Academia.edu no longer supports Internet Explorer.
To browse Academia.edu and the wider internet faster and more securely, please take a few seconds to upgrade your browser.
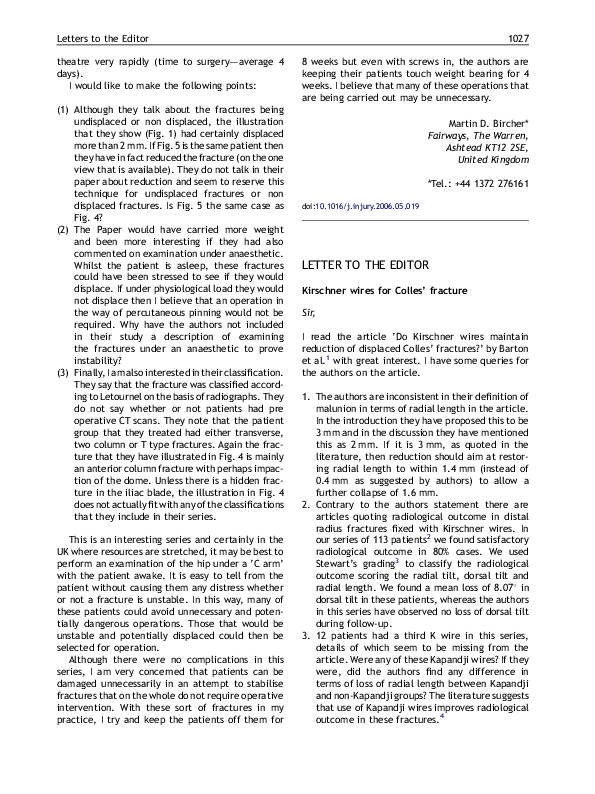
Kirschner wires for Colles’ fracture
 Harish Kurup
Harish KurupRelated Papers
Acta Chirurgiae Orthopaedicae Et Traumatologiae Cechoslovaca
Direct Radiography Following Fracture Reduction Improves the Reliability of Pauwels Classification2021 •
Ethiopian Journal of Health Sciences
Evaluation of the Inter and Intra-Observer Reliability of the AO Classification of Intertrochanteric Fractures and the Device Choice (DHS, PFNA, and DCS) of FixationsBACKGROUND:ArbeitsgemeinschaftfürOsteosynthesefragen (AO) classification is the most frequently used tool to classify intertrochanteric fractures. However, there is limited evidence regarding its reliability. Therefore, this study was designed to evaluate inter-observer and intra-observer reliability of the AO-2018 intertrochanteric fracture classification.METHOD: A retrospective study was conducted in Imam Khomeini Hospital Complex, on radiography of patients who came with intertrochanteric fractures from March 21, 2018, to March 19, 2019. Four orthopedic trauma surgeons assessed 96 anteroposterior pelvic radiographs of intertrochanteric fractures and classified using an AO intertrochanteric fracture classification of 2018. The reading and review of radiography were performed in 2 separate occasions in a 1-month interval. The inter-observer and intra-observer reliability was assessed using kappa statistics.RESULT: The level of both mean inter-observer (K =0.322; 95%CI: 0.321-0.323)...
Orthopaedics & traumatology, surgery & research : OTSR
The reliability of a simplified Garden classification for intracapsular hip fractures2012 •
The Garden classification is used to classify intracapsular proximal femur fractures. The reliability of this classification is poor and several authors advise a simplified classification of intracapsular hip fractures into non-displaced and displaced fractures. However, this proposed simplified classification has never been tested for its reliability. We estimate simplifying the classification of femoral neck fractures will lead to a higher inter-observer agreement. Ten observers, trauma surgeons and residents, from two different institutes classified 100 intracapsular femoral neck fractures. The inter-observer agreements were calculated using the multi-rater Fleiss' kappa. The inter-observer kappa for the Garden classification was 0.31. An agreement of κ0.52 was observed if the Garden classification was simplified and the fractures were classified by our observers as 'non-displaced' or 'displaced'. No difference in reliability was seen for the use of the four-g...
RELATED PAPERS
Alexander Reis (Hrsg.), Das Rhein-Main-Gebiet in der Spätantike – Beiträge zur Archäologie und Geschichte Akten der Tagung in Obernburg am Main vom 12.–13. April 2018
The glass bowl from Obernburg and the early Christian evidence in Southwest Germany and Alsace / Die Glasschale von Obernburg und die frühchristlichen Zeugnisse in Südwestdeutschland und im Elsass2022 •
La gobernanza armada ilegal y su transferencia al Estado para construir la paz
La gobernanza armada ilegal y su transferencia al Estado para construir la paz2018 •
2017 •
2nd International Conference on Quaternary Sciences
Clay mineralogy of the sediments in Sabzevar playa, NE Iran; implication for the late quaternary climate changes2021 •
Surface and Interface Analysis
Analysis of lithium transport in electrochromic multilayer films by neutron depth profiling2000 •
2023 •
International Journal of Humanities and Educational Research
Symmetry of Syntactic Structure in the Qur'Anic ExpressionEuropean journal of cardio-thoracic surgery : official journal of the European Association for Cardio-thoracic Surgery
Management of postoperative pain as part of a successful multidisciplinary lung volume reduction surgery programme2015 •
RELATED TOPICS
- Find new research papers in:
- Physics
- Chemistry
- Biology
- Health Sciences
- Ecology
- Earth Sciences
- Cognitive Science
- Mathematics
- Computer Science