of
�Drug-Eluting Medical Implants
323
chitosan with PVA into non-woven nanofiber mats with good in vitro bactericidal
activity against Staphylococcus aureus and Escherichia coli (Ignatova et al. 2006).
Another interesting fibrous form which combines the polysaccharides chitosan and
alginate was reported by Knill et al. (2004), who developed a composite structure of
calcium alginate filaments coated with chitosan, utilizing the cationic interaction of
chitosan with the anionic nature of alginate to bond the two together. It has been
suggested that the core alginate fiber may manage excess exudates whereas chitosan would provide antibacterial, hemostatic and wound healing properties. In this
case too, antibacterial testing of the fibers demonstrated an antibacterial effect.
Several attempts to improve the chitosan dressing’s antibacterial capabilities by
incorporating various agents such as AgSD (Mi et al. 2002), chlorhexidine diacetate
(Rossi et al. 2007) and minocycline hydrochloride (Aoyagi et al. 2007) have been
reported.
2.4
Composite Fiber Structures Loaded with Antibacterial
Drugs for Wound Healing Applications
Drug-eluting fibers can be used for various biomedical applications. Few controlledrelease fiber systems based on polymers have been investigated to date. The two
basic types of drug-loaded fibers that have been reported are monolithic fibers in
which the agent is dissolved or dispersed throughout the polymer fiber, and hollow
reservoir fibers in which the agent is added to the internal section of the fiber. The
advantages of drug-loaded fibers include ease of fabrication, high surface area
for controlled release and localized delivery of bioactive agents to their target.
Disadvantages of monolithic and reservoir fibers include poor mechanical properties due to drug incorporation and limitations in drug loading. Furthermore, many
small molecules and all proteins do not tolerate melt processing and organic
solvents.
In one of our recent studies we presented a new concept of core/shell fiber
structures which successfully meet these challenges (Zilberman et al. 2009). These
composite fibers combine a dense polyglyconate core fiber and a drug-loaded
porous 75/25 PDLGA shell structure, i.e., the antibacterial drug molecules are
located in a separate compartment (a “shell”) around the “core” fiber. A general
view of our composite fibers and a schematic representation showing the core/shell
concept are presented in Fig. 7a, b, respectively. The shell is prepared using freezedrying of inverted emulsions with mild processing conditions. These unique fibers
are designed to be used as basic elements of bioresorbable burn and ulcer dressings.
The main goal of these studies was to investigate core/shell fiber structures loaded
with the antibiotic drugs gentamicin sulfate, ceftazidime pentahydrate and mafenide acetate. The first two antibacterial drugs are broad spectrum antibiotics which
can be used systemically or locally, whereas the third is typically used in burn
dressings. Their investigation focused on the effects of the emulsion’s composition
�324
M. Zilberman et al.
Fig. 7 The structure of the composite core/shell fiber structures: (a) general view (photograph) of
the fiber, (b) schematic representation showing the core dense fiber and the porous drug-loaded
shell, (c) and (d) SEM fractographs of part of a core fiber coated with drug-loaded porous PDLGA
shell (cross section). Good adhesion between core and shell is demonstrated (Elsner and Zilberman
2008)
(formulation) on the shell microstructure, on the drug release profile from the fibers
and on the resulting bacterial inhibition.
The freeze-drying technique is unique in being able to preserve the liquid
structure in solids. We used this technique in order to produce the shell from
inverted emulsions in which the continuous phase contained polymer dissolved in
a solvent, with water and the antibiotics dissolved in it as the dispersed phase. SEM
fractographs showing the bulk morphology of the reference specimen are presented
in Fig. 7c, d. The quality of the interface between the fiber and the porous coating is
high (Fig. 7d), i.e., the preliminary surface treatment enabled good adhesion
between the core and the shell.
The shell’s microstructure affects the drug release profile and can also serve as a
good measure of the emulsion’s stability. The shell’s porous structure contains
round pores with a diameter of 0.5–5 mm and a porosity of 16–82%. The release
profiles commonly exhibited an initial burst effect accompanied by a decrease in
release rates with time over periods ranging from several days to 50 days, depending on the formulation (Elsner and Zilberman 2009). The effects of the emulsion’s
parameters on the shell’s microstructure and on the drug release profile are demonstrated on ceftazidime-loaded fibers and presented in Figs. 8 and 9, respectively.
Higher organic: aqueous (O:A) phase ratios, polymer content and molecular weight
(MW) reduced the burst release of antibiotics from the fibers and prolonged their
release due to changes in the shell’s structure. A higher MW and polymer content
�Drug-Eluting Medical Implants
325
Fig. 8 SEM fractographs of core/shell fibers showing the effect of change in certain formulation
parameters on shell microstructure. (a) reference formulation 5% (w/w) ceftazidime, 15% (w/v)
polymer (75/25 PDLGA, MW 100 KDa), O:A phase ratio of 6:1, (b) O:A modified to 12:1, (c)
polymer content modified to 20% (w/v) polymer, (d) higher polymer MW (modified to 240 kDa)
(Elsner and Zilberman 2008)
resulted in a larger effect on the microstructure and release profile than the O:A
phase ratio (Elsner and Zilberman 2008).
Albumin was found to be the most effective surfactant for stabilizing the
inverted emulsions (Elsner and Zilberman 2008; Zilberman et al. 2009). As a
surfactant, it is located at the interface between the aqueous phase and the organic
phase, reduces the interfacial tension between the two phases and therefore significantly decreases the pore size. It also enables a high encapsulation efficiency and a
relatively low burst release followed by a moderate release profile which enables
prolonged drug release. This behavior probably results from albumin’s ability to
bind the drug molecules (especially mafenide acetate) through specific interactions.
The effect of albumin on the release profile of mafenide acetate from the fibers is
presented in Fig. 10(a) and the release profiles of the three investigated antibiotics
from fibers with shells that contain albumin are presented in Fig. 10(b). The ability
of albumin to bind APIs is well-known (Foye et al. 1998). Albumin can interact
with acidic or basic agents via van der Waals dispersion forces, hydrogen bonds and
ionic interactions. Based on these results, we chose albumin as the preferred
surfactant in our systems.
We also performed microbiological experiments in order to monitor the effectiveness of various concentrations of the antibiotic released from the fibers in terms
of the residual bacteria compared with the initial number of bacteria. Bacteria in
PBS only served as the control. We chose the following three types of gentamicineluting fibers with different release profiles (Fig. 11):
�326
M. Zilberman et al.
Fig. 9 In vitro release of ceftazidime from core/shell fibers demonstrating the effect of change in
certain formulation parameters compared to the reference formulation: (a) effect of O:A phase
ratio: ■ – 6:1, ● – 8:1, ~ – 10:1, r – 12:1, (b) effect of polymer content: ■ – 15% (w/v), ● – 17.5
(w/v), r – 20% (w/v), (c) effect of polymer MW: ■ – 100 kDa, ● – 240 kDa (Elsner and
Zilberman 2008)
�Drug-Eluting Medical Implants
327
Fig. 10 Drug release profiles from fibers containing albumin as surfactant: (a) mafenide acetate
release profiles from core/shell fiber structures containing 5% (w/w) drug, 15% (w/v) polymer and
O:A phase ratio of 6:1: ~ no surfactant r 0.5% (w/v) surfactant; ■ 1% (w/v) surfactant. (b)
Antibiotic release from fibers containing 15% (w/w) polymer, O:A phase ratio of 6:1, 5% (w/w)
drug and 1% (w/v) albumin: ■
mafenide, ~ – ceftazidime, ● – gentamicin (Elsner and
Zilberman 2008)
1. Fibers with a shell based on 26.7% (w/v) polymer, 20% (w/v) gentamicin, 6:1 O:
A phase ratio and albumin as surfactant. These fibers demonstrated a moderate
burst release of 32% followed by a moderate release profile.
2. Fibers with a shell based on 20% (w/v) polymer, 20% (w/v) gentamicin, 6:1 O:
A. These fibers demonstrated a high burst release of approximately 60%.
3. Fibers with a shell based on 26.7% (w/v) polymer, 5% (w/v) gentamicin, 6:1 O:
A phase ratio and albumin as surfactant. These fibers demonstrated a low burst
release of 13% during the first day and 60% within three days. After three days
the release pattern was similar to that of sample II.
�328
M. Zilberman et al.
Fig. 11 Gentamicin’s release profile from fiber samples which were used for microbiological
evaluation: ■ – sample I (26.7% (w/v) polymer, 20% (w/v) drug, 6:1 O:A phase ratio and 5%
(w/v) albumin), ● – sample II (20% (w/v) polymer, 20% (w/v) drug, 6:1 O:A), ~ – sample III
(26.7% (w/v) polymer, 5% (w/v) drug, 6:1 O:A phase ratio and 5% (w/v) albumin) (Zilberman
et al. 2009)
The bacterial strains used in this study were S. aureus, S. epidermidis and
Pseudomonas aeruginosa. Their minimal inhibitory concentration (MIC) values
are 2.5, 5 and 6.3 mg mL 1, respectively. All three strains were clinically isolated.
These strains were chosen because they are prevalent in wound infections, especially S. aureus and P. aeruginosa. The third strain, S. epidermidis, usually comprises the normal flora of the skin. However, under grave conditions it can cause
wound infections. Moreover, these bacteria can produce bio-films, which prevent
antibiotics from reaching the target, therefore causing resistance. The bacteria were
added at the beginning of the fibers’ release in order to simulate contamination at
the time of implantation. The results for all three bacterial types when using a
relatively high initial bacterial concentration of 1�107 CFU mL 1 are presented in
Fig. 12. The released gentamicin significantly decreased bacterial viability, and
practically no bacteria survived after two days. The fiber preparation did not affect
gentamicin’s potency as an antibacterial agent. Our new fiber structures are thus
effective against the relevant bacterial strains and can be used as basic elements of
bioresorbable drug-eluting wound dressings.
In practice, a wound dressing can be woven from a combination of several types
of fibers to create a resultant release profile which is the product of several release
profiles or drug types. The diverse profiles achieved in this study with higher and
�Drug-Eluting Medical Implants
329
Fig. 12 Number of colony forming units (CFU) versus time, when an initial bacterial concentration of 1�107 CFU/mL was used: A – Staphylococcus aureus, B – Staphylococcus epidermidis,
C – Pseudomonas aeruginosa. The releasing fibers are: – sample I (26.7% (w/v) polymer, 20%
(w/v) drug, 6:1 O:A phase ratio and 5% (w/v) albumin), – sample II (20% (w/v) polymer, 20%
(w/v) drug, 6:1 O:A), – sample III (26.7% (w/v) polymer, 5% (w/v) drug, 6:1 O:A phase ratio
and 5% (w/v) albumin), – control – reference fiber without gentamicin (Zilberman et al. 2009)
lower burst release rates and with varying elution spans may serve as a good basis
for further in vivo examination of the fibers in order to create the ideal profile for a
particular wound-healing application.
�330
M. Zilberman et al.
In conclusion, this section described wound dressings with emphasis on
approaches for local drug release for prevention of bacterial infections that accompany the initial period of shock, due to wounds with tissue loss. Drug-eluting wound
dressings based on both synthetic and natural polymers were described in terms of
matrix material, processing techniques, dressing format and drug release profile.
Our novel composite antibiotic-eluting composite fibers which are designed to be
used as basic elements of wound dressings were described. Recent advances in the
field of wound dressings aim to enable improvements in the patient’s quality of life
due to higher biocompatibility and controlled release of bioactive agents that
enhances the healing process and eliminate the need for change of dressing,
which is painful and increases the risk for secondary contamination. Wound dressings that combine controlled release of antibiotics with controlled release of
growth factors will further advance the field of wound healing.
3 Protein-Eluting Scaffolds for Tissue Regeneration
Organ or tissue deficiency or loss is one of the most frequent and devastating
problems in human healthcare. Tissue engineering is described as “an interdisciplinary field that applies the principles of engineering and life sciences towards the
development of biological substitutes that restore, maintain, or improve tissue
function or a whole organ” (Langer and Vacanti 1993). One of the major
approaches in tissue engineering is scaffolds that elute bioactive agents. Upon
implantation of such scaffolds, cells from the body are recruited to the site and a
tissue can be formed (Howard et al. 2008). Growth factors are essential for
promoting cell proliferation and differentiation; however, their direct administration is problematic due to their poor in vivo stability (Babensee et al. 2000; Chen
and Mooney 2003). It is therefore necessary to develop scaffolds with controlled
delivery of bioactive agents that can achieve prolonged availability as well as
protection of these bioactive agents which might otherwise undergo rapid proteolysis (Buket Basmanav et al. 2008; Zhu et al. 2008). The main obstacle to successful
incorporation and delivery of small molecules as well as proteins from scaffolds is
their inactivation during the process of scaffold manufacture due to exposure to
high temperatures or harsh chemical environments, which is why it is necessary to
develop a method that minimizes protein inactivation.
Growth factors can be attached onto scaffolds by adsorption to the surface of the
scaffolds. For example, Elcin and Elcin (2006) formed sponges made of PLGA
using a solvent casting and particulate leaching method. The sponges were
immersed overnight in a solution containing vascular endothelial growth factor
(VEGF) at a temperature of 4� C and then freeze-dried. VEGF release from the
sponges was examined in vivo in Wistar rats. Rapid release of VEGF was observed
in the first two days, followed by a slow release for two weeks. Furthermore, the
released VEGF retained its bioactivity.
�Drug-Eluting Medical Implants
331
Growth factors can also be incorporated into scaffolds directly during the
fabrication process. Liu et al. (2003) fabricated thin films using the solvent casting
and particulate leaching technique. A solution containing bone morphogenetic
protein 7 (BMP-7) was added to the polymer solution. The final solution was
exposed to 20� C and the solvent was slowly evaporated. Cells from a muscle
tissue of New Zealand white rabbits were seeded on the BMP-7 eluted films and
differentiated into osteoblast-like cells.
Whang et al. (1995, 1998) presented an important method for incorporating
bioactive molecules during the scaffold-production processing, based on the technique of freeze-drying an inverted emulsion. This method enables the production of
highly porous scaffolds with a controllable pore size and the ability to incorporate
and release proteins in a controlled manner. Since the bioactive molecules are
incorporated into the aqueous solution of the emulsion, very sensitive bioactive
molecules can be incorporated without exposing them to organic solvents, thus
preserving their activity. A recombinant human bone morphogenetic protein
(rhBMP-2) was incorporated and released in vivo in a rat ectopic bone induction
assay from a scaffold produced by freeze-drying an inverted emulsion. The rhBMP2 incorporated scaffold-induced bone formation, which confirmed the viability of
the rhBMP-2 released from the scaffold. Contact radiography, radiomorphometry,
histology, and histomorphometry revealed significantly more bone in the rhBMP2 implants than in the controls.
In one of our recent studies we investigated highly porous scaffolds that were
produced using the technique of freeze-drying inverted emulsions (Grinberg 2007).
The enzyme horseradish peroxidase (HRP) was used as a protein source in order to
examine the effect of the emulsion’s formulation on the film microstructure and on
the resulting cumulative protein release. A porous structure with 72–93% porosity
and partially interconnected pores was obtained. The released profiles usually
exhibited an initial burst effect, accompanied by a decrease in release rate with
time, as is typical of diffusion-controlled systems. The release profile was mostly
affected by the polymer’s initial molecular weight and the enzyme. An increase in
the polymer’s initial molecular weight resulted in a decrease in the initial burst
effect and in the release rate due to changes in the microstructure. An increase in the
enzyme content resulted in an increase in the initial burst effect and in the release
rate due to a higher driving force for diffusion. The other emulsion parameters had
minor effects on the release profile in the examined range. We demonstrated that
appropriate selection of the inverted emulsion’s parameters results in the desired
release profile which can be adjusted to the specific application. We observed cell
adherence and growth with fibroblast characteristics on the film. The studied films
are thus biocompatible and can be used as a controlled release system for bioactive
agents in tissue regeneration applications.
Another approach for encapsulation of bioactive molecules in scaffolds is composite scaffold/microsphere structures. The growth factors are initially encapsulated
into the microspheres, and the microspheres can then be integrated into scaffolds.
Zhu et al. (2008) demonstrated encapsulation and controlled release of hepatocyte
growth factor (HGF) from such scaffolds. A mixture of poly(3-hydroxybutyrate-
�332
M. Zilberman et al.
co-3-hydroxyvalerate) (PHBV) and PLGA was chosen as the microsphere/polymer
matrix. The PLGA/PHBV microspheres had a core/shell structure and the released
HGF preserved its bioactivity for at least 40 days. Moreover, the three-dimensional
microsphere scaffolds were more effective in maintaining the viability and phenotype of the primary hepatocytes. Wei et al. (2006) reported that microspheres
can also be incorporated into scaffolds using the post-seeding method. PLGA
microspheres consisting of platelet-derived growth factor-BB (PDGF-BB) were
incorporated into a poly(L-lactic acid) (PLLA) nanofiber scaffold. The released
PDGF-BB from the microspheres and from the microsphere-incorporated scaffolds
remained bioactive. Furthermore, the burst effect was significantly lower in the
microsphere-incorporated scaffolds than in the microspheres.
In conclusion, the field of active scaffolds for tissue regeneration is relatively
new and only a small number of such scaffolds have been developed to date. Three
approaches to protein (growth factor) incorporation into bioresorbable scaffolds
were presented in this section: adsorption onto the surface of the scaffold, freezedrying of inverted emulsions for incorporation of the bioactive agents into the
scaffold during its formation process, and composite scaffold/microsphere structures. It is important to note that incorporation of protein in all three approaches is
carried out such that it preserves the activity, i.e., without exposure to elevated
temperatures or organic solvents.
References
Abizaid A, Lansky AJ, Fitzgerald PJ, Tanajura LF, Feres F, Staico R, Mattos L, Abizaid A,
Chaves A, Centemero M, Sousa AG, Sousa JE, Zaugg MJ, Schwartz LB (2007) Percutaneous
coronary revascularization using a trilayer metal phosphorylcholine-coated zotarolimuseluting stent. Am J Cardiol 99:1403–1408
Alexis, F., et al., (2004) In vitro study of release mechanisms of paclitaxel and rapamycin from
drug-incorporated biodegradable stent matrices. J Control Release 98(1):67–74
Aoki J, Abizaid AC, Serruys PW, Ong AT, Boersma E, Sousa JE, Bruining N (2005a) Evaluation
of four-year coronary artery response after sirolimus-eluting stent implantation using serial
quantitative intravascular ultrasound and computer-assisted grayscale value analysis for plaque
composition in event-free patients. J Am Coll Cardiol 46:1670–1676
Aoki J, Serruys PW, van Beusekom H, Ong AT, McFadden EP, Sianos G, van der Giessen WJ,
Regar E, de Feyter PJ, Davis HR, Rowland S, Kutryk MJ (2005b) Endothelial progenitor cell
capture by stents coated with antibody against CD34: the HEALING-FIM (Healthy Endothelial Accelerated Lining Inhibits Neointimal Growth-First In Man) registry. J Am Coll Cardiol
45:1574–1579
Aoyagi S, Onishi H, Machida Y (2007) Novel chitosan wound dressing loaded with minocycline
for the treatment of severe burn wounds. Int J Pharm 330:138–145
Ardissino D, Cavallini C, Bramucci E, Indolfi C, Marzocchi A, Manari A, Angeloni G, Carosio G,
Bonizzoni E, Colusso S, Repetto M, Merlini PA (2004) Sirolimus-eluting vs uncoated
stents for prevention of restenosis in small coronary arteries: a randomized trial. J Am Med
Assoc 292:2727–2734
Babapulle MN, Eisenberg MJ (2002) Coated stents for the prevention of restenosis: part II.
Circulation 106:2859–2866
�Drug-Eluting Medical Implants
333
Babensee JE, McIntire LV, Mikos AG (2000) Growth factor delivery for tissue engineering.
Pharm Res 17:497–504
Beohar N, Davidson CJ, Kip KE, Goodreau L, Vlachos HA, Meyers SN, Benzuly KH, Flaherty JD,
Ricciardi MJ, Bennett CL, Williams DO (2007) Outcomes and complications associated with
off-label and untested use of drug-eluting stents. J Am Med Assoc 297:1992–2000
Berg R, Aragon J, Royter V, Shanley JF, Cogert G, Vermani R, Kar S, Eigler N, Litvack F (2007)
Pimecrolimus and dual pimecrolimus-paclitaxel eluting stents decrease neointimal proliferation in a porcine model. Catheter Cardiovasc Interv 70:871–879
Buchbinder M (2007) Biodegradable stents: BTI approach. Foundation for Cardiovascular
Medicine, www.summitmd.com/pdf/pdf/070601_7.pdf
Buket Basmanav F, Kose GT, Hasirci V (2008) Sequential growth factor delivery from complexed
microspheres for bone tissue engineering. Biomaterials 29:4195–4204
Cairns BA, deSerres S, Peterson HD, Meyer AA (1993) Skin replacements. The biotechnological
quest for optimal wound closure. Arch Surg 128:1246–1252
Chang HI, Lau YC, Yan C, Coombes AG (2008) Controlled release of an antibiotic, gentamicin
sulphate, from gravity spun polycaprolactone fibers. J Biomed Mater Res A 84:230–237
Chen RR, Mooney DJ (2003) Polymeric growth factor delivery strategies for tissue engineering.
Pharm Res 20:1103–1112
Chevalier B, Serruys PW, Silber S, Garcia E, Suryapranata H, Hauptmann K, Wijns W, Schuler G,
Fath-Ordoubadi F, Worthley S, Thuesen L, Meredith I, Bressers M, Nagai H, Paunovic D
(2007) Randomised comparison of NoboriTM, biolimus A9-eluting coronary stent with a
Taxus1, paclitaxel-eluting coronary stent in patients with stenosis in native coronary arteries:
the Nobori 1 trial. Euro Intervention 2:426–434
Chorny M, Fishbein I, Golomb G (2000) Drug delivery systems for the treatment of restenosis. Crit
Rev Ther Drug Carrier Syst 17:249–284
Chung LY, Schmidt RJ, Hamlyn PF, Sagar BF, Andrews AM, Turner TD (1994) Biocompatibility
of potential wound management products: fungal mycelia as a source of chitin/chitosan and
their effect on the proliferation of human F1000 fibroblasts in culture. J Biomed Mater Res
28:463–469
Colletta V, Dioguardi D, Di Lonardo A, Maggio G, Torasso F (2003) A trial to assess the
efficacy and tolerability of Hyalofill-F in non-healing venous leg ulcers. J Wound Care
12:357–360
Colombo A, Drzewiecki J, Banning A, Grube E, Hauptmann K, Silber S, Dudek D, Fort S, Schiele
F, Zmudka K, Guagliumi G, Russell ME (2003) Randomized study to assess the effectiveness
of slow- and moderate-release polymer-based paclitaxel-eluting stents for coronary artery
lesions. Circulation 108:788–794
Commandeur S, van Beusekom HM, van der Giessen WJ (2006) Polymers, drug release, and drugeluting stents. J Interv Cardiol 19:500–506
Corporation BS (2007) TAXUS IV final 5-year outcomes, taken from Boston Scientific web site:
www.bostonscientific.com, Boston Scientific Corporation
Creel CJ, Lovich MA, Edelman ER (2000) Arterial paclitaxel distribution and deposition. Circ Res
86:879–884
Daemen J, Ong AT, Stefanini GG, Tsuchida K, Spindler H, Sianos G, de Jaegere PP, van Domburg
RT, Serruys PW (2006) Three-year clinical follow-up of the unrestricted use of sirolimuseluting stents as part of the Rapamycin-Eluting Stent Evaluated at Rotterdam Cardiology
Hospital (RESEARCH) registry. Am J Cardiol 98:895–901
Daemen J, Serruys PW (2007) Drug-eluting stent update 2007: part I. A survey of current and
future generation drug-eluting stents: meaningful advances or more of the same? Circulation
116:316–328
Dawkins K, Verheye S, Schühlen H, Dens J, Mudra H, Rutsch W, Stella P, Di Mario C, Thomas M,
Serruys PW, Colombo A (2007) The European cobalt STent with antiproliferative for restenosis trial (EuroSTAR): 12 month results. Eur Heart J 3:82–88
Dawkins KD, Grube E, Guagliumi G, Banning AP, Zmudka K, Colombo A, Thuesen L,
Hauptman K, Marco J, Wijns W, Popma JJ, Koglin J, Russell ME (2005) Clinical efficacy of
polymer-based paclitaxel-eluting stents in the treatment of complex, long coronary artery
�334
M. Zilberman et al.
lesions from a multicenter, randomized trial: support for the use of drug-eluting stents in
contemporary clinical practice. Circulation 112:3306–3313
Duda SH, Poerner TC, Wiesinger B, Rundback JH, Tepe G, Wiskirchen J, Haase KK (2003) Drugeluting stents: potential applications for peripheral arterial occlusive disease. J Vasc Interv
Radiol 14:291–301
Eisinger M, Lee JS, Hefton JM, Darzynkiewicz Z, Chiao JW, de Harven E (1979) Human epidermal
cell cultures: growth and differentiation in the absence of differentiation in the absence of dermal
components or medium supplements. Proc Natl Acad Sci USA 76:5340–5344
Elcin AE, Elcin YM (2006) Localized angiogenesis induced by human vascular endothelial
growth factor-activated PLGA sponge. Tissue Eng 12:959–968
Elezi S, Kastrati A, Neumann FJ, Hadamitzky M, Dirschinger J, Schomig A (1998) Vessel size and
long-term outcome after coronary stent placement. Circulation 98:1875–1880
Elsner JJ, Zilberman M (2009) Antibiotic-eluting bioresorbable composite fibers for wound
healing applications: microstructure, drug delivery and mechanical properties. Acta Biomater
5:2872–2883
Fajadet J, Wijns W, Laarman GJ, Kuck KH, Ormiston J, Munzel T, Popma JJ, Fitzgerald PJ, Bonan
R, Kuntz RE (2006) Randomized, double-blind, multicenter study of the Endeavor zotarolimuseluting phosphorylcholine-encapsulated stent for treatment of native coronary artery lesions:
clinical and angiographic results of the ENDEAVOR II trial. Circulation 114:798–806
Farb A, Sangiorgi G, Carter AJ, Walley VM, Edwards WD, Schwartz RS, Virmani R (1999)
Pathology of acute and chronic coronary stenting in humans. Circulation 99:44–52
Finn AV, Joner M, Nakazawa G, Kolodgie F, Newell J, John MC, Gold HK, Virmani R (2007)
Pathological correlates of late drug-eluting stent thrombosis: strut coverage as a marker of
endothelialization. Circulation 115:2435–2441
Fischman DL, Leon MB, Baim DS, Schatz RA, Savage MP, Penn I, Detre K, Veltri L, Ricci D,
Nobuyoshi M, Cleman M, Heuser R, Almond D, Teirstein PS, Fish RD, Colombo A, Brinker J,
Moses J, Shaknovish A, Hirshfeld J, Bailey S, Ellis S, Rake R, Goldberg S (1994) A
randomized comparison of coronary-stent placement and balloon angioplasty in the treatment
of coronary artery disease. Stent restenosis study investigators. N Engl J Med 331:496–501
Foye WO, Lemke TL, Williams DA (1998) Principles of medicinal chemistry, 3rd edn. Lea &
Febiger, Baltimore, MD
Fraser JF, Bodman J, Sturgess R, Faoagali J, Kimble RM (2004) An in vitro study of the antimicrobial efficacy of a 1% silver sulphadiazine and 0.2% chlorhexidine digluconate cream,
1% silver sulphadiazine cream and a silver coated dressing. Burns 30:35–41
Freed M, Safian RD, Grines C (1996) Manual of interventional cardiology. Physicians’ Press,
Birmingham, MI
Gao RL, Xu B, Lu SZ, Chen JL, Han YL, Chen JZ, Gai LY, Ge JB, Wang WM, Du ZM, Huo Y,
Wang LF, Gao W, Chen JY, He B, Jia GL, Yang ZJ, Cao KJ, Li WM, Shen WF, Wan Z,
Huang DJ, Zhu GY (2008) Safety and efficacy of the CYPHER select sirolimus-eluting stent in
the “Real World”–clinical and angiographic results from the China CYPHER select registry.
Int J Cardiol 125:339–346
George J, Sack J, Barshack I, Keren P, Goldberg I, Haklai R, Elad-Sfadia G, Kloog Y, Keren G
(2004) Inhibition of intimal thickening in the rat carotid artery injury model by a nontoxic Ras
inhibitor. Arterioscler Thromb Vasc Biol 24:363–368
Gershlick A, De Scheerder I, Chevalier B, Stephens-Lloyd A, Camenzind E, Vrints C, Reifart N,
Missault L, Goy JJ, Brinker JA, Raizner AE, Urban P, Heldman AW (2004) Inhibition of
restenosis with a paclitaxel-eluting, polymer-free coronary stent: the European evaLUation of
pacliTaxel Eluting Stent (ELUTES) trial. Circulation 109:487–493
Gershlick AH (2005) Drug eluting stents in 2005. Heart 91(Suppl 3):iii24–iii31
Gold HS, Moellering RC Jr (1996) Antimicrobial-drug resistance. N Engl J Med 335:1445–1453
Gransden WR (1997) Antibiotic resistance. Nosocomial gram-negative infection. J Med Microbiol
46:436–439
�Drug-Eluting Medical Implants
335
Grinberg O (2007) Highly porous bioresorbable scaffolds with controlled release of bioactive
agents for tissue regeneration applications. MSc thesis. Tel Aviv University
Gristina AG (1987) Biomaterial-centered infection: microbial adhesion versus tissue integration.
Science 237:1588–1595
Grube E (2008) Novel drug eluting stent system for customised treatment of coronary lesions:
CUSTOM I feasibility trial 24 month results. Eur Heart J 4:71–76
Grube E, Bullesfeld L (2002) Initial experience with paclitaxel-coated stents. J Interv Cardiol
15:471–475
Grube E, Sonoda S, Ikeno F, Honda Y, Kar S, Chan C, Gerckens U, Lansky AJ, Fitzgerald PJ
(2004) Six- and twelve-month results from first human experience using everolimus-eluting
stents with bioabsorbable polymer. Circulation 109:2168–2171
Halkin A, Stone GW (2004) Polymer-based paclitaxel-eluting stents in percutaneous coronary
intervention: a review of the TAXUS trials. J Interv Cardiol 17:271–282
Heggers J, Goodheart RE, Washington J, McCoy L, Carino E, Dang T, Edgar P, Maness C,
Chinkes D (2005) Therapeutic efficacy of three silver dressings in an infected animal model.
J Burn Care Rehabil 26:53–56
Heldman AW, Cheng L, Jenkins GM, Heller PF, Kim DW, Ware M Jr, Nater C, Hruban RH,
Rezai B, Abella BS, Bunge KE, Kinsella JL, Sollott SJ, Lakatta EG, Brinker JA, Hunter WL,
Froehlich JP (2001) Paclitaxel stent coating inhibits neointimal hyperplasia at 4 weeks in a
porcine model of coronary restenosis. Circulation 103:2289–2295
Hofma SH, van der Giessen WJ, van Dalen BM, Lemos PA, McFadden EP, Sianos G, Ligthart JM,
van Essen D, de Feyter PJ, Serruys PW (2006) Indication of long-term endothelial dysfunction
after sirolimus-eluting stent implantation. Eur Heart J 27:166–170
Holmes DR Jr, Leon MB, Moses JW, Popma JJ, Cutlip D, Fitzgerald PJ, Brown C, Fischell T,
Wong SC, Midei M, Snead D, Kuntz RE (2004) Analysis of 1-year clinical outcomes in the
SIRIUS trial: a randomized trial of a sirolimus-eluting stent versus a standard stent in patients
at high risk for coronary restenosis. Circulation 109:634–640
Howard D, Buttery LD, Shakesheff KM, Roberts SJ (2008) Tissue engineering: strategies, stem
cells and scaffolds. J Anat 213:66–72
Hutchinson FG, Furr BJ (1985) Biodegradable polymers for the sustained release of peptides.
Biochem Soc Trans 13:520–523
Ignatova M, Starbova K, Markova N, Manolova N, Rashkov I (2006) Electrospun nano-fibre mats
with antibacterial properties from quaternised chitosan and poly(vinyl alcohol). Carbohydr Res
341:2098–2107
Iofina E, Langenberg R, Blindt R, Kuhl H, Kelm M, Hoffmann R (2006) Polymer-based paclitaxel-eluting stents are superior to nonpolymer-based paclitaxel-eluting stents in the treatment
of de novo coronary lesions. Am J Cardiol 98:1022–1027
Joner M, Finn AV, Farb A, Mont EK, Kolodgie FD, Ladich E, Kutys R, Skorija K, Gold HK,
Virmani R (2006) Pathology of drug-eluting stents in humans: delayed healing and late
thrombotic risk. J Am Coll Cardiol 48:193–202
Joner M, Nakazawa G, Finn AV, Quee SC, Coleman L, Acampado E, Wilson PS, Skorija K,
Cheng Q, Xu X, Gold HK, Kolodgie FD, Virmani R (2008) Endothelial cell recovery between
comparator polymer-based drug-eluting stents. J Am Coll Cardiol 52:333–342
Jones SA, Bowler PG, Walker M, Parsons D (2004) Controlling wound bioburden with a novel
silver-containing hydrofiber dressing. Wound Repair Regen 12:288–294
Jürgens C, Schulz AP, Porté T, Faschingbauer M, Seide K (2006) Biodegradable films in trauma
and orthopedic surgery. Eur J Trauma 2:160–171
Kastrati A, Schomig A, Elezi S, Schuhlen H, Dirschinger J, Hadamitzky M, Wehinger A,
Hausleiter J, Walter H, Neumann FJ (1997) Predictive factors of restenosis after coronary
stent placement. J Am Coll Cardiol 30:1428–1436
Katti DS, Robinson KW, Ko FK, Laurencin CT (2004) Bioresorbable nanofiber-based systems for
wound healing and drug delivery: optimization of fabrication parameters. J Biomed Mater Res
B Appl Biomater 70:286–296
�336
M. Zilberman et al.
Kau U (2007) CObalt Chromium STent with antiproliferative for restenosis trial in India
(COSTAR I). Indian Heart J 59:167–172
Kloog Y, Cox AD (2004) Prenyl-binding domains: potential targets for Ras inhibitors and anticancer drugs. Semin Cancer Biol 14:253–261
Knill CJ, Kennedy JF, Mistry J, Miraftab M, Smart G, Groocock MR, Williams HJ (2004) Alginate
fibres modified with unhydrolysed and hydrolysed chitosans for wound dressings. Carbohydr
Polym 55:65–76
Kraitzer A, Kloog Y, Zilberman M (2007) Approaches for prevention of restenosis. J Biomed
Mater Res B Appl Biomater 85B:583–603
Kraitzer A, Kloog Y, Zilberman M (2009) Novel farnesylthiosalicylate (FTS)-eluting composite
structures. Eur J Pharm Sci 37:351–362
Kraitzer A, Ofek L, Schreiber R, Zilberman M (2008) Long-term in vitro study of paclitaxeleluting bioresorbable core/shell fiber structures. J Control Release 126:139–148
Kraitzer A, Zilberman M (2007) Paclitaxel-loaded composite fibers: microstructure and emulsion
stability. J Biomed Mater Res A 81:427–436
Kraitzer A, Zilberman M (2009) Novel Farnesylthiosalicylate (FTS) –Eluting Composite Structures. J Control Release 37(3–4):351–362
Krucoff MW, Kereiakes DJ, Petersen JL, Mehran R, Hasselblad V, Lansky AJ, Fitzgerald PJ,
Garg J, Turco MA, Simonton CA 3rd, Verheye S, Dubois CL, Gammon R, Batchelor WB,
O’Shaughnessy CD, Hermiller JB Jr, Schofer J, Buchbinder M, Wijns W (2008) A novel
bioresorbable polymer paclitaxel-eluting stent for the treatment of single and multivessel
coronary disease: primary results of the COSTAR (Cobalt Chromium Stent With Antiproliferative for Restenosis) II study. J Am Coll Cardiol 51:1543–1552
Kutryk MJ (2003) Drug eluting stents for the treatment of coronary artery disease part 4: New
results from clinical trials and future directions, Cardiology Rounds VIII, issue 10
Lagerqvist B, James SK, Stenestrand U, Lindback J, Nilsson T, Wallentin L (2007) Long-term
outcomes with drug-eluting stents versus bare-metal stents in Sweden. N Engl J Med
356:1009–1019
Langer R, Vacanti JP (1993) Tissue engineering. Science 260:920–926
Lansky AJ, Costa RA, Mintz GS, Tsuchiya Y, Midei M, Cox DA, O’Shaughnessy C, Applegate
RA, Cannon LA, Mooney M, Farah A, Tannenbaum MA, Yakubov S, Kereiakes DJ, Wong SC,
Kaplan B, Cristea E, Stone GW, Leon MB, Knopf WD, O’Neill WW (2004) Non-polymerbased paclitaxel-coated coronary stents for the treatment of patients with de novo coronary
lesions: angiographic follow-up of the DELIVER clinical trial. Circulation 109:1948–1954
Lee SH, Szinai I, Carpenter K, Katsarava R, Jokhadze G, Chu CC, Huang Y, Verbeken E,
Bramwell O, De Scheerder I, Hong MK (2002) In-vivo biocompatibility evaluation of stents
coated with a new biodegradable elastomeric and functional polymer. Coron Artery Dis
13:237–241
Lewis AL, Tolhurst LA, Stratford PW (2002) Analysis of a phosphorylcholine-based polymer
coating on a coronary stent pre- and post-implantation. Biomaterials 23:1697–1706
Lincoff A.M, et al (1997) Sustained local delivery of dexamethasone by a novel intravascular
eluting stent to prevent restenosis in the porcine coronary injury model. J Am Coll Cardiol
29:808–816
Liu X, Huang Y, Hanet C, Vandormael M, Legrand V, Dens J, Vandenbossche JL, Missault L,
Vrints C, De Scheerder I (2003) Study of antirestenosis with the BiodivYsio dexamethasoneeluting stent (STRIDE): a first-in-human multicenter pilot trial. Catheter Cardiovasc Interv
60:172–178 discussion 179
Maruguchi T, Maruguchi Y, Suzuki S, Matsuda K, Toda K, Isshiki N (1994) A new skin
equivalent: keratinocytes proliferated and differentiated on collagen sponge containing fibroblasts. Plast Reconstr Surg 93:537–544 Discussion 545-6
Mauri L, Hsieh WH, Massaro JM, Ho KK, D’Agostino R, Cutlip DE (2007) Stent thrombosis in
randomized clinical trials of drug-eluting stents. N Engl J Med 356:1020–1029
Medsystems C (2007) Conor Medsystems, LLC Reports COSTAR II Pivotal Drug-Eluting Stent
Trial Conclusions. Johnson & Johnson press release
�Drug-Eluting Medical Implants
337
Meredith IT, Ormiston J, Whitbourn R, Kay IP, Muller D, Popma JJ, Cutlip DE, Fitzgerald PJ
(2007a) Four-year clinical follow-up after implantation of the endeavor zotarolimus-eluting
stent: ENDEAVOR I, the first-in-human study. Am J Cardiol 100:56M–61M
Meredith IT, Worthley S, Whitbourn R, Walters D, Popma J, Cutlip D, Fitzgerald P (2007b) The
next-generation EndeavorTM ResoluteTM stent: 4-month clinical and angiographic results from
the ResoluteTM first-in-man trial. Euro Intervention 3:50–53
Mi FL, Wu YB, Shyu SS, Schoung JY, Huang YB, Tsai YH, Hao JY (2002) Control of wound
infections using a bilayer chitosan wound dressing with sustainable antibiotic delivery.
J Biomed Mater Res 59:438–449
Miyazawa A, Ako J, Hongo Y, Hur SH, Tsujino I, Courtney BK, Hassan AH, Kandzari DE, Honda
Y, Fitzgerald PJ (2008) Comparison of vascular response to zotarolimus-eluting stent versus
sirolimus-eluting stent: intravascular ultrasound results from ENDEAVOR III. Am Heart J
155:108–113
Moreno R, Macaya C (2005) Stent-based delivered anti-proliferative drugs in the prevention of
coronary stent restenosis. Curr Med Chem Cardiovasc Hematol Agents 3:221–229
Morice MC, Colombo A, Meier B, Serruys P, Tamburino C, Guagliumi G, Sousa E, Stoll HP
(2006) Sirolimus- vs paclitaxel-eluting stents in de novo coronary artery lesions: the REALITY
trial: a randomized controlled trial. J Am Med Assoc 295:895–904
Morice MC, Serruys PW, Barragan P, Bode C, Van Es GA, Stoll HP, Snead D, Mauri L, Cutlip
DE, Sousa E (2007) Long-term clinical outcomes with sirolimus-eluting coronary stents: fiveyear results of the RAVEL trial. J Am Coll Cardiol 50:1299–1304
Morice MC, Serruys PW, Sousa JE, Fajadet J, Ban Hayashi E, Perin M, Colombo A, Schuler G,
Barragan P, Guagliumi G, Molnar F, Falotico R (2002) A randomized comparison of a
sirolimus-eluting stent with a standard stent for coronary revascularization. N Engl J Med
346:1773–1780
Moses JW, Leon MB, Popma JJ, Fitzgerald PJ, Holmes DR, O’Shaughnessy C, Caputo RP,
Kereiakes DJ, Williams DO, Teirstein PS, Jaeger JL, Kuntz RE (2003) Sirolimus-eluting stents
versus standard stents in patients with stenosis in a native coronary artery. N Engl J Med
349:1315–1323
Muzzarelli R, Tarsi R, Filippini O, Giovanetti E, Biagini G, Varaldo PE (1990) Antimicrobial
properties of N-carboxybutyl chitosan. Antimicrob Agents Chemother 34:2019–2023
Nguyen KT, Su SH, Zilberman M, Bohluli P, Frenkel P, Tang L, Eberhart RC (2004) Biomaterials
and stent technology. In: Yaszemski M, Rantolo D, Lewandrowski KU, Hasirci V, Altobelli D,
Wise D (eds) Tissue engineering and novel delivery systems. Marcel Dekker, New York,
pp 107–130
Ormiston JA, Serruys PW, Regar E, Dudek D, Thuesen L, Webster MW, Onuma Y, Garcia-Garcia
HM, McGreevy R, Veldhof S (2008) A bioabsorbable everolimus-eluting coronary stent
system for patients with single de-novo coronary artery lesions (ABSORB): a prospective
open-label trial. Lancet 371:899–907
Ostojik M, Sagic D, Beleslin B, Jung R, Perisic Z, Jagic N, Nedeljkovic M, Mangovski L,
Milosavljevic B, Stojkovic S, Orlic D, Antonic Z, Miloradovic V, Topic D, Paunovic D
(2008) First clinical comparison of Nobori-Biolimus A9 eluting stents with Cypher-Sirolimus
eluting stents: NOBORI CORE nine months angiographic and one year clinical outcomes.
Euro Intervention 3:574–579
Park SN, Kim JK, Suh H (2004) Evaluation of antibiotic-loaded collagen-hyaluronic acid matrix
as a skin substitute. Biomaterials 25:3689–3698
Peterson L (2004) PARIS COURSE ON REVASCULARIZATION (PCR) Trends-in-Medicine.
Stephen Snyder, Paris, France
Planer D, Beyar R, Almagor Y, Banai S, Guetta V, Miller H, Kornowski R, Brandes S, Krakover
R, Solomon M, Lotan C (2008) Long-term (>3 Years) outcome and predictors of clinical
events after insertion of sirolimus-eluting stent in one or more native coronary arteries (from
the Israeli arm of the e-Cypher registry). Am J Cardiol 101:953–959
Popma JJ (2007) Stent Design, Materials, Polymers and Drugs for DES
�338
M. Zilberman et al.
Prabu P, Dharmaraj N, Aryal S, Lee BM, Ramesh V, Kim HY (2006) Preparation and drug release
activity of scaffolds containing collagen and poly(caprolactone). J Biomed Mater Res A
79:153–158
Price JS, Tencer AF, Arm DM, Bohach GA (1996) Controlled release of antibiotics from coated
orthopedic implants. J Biomed Mater Res 30:281–286
Pruitt BA Jr, Levine NS (1984) Characteristics and uses of biologic dressings and skin substitutes.
Arch Surg 119:312–322
Radu FA, Bause M, Knabner P, Lee GW, Friess WC (2002) Modeling of drug release from
collagen matrices. J Pharm Sci 91:964–972
Rao SV, Califf RM, Kramer JM, Peterson ED, Gross TP, Pepine CJ, Williams DO, Donohoe D,
Waksman R, Mehran R, Krucoff MW (2008) Postmarket evaluation of breakthrough technologies. Am Heart J 156:201–208
Rao SV, Shaw RE, Brindis RG, Klein LW, Weintraub WS, Peterson ED (2006) On- versus
off-label use of drug-eluting coronary stents in clinical practice (report from the American
College of Cardiology National Cardiovascular Data Registry [NCDR]). Am J Cardiol
97:1478–1481
REVA Medical I (2007) REVA Medical Announces Enrollment of First Patients in the RESORB
Clinical Trial
Revathi G, Puri J, Jain BK (1998) Bacteriology of burns. Burns 24:347–349
Ribichini F, Tomai F, Paloscia L, Di Sciascio G, Carosio G, Romano M, Verna E, Galli M,
Tamburino C, De Cesare N, Pirisi R, Piscione F, Lanteri G, Ferrero V, Vassanelli C (2007)
Steroid-eluting stents in patients with acute coronary syndrome: the dexamethasone eluting
stent Italian registry. Heart 93:598–600
Roenigk RK, Roenigk HH (1989) Dermatologic surgery: principles and practice. M. Dekker,
New York
Rogers CD (2004) Optimal stent design for drug delivery. Rev Cardiovasc Med 5(Suppl 2):
S9–S15
Rossi S, Marciello M, Sandri G, Ferrari F, Bonferoni MC, Papetti A, Caramella C, Dacarro C,
Grisoli P (2007) Wound dressings based on chitosans and hyaluronic acid for the release of
chlorhexidine diacetate in skin ulcer therapy. Pharm Dev Technol 12:415–422
Roy P, Bonello L, de Labriolle A, Okabe T, Pinto Slottow TL, Steinberg DH, Torguson R,
Smith K, Xue Z, Satler LF, Kent KM, Suddath WO, Pichard AD, Waksman R (2008) Twoyear outcome of patients treated with sirolimus- versus paclitaxel-eluting stents in an unselected population with coronary artery disease (from the REWARDS Registry). Am J Cardiol
102:292–297
Ruszczak Z, Friess W (2003) Collagen as a carrier for on-site delivery of antibacterial drugs. Adv
Drug Deliv Rev 55:1679–1698
Saito Y, Minami K, Kobayashi M, Nakao Y, Omiya H, Imamura H, Sakaida N, Okamura A (2002)
New tubular bioabsorbable knitted airway stent: biocompatibility and mechanical strength.
J Thorac Cardiovasc Surg 123:161–167
Salam AM, Al Suwaidi J, Holmes DR Jr (2006) Drug-eluting coronary stents. Curr Probl Cardiol
31:8–119
Schampaert E, Cohen EA, Schluter M, Reeves F, Traboulsi M, Title LM, Kuntz RE, Popma JJ
(2004) The Canadian study of the sirolimus-eluting stent in the treatment of patients with
long de novo lesions in small native coronary arteries (C-SIRIUS). J Am Coll Cardiol
43:1110–1115
Schofer J, Schluter M, Gershlick AH, Wijns W, Garcia E, Schampaert E, Breithardt G (2003)
Sirolimus-eluting stents for treatment of patients with long atherosclerotic lesions in
small coronary arteries: double-blind, randomised controlled trial (E-SIRIUS). Lancet
362:1093–1099
Serruys P (2005) Randomized comparison of a durable polymer everolimus-eluting stent with a
bare metal coronary stent: the SPIRIT first trial. Eur Heart J 1:58–65
�Drug-Eluting Medical Implants
339
Serruys P (2006) Randomized comparison of an everolimus eluting coronary stent with a paclitaxel eluting coronary stent: the SPIRIT II trial. Eur Heart J 2:286–294
Serruys PW, de Jaegere P, Kiemeneij F, Macaya C, Rutsch W, Heyndrickx G, Emanuelsson H,
Marco J, Legrand V, Materne P, Belardi J, Sigwart U, Colombo A, Goy JJ, van den Heuvel P,
Delcan J, Morel MA (1994) A comparison of balloon-expandable-stent implantation with
balloon angioplasty in patients with coronary artery disease. Benestent Study Group. N Engl
J Med 331:489–495
Serruys PW, Sianos G, Abizaid A, Aoki J, den Heijer P, Bonnier H, Smits P, McClean D, Verheye
S, Belardi J, Condado J, Pieper M, Gambone L, Bressers M, Symons J, Sousa E, Litvack F
(2005) The effect of variable dose and release kinetics on neointimal hyperplasia using a novel
paclitaxel-eluting stent platform: the Paclitaxel In-Stent Controlled Elution Study (PISCES).
J Am Coll Cardiol 46:253–260
Shanmugasundaram N, Sundaraseelan J, Uma S, Selvaraj D, Babu M (2006) Design and delivery
of silver sulfadiazine from alginate microspheres-impregnated collagen scaffold. J Biomed
Mater Res B Appl Biomater 77:378–388
Sousa JE, Serruys PW, Costa MA (2003a) New frontiers in cardiology: drug-eluting stents: part I.
Circulation 107:2274–2279
Sousa JE, Serruys PW, Costa MA (2003b) New frontiers in cardiology: drug-eluting stents: part II.
Circulation 107:2383–2389
Springer BD, Lee GC, Osmon D, Haidukewych GJ, Hanssen AD, Jacofsky DJ (2004) Systemic
safety of high-dose antibiotic-loaded cement spacers after resection of an infected total knee
arthroplasty. Clin Orthop Relat Res 427:47–51
Sripriya R, Kumar MS, Sehgal PK (2004) Improved collagen bilayer dressing for the controlled
release of drugs. J Biomed Mater Res B Appl Biomater 70:389–396
Stack RS, Califf RM, Phillips HR, Pryor DB, Quigley PJ, Bauman RP, Tcheng JE, Greenfield JC Jr
(1988) Interventional cardiac catheterization at Duke Medical Center. Am J Cardiol 62:3F–24F
Stella PR et al (2008) One year results of a new in situ length-adjustable stent platform with a biodegradable biolimus A9 eluting polymer: results of the CUSTOM-II trial. Eur Heart J 4(2):200–207
Stone GW, Ellis SG, Cox DA, Hermiller J, O’Shaughnessy C, Mann JT, Turco M, Caputo R,
Bergin P, Greenberg J, Popma JJ, Russell ME (2004) One-year clinical results with the slowrelease, polymer-based, paclitaxel-eluting TAXUS stent: the TAXUS-IV trial. Circulation
109:1942–1947
Stone GW, Midei M, Newman W, Sanz M, Hermiller JB, Williams J, Farhat N, Mahaffey KW,
Cutlip DE, Fitzgerald PJ, Sood P, Su X, Lansky AJ (2008) Comparison of an everolimuseluting stent and a paclitaxel-eluting stent in patients with coronary artery disease: a randomized trial. J Am Med Assoc 299:1903–1913
Sussman C, Bates-Jensen BM (2001) Wound care: a collaborative practice manual for physical
therapists and nurses, 2nd edn. Aspen Publishers, Gaithersburg, Md
Suzuki Y, Tanihara M, Nishimura Y, Suzuki K, Kakimaru Y, Shimizu Y (1997) A novel
wound dressing with an antibiotic delivery system stimulated by microbial infection. Asaio J
43:M854–M857
Suzuki Y, Tanihara M, Nishimura Y, Suzuki K, Kakimaru Y, Shimizu Y (1998) A new drug
delivery system with controlled release of antibiotic only in the presence of infection. J Biomed
Mater Res 42:112–116
Taddeucci P, Pianigiani E, Colletta V, Torasso F, Andreassi L, Andreassi A (2004) An evaluation
of Hyalofill-F plus compression bandaging in the treatment of chronic venous ulcers. J Wound
Care 13:202–204
Tamai H, Igaki K, Tsuji T (1999) A biodegradable poly-L-lactic acid coronary stent in porcine
coronary artery. J Intervent Cardiol 12:443–449
Tamai H, Igaki K, Kyo E, Kosuga K, Kawashima A, Matsui S, Komori H, Tsuji T, Motohara S,
Uehata H (2000) Initial and 6-month results of biodegradable poly-l-lactic acid coronary stents
in humans. Circulation 102:399–404
�340
M. Zilberman et al.
Tanabe K, Serruys PW, Grube E, Smits PC, Selbach G, van der Giessen WJ, Staberock M,
de Feyter P, Muller R, Regar E, Degertekin M, Ligthart JM, Disco C, Backx B, Russell ME
(2003) TAXUS III Trial: in-stent restenosis treated with stent-based delivery of paclitaxel
incorporated in a slow-release polymer formulation. Circulation 107:559–564
Tepe G, Wendel HP, Khorchidi S, Schmehl J, Wiskirchen J, Pusich B, Claussen CD, Duda SH
(2002) Thrombogenicity of various endovascular stent types: an in vitro evaluation. J Vasc
Interv Radiol 13:1029–1035
Trafny EA, Kowalska K, Grzybowski J (1998) Adhesion of Pseudomonas aeruginosa to collagen
biomaterials: effect of amikacin and ciprofloxacin on the colonization and survival of the
adherent organisms. J Biomed Mater Res 41:593–599
Trop M (2006) Silver-coated dressing acticoat caused raised liver enzymes and argyria-like
symptoms in burn patient. J Trauma 61:1024
Tsuchiya Y, Lansky AJ, Costa RA, Mehran R, Pietras C, Shimada Y, Sonoda S, Cristea E,
Negoita M, Dangas GD, Moses JW, Leon MB, Fitzgerald PJ, Muller R, Storger H, Hauptmann
KE, Grube E (2006) Effect of everolimus-eluting stents in different vessel sizes (from the
pooled FUTURE I and II trials). Am J Cardiol 98:464–469
Turco MA, Ormiston JA, Popma JJ, Mandinov L, O’Shaughnessy CD, Mann T, McGarry TF, Wu
CJ, Chan C, Webster MW, Hall JJ, Mishkel GJ, Cannon LA, Baim DS, Koglin J (2007)
Polymer-based, paclitaxel-eluting TAXUS Liberte stent in de novo lesions: the pivotal
TAXUS ATLAS trial. J Am Coll Cardiol 49:1676–1683
Urban P, Gershlick AH, Guagliumi G, Guyon P, Lotan C, Schofer J, Seth A, Sousa JE, Wijns W,
Berge C, Deme M, Stoll HP (2006) Safety of coronary sirolimus-eluting stents in daily clinical
practice: 1-year follow-up of the e-Cypher registry. Circulation 113:1434–1441
Uurto I et al (2005) Drug-eluting biodegradable poly-D/L-lactic acid vascular stents: an experimental pilot study. J Endovasc Ther 12(3):371–379
Varghese MC, Balin AK, Carter DM, Caldwell D (1986) Local environment of chronic wounds
under synthetic dressings. Arch Dermatol 122:52–57
Venkatraman S, Boey F (2007) Release profiles in drug-eluting stents: issues and uncertainties.
J Control Release 120:149–160
Virmani R, Guagliumi G, Farb A, Musumeci G, Grieco N, Motta T, Mihalcsik L, Tespili M,
Valsecchi O, Kolodgie FD (2004) Localized hypersensitivity and late coronary thrombosis
secondary to a sirolimus-eluting stent: should we be cautious? Circulation 109:701–705
Vogt F et al (2004) Long-term assessment of a novel biodegradable paclitaxel-eluting coronary
polylactide stent. Eur Heart J 25:1330–1340
Vranckx P, Serruys PW, Gambhir S, Eduardo SJ, Abizaid A, Lemos P, Ribeiro E, Dani SI,
Dalal JJ, Mehan V, Dhar A, Dutta AL, Reddy KN, Chand R, Ray A (2006) Biodegradablepolymer-based, paclitaxel-eluting InfinniumTM stent: 9-month clinical and angiographic follow-up results from the SIMPLE II prospective multi-centre registry study. Euro Intervention
2:310–317
Waksman R (2006) Update on bioabsorbable stents: from bench to clinical. J Interv Cardiol
19:414–421
Wang X, Venkatraman SS, Boey FY, Loo JS, Tan LP (2006) Controlled release of sirolimus from
a multilayered PLGA stent matrix. Biomaterials 27:5588–5595
Wei G, Jin Q, Giannobile WV, Ma PX (2006) Nano-fibrous scaffold for controlled delivery of
recombinant human PDGF-BB. J Control Release 112:103–110
Whang K, Thomas CH, Healy KE and Nuber G. (1995) A novel method to fabricate bioabsorbable
scaffolds. Polymer 36:837–842
Whang K, Tsai DC, Nam EK, Aitken M, Sprague SM, Patel PK and Healy KE (1998) Ectopic bone
formation via rhBMP-2 delivery from porous bioabsorbable polymer scaffolds. J Biomed Mat
Res 42:491–499
Windecker S, Serruys PW, Wandel S, Buszman P, Trznadel S, Linke A, Lenk K, Ischinger T,
Klauss V, Eberli F, Corti R, Wijns W, Morice MC, di Mario C, Davies S, van Geuns RJ,
Eerdmans P, van Es GA, Meier B, Juni P (2008) Biolimus-eluting stent with biodegradable
�Drug-Eluting Medical Implants
341
polymer versus sirolimus-eluting stent with durable polymer for coronary revascularisation
(LEADERS): a randomised non-inferiority trial. Lancet 372:1163–1173
Woods TC, Marks AR (2004) Drug-eluting stents. Annu Rev Med 55:169–178
Wu P, Grainger DW (2006) Drug/device combinations for local drug therapies and infection
prophylaxis. Biomaterials 27:2450–2467
Xu RX, Sun X, Weeks BS (2004) Burns regenerative medicine and therapy. Karger, Basel
Yamawaki T et al (1998) Intramural delivery of a specific tyrosine kinase inhibitor with biodegradable stent suppresses the restenotic changes of the coronary artery in pigs in vivo. J Am
Coll Cardiol 32:780–786
Ye YW et al (1998) Bioresorbable microporous stents deliver recombinant adenovirus gene
transfer vectors to the arterial wall. Ann Biomed Eng 26:398–408
Zalavras CG, Patzakis MJ, Holtom P (2004) Local antibiotic therapy in the treatment of open
fractures and osteomyelitis. Clin Orthop Relat Res 427:86–93
Zhu XH, Wang CH, Tong YW (2008) In vitro characterization of hepatocyte growth factor release
from PHBV/PLGA microsphere scaffold. J Biomed Mater Res A 89(2):411–423
Zidar J, Lincoff A, Stack R (1999) Biodegradable stents. In: Topol EJ (ed) Textbook of interventional cardiology, 3rd edn. WB Saunders, Philadelphia, pp 787–802
Zilberman M, Golerkansky E, Elsner JJ, Berdicevsky I (2009) Gentamicin-eluting bioresorbable
composite fibers for wound healing applications. J Biomed Mater Res A 89:654–666
Zilberman M, Schwade ND, Eberhart RC (2004) Protein-loaded bioresorbable fibers and expandable stents: mechanical properties and protein release. J Biomed Mater Res B Appl Biomater
69:1–10
View publication stats
�
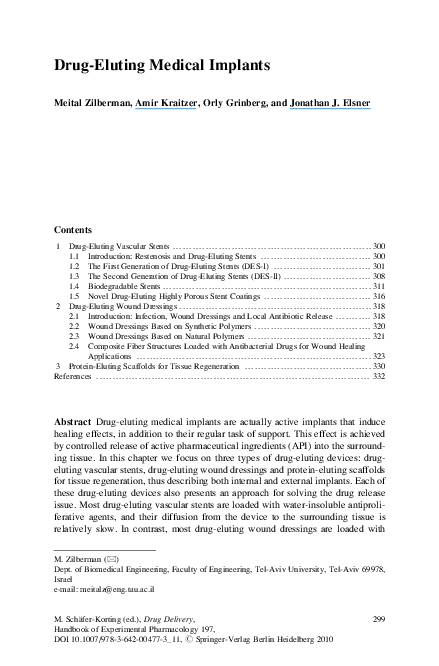
 Orly Grinberg
Orly Grinberg