Srinivasan, J Clin Cell Immunol 2013, S13
http://dx.doi.org/10.4172/2155-9899.S13-007
Clinical & Cellular
Immunology
Research
Article
Review Article
Open
OpenAccess
Access
The Role of Inflammatory Cytokines and the RANKL-RANK-OPG
Molecular Triad in Periodontal Bone Loss-A Review
Prathiba Chichurakanahalli Srinivasan*
SV Dental Collge, Bangalore, Karnataka, India
Abstract
Periodontal diseases are chronic inlammatory disorders involving the supporting structures of the teeth.
Connective tissue destruction and loss of bone support of the dentition are key features of this disease. Early
studies have revealed that bioilm plaque accumulation in the dentogingival area is the primary etiological factor
of periodontal diseases. Recent research has not only reinforced the bacterial etiology of periodontal disease, but
has also emphasized the role of inlammation in this pathologic process. The host mounts an immune-inlammatory
response to combat the bacterial attack. The host response is like a double-edged sword. It eliminates the offending
pathogens, but overstimulation and ampliication of the same leads to tissue destruction and bone loss. In the mid1990s, extensive research in the ield of bone biology led to the discovery of the RANKL-RANK-OPG molecular
triad. This article explores the mechanisms by which inlammatory host response leads to alveolar bone loss-the role
of cytokines, factors that stimulate osteoclastogenesis via the RANKL-RANK-OPG pathway and how inlammation
interferes with the uncoupling of bone formation and bone resorption. In addition to the conventional therapeutic
modalities aimed at eliminating the microbes, additional therapeutic strategies that interfere with the RANKL-RANKOPG axis may have a protective effect on the bone loss.
Keywords: Inlammation; RANKL; OPG; RANK; Osteoclastogenesis;
Cytokines; Periodontal disease; IL-1; TNF; Alveolar bone loss
Introduction
Periodontal diseases, which are chronic inlammatory disorders
localized to the attachment structures of the teeth, are considered to
be the major cause of tooth loss in adults and the most prevalent form
of bone pathology in humans [1]. he term periodontal disease refers
to both gingivitis and periodontitis. Gingivitis is an inlammatory
condition of the sot tissues surrounding the teeth [2]. If unchecked,
gingivitis progresses to periodontitis, an inlammation of the supporting
structures of the teeth [3]. Speciic gram-negative anaerobic bacteria
species such as Porphyromonas gingivialis and Tannerella forsythia
have been associated with periodontitis [4].
he initial host response to bacterial infection is a local
inlammatory reaction that activates the innate immune system [5].
An imbalance between the plaque bioilm and the host immune system
results in the overexpression of an array of proinlammatory cytokines,
propagation of inlammation through the gingival tissues and the
subsequent destruction of alveolar bone [6].
hus the inlammatory process results in destruction of connective
tissue and alveolar bone, the hallmarks of periodontal disease.
he Role of Inlammation in Alveolar Bone Loss
here are two critical factors, which dictate whether bone loss
occurs in response to inlammatory reaction.
1. he concentration of pro-inlammatory cytokines and mediators
present in the gingival tissue must be suicient to activate the pathways
leading to bone resorption.
2. he inlammatory mediators must penetrate the gingival tissue to
reach within a critical distance to alveolar bone [5].
Page and Schroeder showed that bone resorption ceases when a 2.5
mm zone is created between the site of bacteria and bone [7].
J Clin Cell Immunol
Inlammatory Mediators
here are several classes of molecules that activate a host response
which in turn stimulates osteoclastogenesis either directly or indirectly
[8]. hese include lipid-based molecules such as prostaglandins,
leukotrienes [8], pro-inlammatory cytokines such as IL-1, IL-6, IL-11
and IL-17, tumor necrosis factor-alpha, leukemia inhibitory factor, and
oncostatin M. he kinins such as bradykinin, kallidin and thrombin
and various chemokines can also lead to bone resorption [9].
Chemokines are chemotactic cytokines that stimulate recruitment
of inlammatory cells. Based on the structure of their ligand, they are
divided into two major families-CC and CXC. heir receptors are
referred to as CC chemokine receptor (CCR) and CXC chemokine
receptor (CXCR). CXCR2 receptor binds several chemokines that are
neutrophil chemoattractants [10]. Neutrophil recruitment is important
to protect against bacterial attack. Yu JJ et al. conducted a study in
which oral gavage of Porphyromonas gingivalis was administered
to CXCR2-and IL-17-deicient mice. he results revealed increased
periodontal bone loss in these mice compared to wild-type mice,
suggesting that chemokines and IL-17 are important in protecting host
against pathogen-initiated bone loss. IL-17 is a key cytokine produced
by a newly identiied subset of T helper cells (h) called the “h17”
lymphocytes and it is important in stimulating chemokine production
to recruit neutrophils. he enhanced bone loss observed in this study
is the result of a defective ability to stimulate neutrophil migration to
the inlamed bone, which requires IL-17 receptor dependant signals,
*Corresponding author: Prathiba Chichurakanahalli Srinivasan, SV Dental
Collge, Bangalore, Karnataka, India, E-mail: csprati@yahoo.com
Received June 13, 2013; Accepted August 27, 2013; Published August 31, 2013
Citation: Srinivasan PC (2013) The Role of Inlammatory Cytokines and the
RANKL-RANK-OPG Molecular Triad in Periodontal Bone Loss-A Review. J Clin
Cell Immunol S13: 007. doi:10.4172/2155-9899.S13-007
Copyright: © 2013 Srinivasan PC. This is an open-access article distributed under
the terms of the Creative Commons Attribution License, which permits unrestricted
use, distribution, and reproduction in any medium, provided the original author and
source are credited.
Innate Response to Infectious
Diseases
ISSN:2155-9899 JCCI, an open access journal
�Citation: Srinivasan PC (2013) The Role of Inlammatory Cytokines and the RANKL-RANK-OPG Molecular Triad in Periodontal Bone Loss-A Review.
J Clin Cell Immunol S13: 007. doi:10.4172/2155-9899.S13-007
Page 2 of 8
thus underscoring the importance of IL-17 in the defense against
oral pathogens [11]. From their study Zhang et al. concluded that IL17A produced by h17 cells stimulate the development of osteoclasts
(osteoclastogenesis) in the presence of osteoblasts [12] and Cardoso
et al. observed expression of IL-17 in gingiva from patients with
periodontitis [13].
he role of pro-inlammatory cytokines, interleukin-1 (IL1) and tumor necrosis factor (TNF) in bacteria-induced bone
loss was demonstrated in an animal model study by Assuma et al.
Porphyromonas gingivalis (Pg)-soaked silk ligatures were applied to the
posterior mandibular teeth of Macaca fascicularis primates to induce
experimental periodontitis. he primates received local injections,
over a period of 6 weeks, of antagonists to TNF-alpha and IL-1
(soluble TNF-alpha and IL-1 receptors) or vehicle control. he gingival
connective tissue sections in close proximity to bone demonstrated
signiicant inlammatory cell recruitment and osteoclast formation
surrounding bone in the control primates. hus, infection with Pg
in these animals was associated with expansion of the inlammatory
front to alveolar bone. he antagonists to cytokines reduced the
appearance of inlammatory cells in this region and the formation of
bone resorbing osteoclasts. hus, inhibition of inlammatory mediators
can prevent the “inlammatory front” from reaching the alveolar bone
leading to a reduction in bone loss as observed in this animal model
[14]. In a follow-up study with the same model Delima et al. in 2001,
stated that IL-1 and TNF blockers inhibited the loss of connective tissue
attachment [15].
In their study, Graves DT et al. concluded that P. gingivalis
induced osteoclastogenesis was reduced in TNF receptor-deicient
mice compared to wild-type controls, thus indicating that osteoclast
formation resulted from stimulation of the host response rather that
from the direct efect of bacterial products [16]. Gaspersic et al in rat
ligature model study concluded that the administration of recombinant
human TNF-alpha (rhTNF-alpha) accelerated the progression of
periodontitis [17]. In a study by Garlet et al. TNF-alpha receptor-1knockout mice developed signiicantly less inlammation and alveolar
bone loss in response to Aggregibacter actinomycetemcomitans oral
gavage. he levels of the pathogen as quantiied by real-time PCR was
higher in the TNF receptor ablated mice, compared to the wild-type
controls. he quantitative mRNA expression of inlammatory cytokines
IL-1 beta, interferon-gamma, and receptor activator of nuclear
factor-kappa B ligand (RANKL) was signiicantly lower in the TNF
receptor ablated mice. hus, the absence of TNFR-1 resulted in lower
production of cytokines in response to the pathogen. Decrease in TNFalpha seemed to reduce the host response, thereby leading to higher
levels of bacteria. However, there was reduced expression of cytokines
that stimulate bone resorption, which resulted in less net bone loss
[18]. In response to P. gingivalis oral gavage, mice with genetically
deleted IL-6 had decreased bone loss compared to wild-type mice,
thus indicating the pro-inlammatory efects of IL-6 leading to bone
resorption. (Baker PJ et al.) [19]. Li et al. examined the role of B and
CD4 T cells in adaptive immunity of rats infected with Aggregatibacter
actinomycetemcomitans (Aa). Sprague-Dawley male rats were fed
Aa-containing mash or control-mash for 2 weeks. B and CD4 T cells
were obtained from draining lymph nodes at 2, 4 and 12 weeks, post
inoculation. Quantitative polymerase chain reaction-based messenger
RNA expression was conducted for 89 cytokine family genes. B and CD4
T cells of Aa-infected rats increased and were activated, resulting in
enhanced isotype-switched serum immunoglobulin G by 2 weeks post
inoculation. Bone resorption was evident 12 weeks ater Aa-feeding. In
B cells, interleukin-2 (IL-2), macrophage-inhibiting factor, IL-19, ILJ Clin Cell Immunol
21, tumor necrosis factor (TNF), CD40 ligand (CD40L), CD70, bone
morphogenetic protein 2 (BMP2), BMP3, and BMP10 were upregulated
early; while IL-7, Fas ligand (FasL), small inducible cytokine subfamily
E1, and growth diferentiation factor 11 (GDF11; BMP11) were
upregulated late (12 weeks). BMP10 was sustained throughout. In CD4
T cells, IL-10, IL-16, TNF, lymphotoxin-beta (LTβ), APRIL, CD40L,
FasL, RANKL and osteoprotegerin were upregulated early, whereas IL1β, IL-1RN, IL-1F8, IL-24, interferon-α1, GDF11 (BMP11), and GDF15
were upregulated late (12 weeks). here was upregulation in mRNA for
a number of cytokines not normally ascribed to periodontal disease.
IL-16 was upregulated in CD4 T cells in the early phase of the response
[20]. IL-16 has been shown to be involved in the selective migration of
CD4 T cells, and participates in inlammatory diseases [21]. IL-19, a
novel cytokine of the IL-10 family, was also upregulated in CD4 T cells
in response to Aa [20]. IL-19 produced by synovial cell in Rheumatoid
arthritis (RA) patients promotes joint inlammation (Sakurai et al.)
[22]. IL-21, which has recently been shown to induce receptor activator
of nuclear factor kappaB ligand (RANKL) and was implicated in
arthritis (Jang et al.) [23] was upregulated in B cells responding to
Aa [20]. By 12 weeks, there was also an induction of IL-24 in CD4 T
cells responding to Aa [20]. IL-24 was increased in the synovium of
patients with rheumatoid arthritis, and this cytokine was implicated in
recruitment of neutrophil granulocytes (Kragstrup et al.) [24]. B cellactivating-factor (BAFF, or TNFSF13B) and a proliferation-inducing
ligand (APRIL), members of the TNF family, were upregulated in B cells
and CD4 T cells, respectively, in response to Aa infection [20]. IL-23,
a proinlammatory cytokine composed of IL-23p19 and IL-12/23p40
subunits, is known to promote the diferentiation of h17 cells. Studies
showed that IL-23 and IL-12 were expressed at signiicantly higher
levels in periodontal lesions than in control sites, suggesting that IL23-induced h17 pathway is stimulated in inlammatory periodontal
lesions (Ohyama et al.) [25]. IL-33 is a new member of the IL-1 family,
which plays a role in inlammatory response. Injecting IL-33 or IL-33R
agonistic antibody into TNF transgenic mice overexpressing human
TNF inhibited the development of spontaneous joint inlammation
and cartilage destruction. In vitro, IL-33 directly inhibits mouse and
human M-CSF/receptor activator for NF-kβ ligand-driven osteoclast
diferentiation, suggesting an important role for IL-33 as a boneprotecting cytokine with potential for treating bone resorption (Zaiss
et al.) [26]. he bone resorption protein RANKL and its soluble decoy
receptor OPG was also induced in the CD4 T cells of Aa-fed rats [20].
he role of bone morphogenetic proteins (BMPs) and growth
diferentiation factors (GDFs) in periodontal disease
Bone morphogenic proteins (BMPs) and growth diferentiation
factors (GDFs) are members of the transforming growth factor-β
(TGF-β) superfamily. hey play important roles during development
and organogenesis in delivering positional information in both
vertebrates and invertebrates, and are involved in the development of
hard as well as sot tissue (Herpin, Lelong and Favrel) [27]. BMP2 was
induced in B cells early (week 4) of the inlammatory process, at the
same time that RANKL was induced in CD4 T cells (Li et al.). his
suggests that bone repair mechanisms were induced early, well ahead of
impending bone resorption. However, by 12 weeks of infection by Aa,
BMP2 was shut down, as bone resorption proceeded. BMP3 was also
upregulated at week 4 in B cells responding to Aa [20]. BMP3 has been
shown to be a negative regulator in the skeleton, as mice lacking BMP3
have increased bone mass. Transgenic mice over-expressing BMP3
had altered endochondral bone formation resulting in spontaneous rib
fractures [28]. Both BMP2 and BMP3 were upregulated in B cells at the
Innate Response to Infectious
Diseases
ISSN:2155-9899 JCCI, an open access journal
�Citation: Srinivasan PC (2013) The Role of Inlammatory Cytokines and the RANKL-RANK-OPG Molecular Triad in Periodontal Bone Loss-A Review.
J Clin Cell Immunol S13: 007. doi:10.4172/2155-9899.S13-007
Page 3 of 8
same time (4 weeks post infection), and were shut down at 12 weeks, at
which time bone resorption was evident [20]. B cells responding to Aa
upregulated BMP10 at all time points [20]. BMP10 has been shown to
regulate myocardial hypertrophic growth (Chen et al. 2006) [29]. BMP10 may function as a tumor suppressor and apoptosis regulator for
prostate cancer [30]. hus the expression of BMP 10 in the Aa rat model
at all points suggests it’s role in inlammation and bone resorption
[20]. Also the involvement of BMP10 in cardiac hypertrophy [29] and
in prostate cancer [30] suggests a possible link between periodontal
disease and systemic diseases.
Discovery of OPG/RANKL/RANK Molecular Triad he Solving of the Puzzle
Growth diferentiation factor 11 (GDF11) or BMP11, plays an
important role in establishing embryonic axial skeletal patterns [31]. In
the GDF11 was upregulated at 12 weeks post infection, in both B and
CD4 T cells, at the time of bone resorption. his suggests that GDF11
may have a novel role in bone resorption [20].
In 1981, Rodan and Martin proposed a novel hypothesis wherein
the osteoblast played a central role in mediating the hormonal control
of osteoclastogenesis and bone resorption [37]. But, the factors
expressed by the osteoblast/stromal cells remained undetermined until
they were discovered independently by four groups using diferent
approaches. Boyle and coworkers at the Amgen Inc (housand Oaks,
CA, USA) discovered OPG serendipitously when they were attempting
to identify tumor necrosis factor receptor-related molecules with
possible therapeutic utility by generating transgenic mice that overexpress various TNF receptor related cDNAs. Mice over-expressing one
particular cDNA developed marked osteopetrosis because they did not
have osteoclasts in their bones. he protein encoded by the gene was
termed osteoprotegerin-OPG (the bone protector) [38].
he Aa-induced rat model, the Pg-induced mouse model and
several other animal studies discussed above strongly support the role
of pro-inlammatory cytokines in bone loss. he role of novel cytokines
not previously ascribed to periodontal disease has been extensively
discussed and these studies also suggest a possible link between
periodontal disease and systemic diseases.
Using the standard approach to test the Rodan-Martin hypothesis
of purifying a factor from human embryonic ibroblasts that inhibited
osteoclastogenesis, researchers at Snow Brand Milk Products Co.
(Sapporo, Hokkaido, Japan) reported their discovery of an identical
molecule. hey obtained a partial protein sequence and subsequently
cloned the cDNA for OPG [39].
Osteoimmunology
he discovery of OPG became the key to identify the long-sought
osteoclast diferentiation factor expressed on osteoblastic/stromal cell
that was essential for osteoclast development. Using expression cloning
and OPG as a probe, both the groups quickly identiied its ligand, which
they termed OPG ligand [40] and osteoclast diferentiation factor [41]
respectively. his ligand turned out to be identical to a member of the
TNF ligand family, which had been identiied in the preceding year as
RANKL [42] and TNF-related activation induced cytokine (TRANCE)
[43]. he cellular receptor was identiied as being identical to previously
identiied RANK, which Anderson and coworkers at Immunex (Seattle,
WA, USA) had discovered while they were sequencing cDNAs from
a human bone marrow derived myeloid dendritic cell cDNA library.
[42]. Both the groups found that RANK had partial homology to
a portion of the extracellular domain of human CD40, a member of
the TNF receptor superfamily, and it was involved in the activation
of T cells in the immune system. he groups then isolated RANKL by
direct expression screening and found, like Wong and coworkers [43]
did, that it increased dendritic cell stimulated naïve T cell proliferation
and survival of RANK-expressing T cells. hese discoveries led to the
conclusion that RANKL is involved in osteoclastogenesis and T cell
activation.
Extensive research in the ields of immunology and osteology
has revealed an intimate relationship between inlammation/the
immune system and the skeletal system [32].he immunoskeletal
interface involves centralization of the immune and skeletal functions
around common cells types and cytokine efectors that control the
physiological bone mass. Prolonged immune activation can lead to
skeletal deterioration. his interconnection of the skeletal and the
immune systems has spawned the emergence of a new ield of science
termed “osteoimmunology” [33]. he ield of osteoimmunology ofers
better insights into the understanding of pathogenesis of periodontal
disease by explaining the role of inlammation in alveolar bone loss.
Osteoclasts and the Receptor Activator of NF-Kappa
B (RANK)/RANK Ligand (RANKL)/Osteoprotegerin
(OPG) System
Osteoclasts are unique cells of the human body tasked with
resorbing bone. hese multinucleated giant cells bind down onto the
bone surfaces creating a sealing zone and a ruled-membrane border
into which apical proton pumps accumulate hydrogen ions that
combine with chloride ions to form hydrochloric acid, which degrades
bone mineral. he exposed collagen matrix is attacked by acid resistant
endosomal and lysosomal enzymes that cleave collagen ibers efectively
removing small quantities of bone [34].
How osteoclasts form, what regulates their diferentiation and
activity was an enigma. Research has revealed that osteoclast precursors
circulate amid the monocyte/macrophage population and diferentiate
into preosteoclasts that fuse and form giant bone resorbing mature
osteoclasts [35]. Inlammatory processes such as rheumatoid arthritis
and periodontal infection predispose to osteoclastic bone resorption
by production of pro-inlammatory cytokines such as IL-1 and TNFalpha [36]. he osteoclast however, does not possess receptors for the
cytokines or hormones. So, for years the biologists were perplexed
as to how they resorbed bone. his conundrum was solved with the
discovery of the osteoprotegerin (OPG), receptor activator of nuclear
factor-kappa B ligand (RANKL) and receptor activator of nuclear factor
kappa-B (RANK).
J Clin Cell Immunol
Osteoclast Formation/Osteoclastogenesis
Osteoclastogenesis is coordintated by the interaction of the three
members of the TNF superfamily-OPG/RANKL/RANK [44] RANKL is
expressed predominantly as a membrane-bound ligand on osteoblasts,
ibroblasts, and activated T and B cells and its osteoclastogenic action
can be blocked by its soluble decoy receptor osteoprotegerin (OPG)
[9,35]. Together with Macrophage-colony stimulating factor (mCSF),
RANKL is a key cytokine in the induction of osteoclastogeneis both
in vitro and in vivo [45]. It binds directly to RANK on the surface of
preosteoclasts and osteoclasts, stimulating both the diferentiation of
osteoclast progenitors and the activity of mature osteoclasts [40,46,47].
Regulation of Bone Remodeling - he Role of the
RANKL-RANK-OPG System
Systemic factors and local stimuli in the bone microenvironment
Innate Response to Infectious
Diseases
ISSN:2155-9899 JCCI, an open access journal
�Citation: Srinivasan PC (2013) The Role of Inlammatory Cytokines and the RANKL-RANK-OPG Molecular Triad in Periodontal Bone Loss-A Review.
J Clin Cell Immunol S13: 007. doi:10.4172/2155-9899.S13-007
Page 4 of 8
target the molecular interplay of RANKL-RANK-OPG cytokine system,
thus regulating the remodeling of alveolar bone. (Lerner 2; Boyle et al.
Mundy et al. Horowitz et al.) [48-51]. Systemic modulators include
calcitonin, parathyroid hormone, thyroid hormone, gonadal steroids,
vitamin D, glucocorticoids and growth hormone. Local mediators
include pro-inlammatory cytokines as well as prostanoids (Lerner)
[48]. Bacterial products may interfere with bone remodeling balance by
regulating RANKL expression (Lerner, Henderson and Nair) [48,52].
Gram-negative bacteria such as A. actinomycetemcomitans, (Teng et
al. Kikuchi et al. Teng et al. ) [53-55], P. gingivalis (Okahashi et al.)
[56], Treponema denticola (Choi et al.) [57] and Streptococcus pyogenes
(Okahashi et al. Sakurai et al.) [58,59] have been shown to upregulate
RANKL expression in a variety of cells.
RANKL-RANK-OPG in Periodontal Disease
Studies have revealed that during inlammatory response, cytokines,
chemokines and other mediators stimulate periosteal osteoblasts,
altering the expression levels of receptor activator of nuclear factorkappa B ligand (RANKL) on the osteoblast surface [9,49]. RANKL is
expressed by osteoblasts in the form of a membrane-bound protein
(mRANKL) or cleaved into a soluble form (sRANKL) [60,61]. IL-1
stimulates osteoclastogenesis and bone resorption, largely through
up-regulation of RANKL, while TNF can stimulate osteoclastogenesis
directly or indirectly through RANKL [62]. Inhibition of RANK ligand
caused a decrease in alveolar bone loss in several models of periodontal
disease (Teng et al. Han et al. Jin et al.) [55,63,64].
Teng et al. in their study demonstrated the role of CD4+ T cells in
mediating periodontal bone loss. Also, they found that administration
of RANK ligand inhibitor; osteoprotegerin reduced osteoclastogenesis
and inhibited alveolar bone destruction [55]. Han et al. in 2006
demonstrated that B cells contribute to periodontal bone loss in the
absence of T cells through production of RANKL [63].
Bone resorption and formation are regulated by the relative
concentrations of RANKL, RANKL receptor RANK on osteoclast
precursor cells and the soluble decoy receptor OPG. When RANKL
expression is enhanced relative to OPG, RANKL is available to bind to
RANK on osteoclast precursors, tipping the balance to favor activation of
osteoclast formation and bone resorption [49]. he binding of RANKL
to osteoclast precursors occurs at a stage when hematopoietic stem cells
have diferentiated from the colony forming unit for granulocytes and
macrophages to the colony forming unit for macrophages (CFU-M).
Binding of RANKL to RANK on CFU-M in the presence of macrophage
colony stimulating factor induces diferentiation of preosteoclast
into a multinucleated cell that becomes a mature osteoclast, which
then resorbs bone [65]. When OPG concentrations are high relative
to RANKL expression, OPG binds RANKL, inhibiting it to bind to
RANK. Preventing the binding of RANKL to RANK leads to reduced
formation of osteoclasts and apoptosis of preexisting osteoclasts [49].
Jin et al. in 2007 conducted a study in which rats were administered
subcutaneously an OPG-Fc fusion protein to bloc RANK ligand.
Compared to the controls, reduced osteoclastogenesis and signiicant
preservation of the alveolar bone volume was observed in among
the OPG-Fc treated rats [64]. Leiwiecki in 2009 demonstrated that
treatment with Denosumab, a human monoclonal antibody speciic for
RANKL reduces the risk for fractures and increases the bone mineral
density in post-menopausal women. It also inhibits osteoclast-mediated
damage caused by rheumatoid arthritis [66].
he studies discussed above have provided valuable insights into the
role of inlammation or host response in the pathogenesis of periodontal
disease. he studies have unequivocally demonstrated that over
ampliication of the immune system releases a host of pro-inlammatory
cytokines and mediators that can lead to osteoclastogenesis. Also, these
inlammatory mediators can stimulate the release of RANK ligand and
thereby lead to bone resorption.
he Assessment of RANKL/OPG Ratio in the Severity
of Periodontitis
A number of clinical studies have investigated the concentrations
Study
Healthy
Gingivitis
Mild perio Moderate perio Chronic perio Generalized
Chronic with
Conclusion
subjects (n) subjects (n) subjects (n) subjects (n)
subjects (n) aggressive severe immunosuppressant
subjects (n)
subjects (n)
Bostanci et al. (GCF)
[68]
21
22
28
25
11
GCF RANKL &OPG were
oppositely regulated in
periodontitis groups.
Bostanci et al.
Gingival tissue [69]
9
8
11
12
10
RANKL/OPG ratio increased in
all periodontitis groups.
Lu et al. (GCF and
gingiva) [6]
4
20
Mogi et al. (GCF) [70] 28
27
GCF RANKL, but not OPG was
elevated in periodontitis groups.
58
47
RANKL/OPG ratio was
signiicantly elevated in
periodontitis groups.
27
25
RANKL/OPG was elevated in
periodontitis groups.
Liu et al. (Gingival
tissue) [71]
6
Kawai et al. (gingiva
and blood) [72]
12
32
sRANKL, but not OPG
was signiicantly higher in
periodontitis gropus.
Wara-aswapati et al.
(gingiva and plaque)
[73]
15
15
RANKL/OPG ratio was
signiicantly higher in
perioidontitis groups
Garlet et al. (gingival
tissue) [74]
10
Nagasawa et al.
(gingival tissue) [75]
2
7
20
16
RANKL/OPG and MMP/TIMP
expression determined disease
progression/severity
30
OPG is induced by LPSstimulated gingival ibroblast.
sRANKL: Soluble Receptor Activator of Nuclear Factor-Kappa B Ligand; TIMP: Tissue Inhibitors of Metalloproteinases; LPS: Lipopolysaccharides; perio: Periodontitis
Table 1: Summary of human studies evaluating the RANKL and OPG in Periodontal Disease.
J Clin Cell Immunol
Innate Response to Infectious
Diseases
ISSN:2155-9899 JCCI, an open access journal
�Citation: Srinivasan PC (2013) The Role of Inlammatory Cytokines and the RANKL-RANK-OPG Molecular Triad in Periodontal Bone Loss-A Review.
J Clin Cell Immunol S13: 007. doi:10.4172/2155-9899.S13-007
Page 5 of 8
of RANKL and OPG in the gingival crevicular luid of individuals
with periodontitis to determine the RANKL/OPG ratio. Table 1
summarizes the human studies evaluating the RANKL and OPG levels
in periodontal disease [67].
With a net increase in the ratio of RANKL/OPG in gingiva and
crevicular luid associated with bone loss and with the severity of
periodontal disease, the possibility of interference with the RANK/
RANKL/OPG axis may ofer novel therapeutic outcomes. he desired
outcome would be an increase in OPG or a decrease in RANKL that
brings the OPG/RANKL ratio to a balance where bone formation is
equal to bone resorption. A summary of animal studies in which
osteoprotegerin fusion protein (OPG-Fc) and other inhibitors of
RANK-mediated osteoclastogenesis are presented in Table 2 [67].
hus the inference from the above mentioned animal studies is,
therapeutic modalities which interfere with the RANK-RANKL-OPG
axis will have a protective efect on osteoclastogenesis and periodontal
bone loss.
Role of Cytokines in Bone Uncoupling
Bone is resorbed by osteoclasts, following which new bone is laid
down by osteoblasts in the resorption lacunae. Under physiologic
conditions, the two activities are coupled, i.e., the amount of bone
formed by osteoblasts is equal to that resorbed by osteoclasts. In
pathologic processes like periodontal disease and osteoporosis the two
processes are uncoupled i.e., there is deicient bone formation following
resorption [80].
he inlammatory process that leads to osteoclastogenesis and
bone resorption may also be responsible for the failure to form
adequate amount of new bone i.e., inlammation causes uncoupling
of bone formation following bone resorption [8]. Al-Masahat et al.
in 2006 and Liu et al. in 2006 stated that prolonged inlammation in
diabetic animals interferes with bone formation in the periodontium
following an episode of bone resorption. he prolonged inlammation
may stimulate the death of the osteoblasts [81,82]. Application of
cytokines like IL-1 beta and TNF-alpha in vivo not only stimulates bone
resorption but limits bone formation by inhibiting the coupling process
(Bertolini et al. Nyugen et al.) [83,84]. Osteoblast survival is a key
factor in bone formation. A study by Diarra and colleagues reported
that TNF-alpha stimulates production of Dickkopf-1 (DKK-1), which
suppresses bone formation by inhibiting the WNT (wingless WNT/
beta catenin) pathway. DKK-1, a negative regulator of WNT pathway
is up-regulated by TNF stimulation through TNF-1 receptor and P38
MAPK (mitogen-activating protein kinase) signaling. he up-regulated
DKK-1 not only promotes bone resorption but also blocks bone
Study Method
Study Method
Jin et al. [64]
Systemic delivery of rhOPG-Fc
Teng et al. [55]
Intraperitoneal injection of srOPG-Fc
Valverde et al. [76]
Subcutaneous kaliotoxin, K+-channel blocker T cells.
Kawai et al. [77]
Intraperitoneal injection of OPG-Fc
Mahamed et al. [78] Intraperitoneal injection of hu-OPG-Fc
Rogers et al. [79]
Oral gavage of SD282, a p38 MAPK inhibitor
Assuma et al. [14]
Intrapapillary injection of TNF-alpha and IL-1 antagonists.
rhOPG-Fc: Human recombinant osteoprotegerin fusion protein; MAPK: MitogenActivated Protein Kinase; SFRP1: Secreted Frizzled-related Protein 1; hOPGFc: Human Osteoprotegerin fusion protein; srOPG-Fc: soluble recombinant
Osteoprotegerin fusion protein; huOPG-Fc: human osteoprotegerin fusion protein;
SD282: an indole 5-carboxamide selective p38* MAPK inhibitor (Scois, Fremont,
CA). (David L Cochran)
Table 2: Summary of animal interventional trials of periodontal disease.
J Clin Cell Immunol
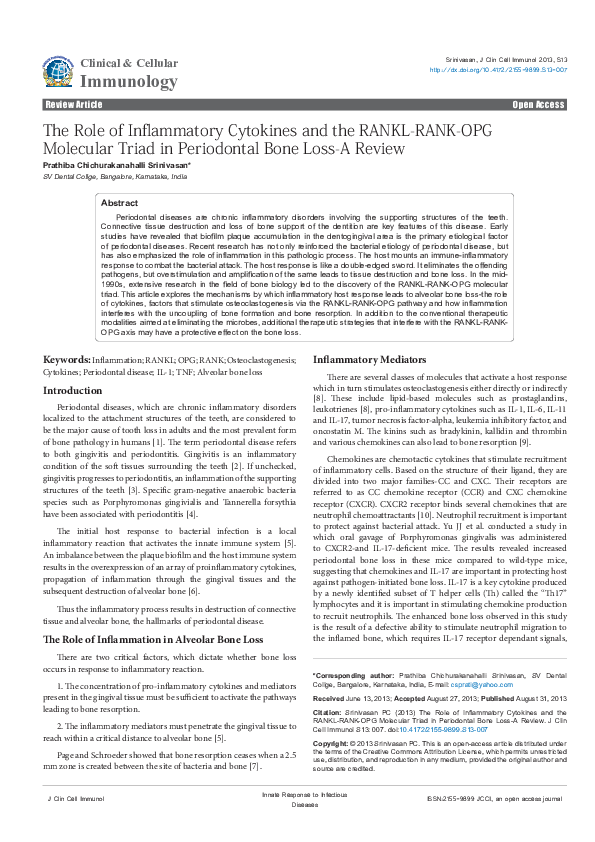
Figure 1: Schematic illustration depicting the role of inlammatory mediators
stimulating osteoclastogenesis and uncoupling of bone leading to alveolar
bone loss in periodontal disease.
formation and repair in the diseased joint [85]. hus, inlammatory
cytokines like TNF-alpha can limit bone formation by inhibiting
osteoblast diferentiation. In addition, the pro-inlammatory cytokines
may directly stimulate osteoblast or osteoblast precursor apoptosis or
indirectly afect it by stimulating expression of Fas, a potent apoptotic
mediator [86]. Periodontal ligament cells are an important source of
osteoblast precursors. TNF-alpha induced apoptosis of periodontal
ligament cells may afect the pool of osteoblast precursors [87]. Another
mechanism for uncoupling is the reduced function of osteoblasts
mediated by diminished production of bone matrix proteins. A study
by Centrella et al. in 1988 showed that TNF-alpha reduces collagen
production and alkaline phosphatase activity in cells obtained from
fetal rat parietal bone [88]. TNF-alpha and TNF-beta induce a twofold to three-fold reduction in synthesis of non-collagen bone matrix
proteins like osteocalcin by osteoblasts [89]. Eguchi et al. stated that
TNF speciic inhibitor, etanercept, promotes BMP-2 induced ectopic
bone formation when applied systemically or locally in vivo, thereby
improving the coupling process [90].
hus evidence from the literature has unequivocally established
the negative impact of the inlammatory process on bone coupling.
he net bone loss observed in periodontitis is due to the cumulative
efect of inlammation-induced bone loss and the uncoupling of bone
resorption and bone formation (Figure 1).
Innate Response to Infectious
Diseases
ISSN:2155-9899 JCCI, an open access journal
�Citation: Srinivasan PC (2013) The Role of Inlammatory Cytokines and the RANKL-RANK-OPG Molecular Triad in Periodontal Bone Loss-A Review.
J Clin Cell Immunol S13: 007. doi:10.4172/2155-9899.S13-007
Page 6 of 8
Conclusion
Periodontal diseases are chronic inlammatory disorders that
alict the supporting structures of the teeth. It is widely recognized
that bacteria initiate periodontal diseases. he host responds to this
bacterial attack by mounting an immuno-inlammatory response.
he host response is essential to ward of the bacterial attack and
prevent the systemic dissemination of infection. But in the process,
the inlammatory response can also cause tissue destruction and
alveolar bone loss. Prolonged inlammation and ampliication of the
inlammatory response releases a wide spectrum of pro-inlammatory
cytokines and mediators. he cytokines and pro-inlammatory
mediators propagate the inlammatory process and the “inlammatory
front” advances to the alveolar bone. Alveolar bone loss is the cardinal
sign of periodontitis. Experimental periodontitis studies have shown
that cytokines like IL-1 and TNF-alpha can lead to alveolar bone loss.
hese cytokines can also induce osteoclastogenesis via the RANKLRANK-OPG pathway. IL-1 and TNF-alpha also have a negative
impact on bone coupling. he net bone loss seen in periodontitis is
due to the cumulative efect of inlammation-induced bone loss and
the uncoupling of bone formation and bone resorption. his intricate
relationship between inlammation and bone metabolism has led to a
new ield of science termed “osteoimmunology.” Extensive research in
ield of bone biology has provided valuable insights into pathogenesis
of periodontal disease. Inlammation is now recognized as the central
component of periodontal disease. Better understanding of the disease
process will pave the way for adopting novel treatment approaches and
thereby improve clinical outcomes. herapeutic agents antagonistic to
the inlammatory mediators or agents which block RANK ligand may be
useful adjuncts to the conventional periodontal treatment procedures.
We are still at the tip of the iceberg and longitudinal human clinical
trials are required to prove the beneits of these therapeutic procedures.
References
1.
Papapanou PN (1999) Epidemiology of periodontal diseases: an update. J Int
Acad Periodontol 1: 110-116.
2.
Haimov-Kochman R, Kochman T, Stabholz A, Hochner-Celinkier D (2004)
Bisphosphonate and estrogen replacement therapy for postmenopausal
periodontitis. Isr Med Assoc J 6: 173-177.
3.
Buencamino MC, Palomo L, Thacker HL (2009) How menopause affects oral
health, and what we can do about it. Cleve Clin J Med 76: 467-475.
4.
Brennan RM, Genco RJ, Wilding GE, Hovey KM, Trevisan M, et al. (2007)
Bacterial species in subgingival plaque and oral bone loss in postmenopausal
women. J Periodontol 78: 1051-1061.
5.
Graves DT, Cochran D (2003) The contribution of interleukin-1 and tumor
necrosis factor to periodontal tissue destruction. J Periodontol 74: 391-401.
6.
Lu HK, Chen YL, Chang HC, Li CL, Kuo MY (2006) Identiication of the
osteoprotegerin/receptor activator of nuclear factor-kappa B ligand system
in gingival crevicular luid and tissue of patients with chronic periodontitis. J
Periodontal Res 41: 354-360.
7.
Page RC, Schroeder HE (1981) Current status of the host response in chronic
marginal periodontitis. J Periodontol 52: 477-491.
8.
Graves DT, Li J, Cochran DL (2011) Inlammation and uncoupling as
mechanisms of periodontal bone loss. J Dent Res 90: 143-153.
9.
Lerner UH (2006) Inlammation-induced bone remodeling in periodontal
disease and the inluence of post-menopausal osteoporosis. J Dent Res 85:
596-607.
10. Graves D (2008) Cytokines that promote periodontal tissue destruction. J
Periodontol 79: 1585-1591.
11. Yu JJ, Ruddy MJ, Wong GC, Sintescu C, Baker PJ, et al. (2007) An essential
role for IL-17 in preventing pathogen-initiated bone destruction: recruitment of
neutrophils to inlamed bone requires IL-17 receptor-dependent signals. Blood
109: 3794-3802.
J Clin Cell Immunol
12. Zhang F, Tanaka H, Kawato T, Kitami S, Nakai K, et al. (2011) Interleukin17A induces cathepsin K and MMP-9 expression in osteoclasts via celecoxibblocked prostaglandin E2 in osteoblasts. Biochimie 93: 296-305.
13. Cardoso CR, Garlet GP, Crippa GE, Rosa AL, Júnior WM, et al. (2009)
Evidence of the presence of T helper type 17 cells in chronic lesions of human
periodontal disease. Oral Microbiol Immunol 24: 1-6.
14. Assuma R, Oates T, Cochran D, Amar S, Graves DT (1998) IL-1 and TNF
antagonists inhibit the inlammatory response and bone loss in experimental
periodontitis. J Immunol 160: 403-409.
15. Delima AJ, Oates T, Assuma R, Schwartz Z, Cochran D, et al. (2001) Soluble
antagonists to interleukin-1 (IL-1) and tumor necrosis factor (TNF) inhibits loss
of tissue attachment in experimental periodontitis. J Clin Periodontol 28: 233240.
16. Graves DT, Oskoui M, Volejnikova S, Naguib G, Cai S, et al. (2001) Tumor
necrosis factor modulates ibroblast apoptosis, PMN recruitment, and
osteoclast formation in response to P. gingivalis infection. J Dent Res 80:
1875-1879.
17. Gaspersic R, Stiblar-Martincic D, Osredkar J, Skaleric U (2003) Inluence of
subcutaneous administration of recombinant TNF-alpha on ligature-induced
periodontitis in rats. J Periodontal Res 38: 198-203.
18. Garlet GP, Cardoso CR, Campanelli AP, Ferreira BR, Avila-Campos MJ,
et al. (2007) The dual role of p55 tumour necrosis factor-alpha receptor in
Actinobacillus actinomycetemcomitans-induced experimental periodontitis:
host protection and tissue destruction. Clin Exp Immunol 147: 128-138.
19. Baker PJ, Dixon M, Evans RT, Dufour L, Johnson E, et al. (1999) CD4(+) T
cells and the proinlammatory cytokines gamma interferon and interleukin-6
contribute to alveolar bone loss in mice. Infect Immun 67: 2804-2809.
20. Li Y, Messina C, Bendaoud M, Fine DH, Schreiner H, et al. (2010) Adaptive
immune response in osteoclastic bone resorption induced by orally
administered Aggregatibacter actinomycetemcomitans in a rat model of
periodontal disease. Mol Oral Microbiol 25: 275-292.
21. Akiyama K, Karaki M, Kobayshi R, Dobashi H, Ishida T, et al. (2009) IL-16
variability and modulation by antiallergic drugs in a murine experimental
allergic rhinitis model. Int Arch Allergy Immunol 149: 315-322.
22. Sakurai N, Kuroiwa T, Ikeuchi H, Hiramatsu N, Maeshima A, et al. (2008)
Expression of IL-19 and its receptors in RA: potential role for synovial
hyperplasia formation. Rheumatology (Oxford) 47: 815-820.
23. Jang E, Cho SH, Park H, Paik DJ, Kim JM, et al. (2009) A positive feedback
loop of IL-21 signaling provoked by homeostatic CD4+CD25- T cell expansion
is essential for the development of arthritis in autoimmune K/BxN mice. J
Immunol 182: 4649-4656.
24. Kragstrup TW, Otkjaer K, Holm C, Jørgensen A, Hokland M, et al. (2008) The
expression of IL-20 and IL-24 and their shared receptors are increased in
rheumatoid arthritis and spondyloarthropathy. Cytokine 41: 16-23.
25. Ohyama H, Kato-Kogoe N, Kuhara A, Nishimura F, Nakasho K, et al. (2009)
The involvement of IL-23 and the Th17 pathway in periodontitis. J Dent Res
88: 633-638.
26. Zaiss MM, Kurowska-Stolarska M, Böhm C, Gary R, Scholtysek C, et al. (2011)
IL-33 shifts the balance from osteoclast to alternatively activated macrophage
differentiation and protects from TNF-alpha-mediated bone loss. J Immunol
186: 6097-6105.
27. Herpin A, Lelong C, Favrel P (2004) Transforming growth factor-beta-related
proteins: an ancestral and widespread superfamily of cytokines in metazoans.
Dev Comp Immunol 28: 461-485.
28. Gamer LW, Cox K, Carlo JM, Rosen V (2009) Overexpression of BMP3 in
the developing skeleton alters endochondral bone formation resulting in
spontaneous rib fractures. Dev Dyn 238: 2374-2381.
29. Chen H, Yong W, Ren S, Shen W, He Y, et al. (2006) Overexpression of
bone morphogenetic protein 10 in myocardium disrupts cardiac postnatal
hypertrophic growth. J Biol Chem 281: 27481-27491.
30. Ye L, Kynaston H, Jiang WG (2009) Bone morphogenetic protein-10
suppresses the growth and aggressiveness of prostate cancer cells through a
Smad independent pathway. J Urol 181: 2749-2759.
31. McPherron AC, Lawler AM, Lee SJ (1999) Regulation of anterior/posterior
Innate Response to Infectious
Diseases
ISSN:2155-9899 JCCI, an open access journal
�Citation: Srinivasan PC (2013) The Role of Inlammatory Cytokines and the RANKL-RANK-OPG Molecular Triad in Periodontal Bone Loss-A Review.
J Clin Cell Immunol S13: 007. doi:10.4172/2155-9899.S13-007
Page 7 of 8
patterning of the axial skeleton by growth/differentiation factor 11. Nat Genet
22: 260-264.
52. Henderson B, Nair SP (2003) Hard labour: bacterial infection of the skeleton.
Trends Microbiol 11: 570-577.
32. Takayanagi H (2007) Osteoimmunology: shared mechanisms and crosstalk
between the immune and bone systems. Nat Rev Immunol 7: 292-304.
53. Teng YT (2002) Mixed periodontal Th1-Th2 cytokine proile in Actinobacillus
actinomycetemcomitans-speciic osteoprotegerin ligand (or RANK-L)mediated alveolar bone destruction in vivo. Infect Immun 70: 5269-5273.
33. Weitzmann MN (2013) The role of inlammatory cytokines, the RANKL/OPG
axis, and the immunoskeletal interface in physiological bone turnover and
osteoporosis. Scienctiica 2013: 125705.
34. Baron R, Neff L, Brown W, Louvard D, and Courtoy PJ (1990) Selective
internalization of the apical plasma membrane and rapid redistribution of
lysosomal enzymes and mannose 6-phosphate receptors during osteoclast
inactivation by calcitonin. J Cell Sci 97: 439-447.
35. Teitelbaum SL (2000) Bone resorption by osteoclasts. Science 289: 15041508.
36. Paciici R, Brown C, Puscheck E, Friedrich E, Slatopolsky E, et al. (1991)
Effect of surgical menopause and estrogen replacement on cytokine release
from human blood mononuclear cells. Proc Natl Acad Sci U S A 88: 51345138.
37. Rodan GA, Martin TJ (1981) Role of osteoblasts in hormonal control of bone
resorption-a hypothesis. Calcif Tissue Int 33: 349-351.
38. Simonet WS, Lacey DL, Dunstan CR, Kelley M, Chang MS, et al. (1997)
Osteoprotegerin: a novel secreted protein involved in the regulation of bone
density. Cell 89: 309-319.
39. Yasuda H, Shima N, Nakagawa N, Mochizuki SI, Yano K, et al. (1998) Identity
of osteoclastogenesis inhibitory factor (OCIF) and osteoprotegerin (OPG):
a mechanism by which OPG/OCIF inhibits osteoclastogenesis in vitro.
Endocrinology 139: 1329-1337.
40. Yasuda H, Shima N, Nakagawa N, Yamaguchi K, Kinosaki M, et al.
(1998) Osteoclast differentiation factor is a ligand for osteoprotegerin/
osteoclastogenesis-inhibitory factor and is identical to TRANCE/RANKL. Proc
Natl Acad Sci USA 95:3597-3602.
41. Lacey DL, Timms E, Tan HL, Kelley MJ, Dunstan CR, et al. (1998)
Osteoprotegerin ligand is a cytokine that regulates osteoclast differentiation
and activation. Cell 93: 165-176.
42. Anderson DM, Maraskovsky E, Billingsley WL, Dougall WC, Tometsko ME,
et al. (1997) A homologue of the TNF receptor and its ligand enhance T-cell
growth and dendritic-cell function. Nature 390: 175-179.
43. Wong BR, Rho J, Arron J, Robinson E, Orlinick J, et al. (1997) TRANCE is a
novel ligand of the tumor necrosis factor receptor family that activates c-Jun
N-terminal kinase in T cells. J Biol Chem 272: 25190-25194.
44. Suda T, Takahashi N, Udagawa N, Jimi E, Gillespie MT, et al. (1999) Modulation
of osteoclast differentiation and function by the new members of the tumor
necrosis factor receptor and ligand families. Endocr Rev 20: 345-357.
45. Haynes DR, Crotti TN, Zreiqat H (2004) Regulation of osteoclast activity in
peri-implant tissues. Biomaterials 25: 4877-4885.
46. Takayanagi H, Iizuka H, Juji T, Nakagawa T, Yamamoto A, et al. (2000)
Involvement of receptor activator of nuclear factor kappaB ligand/osteoclast
differentiation factor in osteoclastogenesis from synoviocytes in rheumatoid
arthritis. Arthritis Rheum 43: 259-269.
47. Kotake S, Udagawa N, Hakoda M, Mogi M, Yano K, et al. (2001) Activated
human T cells directly induce osteoclastogenesis from human monocytes:
possible role of T cells in bone destruction in rheumatoid arthritis patients.
Arthritis Rheum 44: 1003-1012.
48. Lerner UH (2004) New Molecules in the Tumor Necrosis Factor Ligand and
Receptor Superfamilies with Importance for Physiological and Pathological
Bone Resorption. Crit Rev Oral Biol Med 15: 64-81.
49. Boyle WJ, Simonet WS, Lacey DL (2003) Osteoclast differentiation and
activation. Nature 423: 337-342.
50. Mundy GR, Chen D, Oyajobi BO (2006) Bone remodeling. In: Favus MJ (ed)
Primer on the metoabolic diseases and disorders of mineral metabolism.
American society of bone mineral and research, Washington DC, pp: 46-58.
51. Horowitz MC, Xi Y, Wilson K, Kacena MA (2001) Control of osteoclastogenesis
and bone resorption by members of the TNF family of receptors and ligands.
Cytokine Growth Factor Rev 12: 9-18.
J Clin Cell Immunol
54. Kikuchi T, Matsuguchi T, Tsuboi N, Mitani A, Tanaka S, et al. (2001) Gene
expression of osteoclast differentiation factor is induced by lipopolysaccharide
in mouse osteoblasts via Toll-like receptors. J Immunol 166: 3574-3579.
55. Teng YT, Nguyen H, Gao X, Kong YY, Gorczynski RM, et al. (2000) Functional
human T-cell immunity and osteoprotegerin ligand control alveolar bone
destruction in periodontal infection. J Clin Invest 106: R59-67.
56. Okahashi N, Inaba H, Nakagawa I, Yamamura T, Kuboniwa M, et al. (2004)
Porphyromonas gingivalis induces receptor activator of NF-kappaB ligand
expression in osteoblasts through the activator protein 1 pathway. Infect
Immun 72: 1706-1714.
57. Choi BK, Lee HJ, Kang JH, Jeong GJ, Min CK, et al. (2003) Induction
of osteoclastogenesis and matrix metalloproteinase expression by the
lipooligosaccharide of Treponema denticola. Infect Immun 71: 226-233.
58. Okahashi N, Sakurai A, Nakagawa I, Fujiwara T, Kawabata S, et al. (2003)
Infection by Streptococcus pyogenes induces the receptor activator of NFkappaB ligand expression in mouse osteoblastic cells. Infect Immun 71:948955.
59. Sakurai A, Okahashi N, Nakagawa I, Kawabata S, Amano A, et al. (2003)
Streptococcus pyogenes infection induces septic arthritis with increased
production of the receptor activator of the NF-kappaB ligand. Infect Immun
71: 6019-6026.
60. Mizuno A, Kanno T, Hoshi M, Shibata O, Yano K, et al. (2002) Transgenic mice
overexpressing soluble osteoclast differentiation factor (sODF) exhibit severe
osteoporosis. J Bone Miner Metab 20: 337-344.
61. Nakashima T, Kobayashi Y, Yamasaki S, Kawakami A, Eguchi K, et al. (2000)
Protein expression and functional difference of membrane-bound and soluble
receptor activator of NF-kappaB ligand: modulation of the expression by
osteotropic factors and cytokines. Biochem Biophys Res Commun 275: 768775.
62. Wei S, Kitaura H, Zhou P, Ross FP, Teitelbaum SL (2005) IL-1 mediates TNFinduced osteoclastogenesis. J Clin Invest 115: 282-290.
63. Han X, Kawai T, Eastcott JW, Taubman MA (2006) Bacterial-responsive B
lymphocytes induce periodontal bone resorption. J Immunol 176: 625-631.
64. Jin Q, Cirelli JA, Park CH, Sugai JV, Taba M Jr, et al. (2007) RANKL inhibition
through osteoprotegerin blocks bone loss in experimental periodontitis. J
Periodontol 78: 1300-1308.
65. Bar-Shavit Z (2007) The osteoclast: a multinucleated, hematopoietic-origin,
bone-resorbing osteoimmune cell. J Cell Biochem 102: 1130-1139.
66. Lewiecki EM (2009) Denosumab update. Curr Opin Rheumatol 21: 369-373.
67. Cochran DL (2008) Inlammation and bone loss in periodontal disease. J
Periodontol 79: 1569-1576.
68. Bostanci N, Ilgenli T, Emingil G, Afacan B, Han B, et al. (2007) Gingival
crevicular luid levels of RANKL and OPG in periodontal diseases: implications
of their relative ratio. J Clin Periodontol 34: 370-376.
69. Bostanci N, Ilgenli T, Emingil G, Afacan B, Han B, et al. (2007) Differential
expression of receptor activator of nuclear factor-kappaB ligand and
osteoprotegerin mRNA in periodontal diseases. J Periodontal Res 42: 287293.
70. Mogi M, Otogoto J, Ota N, Togari A (2004) Differential expression of RANKL
and osteoprotegerin in gingival crevicular luid of patients with periodontitis. J
Dent Res 83: 166-169.
71. Liu D, Xu JK, Figliomeni L, Huang L, Pavlos NJ, et al. (2003) Expression of
RANKL and OPG mRNA in periodontal disease: possible involvement in bone
destruction. Int J Mol Med 11: 17-21.
72. Kawai T, Matsuyama T, Hosokawa Y, Makihira S, Seki M, et al. (2006) B and T
lymphocytes are the primary sources of RANKL in the bone resorptive lesion
of periodontal disease. Am J Pathol 169: 987-998.
73. Wara-aswapati N, Surarit R, Chayasadom A, Boch JA, Pitiphat W (2007)
Innate Response to Infectious
Diseases
ISSN:2155-9899 JCCI, an open access journal
�Citation: Srinivasan PC (2013) The Role of Inlammatory Cytokines and the RANKL-RANK-OPG Molecular Triad in Periodontal Bone Loss-A Review.
J Clin Cell Immunol S13: 007. doi:10.4172/2155-9899.S13-007
Page 8 of 8
RANKL upregulation associated with periodontitis and Porphyromonas
gingivalis. J Periodontol 78: 1062-1069.
enhances mRNA levels of proapoptotic genes and caspase activity, which
contribute to impaired healing. Diabetes 55: 487-495.
74. Garlet GP, Martins W Jr., Fonseca BA, Ferreira BR, Silva JS (2004) Matrix
metalloproteinases, their physiological inhibitors and osteoclast factors are
differentially regulated by the cytokine proile in human periodontal disease. J
Clin Periodontol 31:671-679.
82. Liu R, Bal HS, Desta T, Krothapalli N, Alyassi M, et al. (2006) Diabetes
enhances periodontal bone loss through enhanced resorption and diminished
bone formation. J Dent Res 85: 510-514.
75. Nagasawa T, Kobayashi H, Kiji M, Aramaki M, Mahanonda R, et al. (2002)
LPS-stimulated human gingival ibroblasts inhibit the differentiation of
monocytes into osteoclasts through the production of osteoprotegerin. Clin
Exp Immunol 130: 338-344.
76. Valverde P, Kawai T, Taubman MA (2004) Selective blockade of voltage-gated
potassium channels reduces inlammatory bone resorption in experimental
periodontal disease. J Bone Miner Res 19: 155-164.
77. Kawai T, Paster BJ, Komatsuzawa H, Ernst CW, Goncalves RB, et al. (2007)
Crossreactive adaptive immune response to oral commensal bacteria results
in an induction of receptor activator of nuclear factor-kappaB ligand (RANKL)dependent periodontal bone resorption in a mouse model. Oral Microbiol
Immunol 22: 208-215.
78. Mahamed DA, Marleau A, Alnaeeli M, Singh B, Zhang X, et al. (2005) G(-)
anaerobes-reactive CD4+ T-cells trigger RANKL-mediated enhanced alveolar
bone loss in diabetic NOD mice. Diabetes 54: 1477-1486.
79. Rogers JE, Li F, Coatney DD, Otremba J, Kriegl JM, et al. (2007) A p38
mitogen-activated protein kinase inhibitor arrests active alveolar bone loss in a
rat periodontitis model. J Periodontol 78: 1992-1998.
80. Paritt AM (1982) The coupling of bone formation to bone resorption: a
critical analysis of the concept and of its relevance to the pathogenesis of
osteoporosis. Metab Bone Dis Relat Res 4: 1-6.
81. Al-Mashat HA, Kandru S, Liu R, Behl Y, Desta T, et al. (2006) Diabetes
83. Bertolini DR, Nedwin GE, Bringman TS, Smith DD, Mundy GR (1986)
Stimulation of bone resorption and inhibition of bone formation in vitro by
human tumour necrosis factors. Nature 319: 516-518.
84. Nguyen L, Dewhirst FE, Hauschka PV, Stashenko P (1991) Interleukin-1 beta
stimulates bone resorption and inhibits bone formation in vivo. Lymphokine
Cytokine Res 10: 15-21.
85. Diarra D, Stolina M, Polzer K, Zwerina J, Ominsky MS, et al. (2007) Dickkopf-1
is a master regulator of joint remodeling. Nat Med 13: 156-163.
86. Tsuboi M, Kawakami A, Nakashima T, Matsuoka N, Urayama S, et al. (1999)
Tumor necrosis factor-alpha and interleukin-1beta increase the Fas-mediated
apoptosis of human osteoblasts. J Lab Clin Med 134: 222-231.
87. Thammasitboon K, Goldring SR, Boch JA (2006) Role of macrophages in
LPS-induced osteoblast and PDL cell apoptosis. Bone 38: 845-852.
88. Centrella M, McCarthy TL, Canalis E (1988) Tumor necrosis factor-alpha
inhibits collagen synthesis and alkaline phosphatase activity independently of
its effect on deoxyribonucleic acid synthesis in osteoblast-enriched bone cell
cultures. Endocrinology 123: 1442-1448.
89. Taichman RS, Hauschka PV (1992) Effects of interleukin-1 beta and
tumor necrosis factor-alpha on osteoblastic expression of osteocalcin and
mineralized extracellular matrix in vitro. Inlammation 16: 587-601.
90. Eguchi Y, Wakitani S, Imai Y, Naka Y, Hashimoto Y, et al. (2010) Antitumor
necrotic factor agent promotes BMP-2-induced ectopic bone formation. J
Bone Miner Metab 28: 157-164.
Submit your next manuscript and get advantages of OMICS
Group submissions
Unique features:
•
User friendly/feasible website-translation of your paper to 50 world’s leading languages
•
Audio Version of published paper
•
Digital articles to share and explore
Special features:
Citation: Srinivasan PC (2013) The Role of Inlammatory Cytokines and the RANKL-RANKOPG Molecular Triad in Periodontal Bone Loss-A Review. J Clin Cell Immunol S13: 007.
doi:10.4172/2155-9899.S13-007
This article was originally published in a special issue, entitled: “Innate
Response to Infectious Diseases”, Edited by Dr. Anshu Agrawal, University
of California Irvine, USA
J Clin Cell Immunol
•
250 Open Access Journals
•
20,000 editorial team
•
21 days rapid review process
•
Quality and quick editorial, review and publication processing
•
Indexing at PubMed (partial), Scopus, EBSCO, Index Copernicus and Google Scholar etc
•
Sharing Option: Social Networking Enabled
•
Authors, Reviewers and Editors rewarded with online Scientiic Credits
•
Better discount for your subsequent articles
Submit your manuscript at: www.editorialmanager.com/clinicalgroup
Innate Response to Infectious
Diseases
ISSN:2155-9899 JCCI, an open access journal
�
 Prathiba Srinivasan
Prathiba Srinivasan