Current Obstetrics & Gynaecology (1998) 8, 2-7
© 1998 Harcourt Brace & Co. Ltd
Mini-symposium: The placenta
Aspects of structure and function in human placenta
T. M. Mayhew and L. Leach
This review summarizes essential features of the functional morphology of human term placenta,
concentrating on the processes of proliferation, growth, diffusive transport and microvascular
permeability. It introduces the main structures that make up the 'villous membrane' interposed
between the maternal and fetal bloods. It then presents an updated view of the proliferation of the
principal functional compartment of the membrane, the trophoblast. This is a continuously renewing
epithelium: cytotrophoblast cells divide mitotically throughout gestation and are recruited into the
overlying syncytium. Contrary to previous dogma, cytotrophoblast is not depleted during gestation.
The syncytium loses nuclei in large aggregates (syncytial knots), which detach into the maternal
circulation. At least some nuclei are apoptotic and may be phagocytosed by macrophages at
extraplacental sites. The villous stroma and fetal endothelium also grow by proliferation. These
processes help to expand exchange surface areas and minimize diffusive distances, structural
quantities that can be used to estimate placental-oxygen diffusive conductance. The fetal vascular
compartment contributes substantially to overall transplacental resistance to solute transport. Fetal
vessels are lined by a continuous endothelium with well-differentiated junctional complexes in the
paracellular clefts. These complexes contain adhesion molecules that are vulnerable to exogenous
agents, and whose expression and localization have been linked with junctional disruption and altered
permeability, and altered placental efficiency and permeability. Changes in placental proliferation,
growth, diffusive transport and vascular permeability may all play a role in pregnancy-related
disorders such as pre-eclampsia and diabetes.
OVERVIEW OF PLACENTAL STRUCTURE
In the human haemochorial placenta, villous trees
bathed by maternal blood circulating through the
intervillous space are crucial to placental growth,
morphogenesis and function and, hence, to fetal
well-being.I,: Because of their number and physical
attributes, terminal villi (TV) are the most influential
in determining functional activity, and exchanges
between maternal and fetal blood occur via the villous
T. M. Mayhew, L. Leach, School of Biomedical Sciences
University of Nottingham, Queen's Medical Centre, Nottingham
NG7 2UH, UK
Correspondence to: T.M.M.
membrane (VM), which comprises trophoblast,
stroma and the endothelium of fetal mierovessels.
Trophoblast is a two-compartment epithelium. An
inner proliferative zone, the cytotrophoblast (CT),
transforms during gestation from a complete layer to a
set of dispersed cells from which post-mitotic cells are
recruited into an outer terminally-differentiated syncytiotrophoblast (ST). The syncytium is all but unique
in human tissues and may have evolved to allow invasion of maternal tissues without breaching the intervascular barrier. Moreover, syncytium also permits
the economical regional redistribution of ST mass
and, hence, economical adaptations to improve diffusive conductance? Its effectiveness in this regard is
related to its mean thickness, variability of thickness
�Placental structure and function
3
and surface area. During pregnancy the VM becomes
thinner, whilst surface area and volume increase
enormously, further enhancing placental functional
capacity. Most expansion occurs after 20 weeks by
the formation of new TV. 2'44
The second major discriminatory barrier of the
villous membrane is the fetal endothelium. This is a
continuous endothelium with numerous tight and
adhaerens junctions present in the intercellular clefts.
Fetal microvessels are fairly 'tight' and their permeability values approach those seen for skeletal muscle
microvessels rather than the leakier microvessels
found in the heart, liver or kidney.7,8 Dilation and
peripheralization of fetal microvessels, together with
dispersal of CT cells, lead to localized attenuation of
the VM (at vasculosyncytial membranes, thickness
less than 2 gm), as well as thickened regions where ST
nuclei aggregate (syncytial knots, thickness 10-15 gm).
Surface area expands faster than volume so the ST
becomes progressively thinner overall. This design
ensures t h a t maternal and fetal vascular beds are
brought into close proximity over an extensive area.
The beds are separated by the VM and this paper
focuses attention on some recent changes in our perceptions of the VM and its structural ingredients.
A NEW VIEW OF TROPHOBLAST
PROLIFERATION AND GROWTH
The prevailing notion of trophoblast growth has been
one of conditional expansion limited by a shrinking
pool of CT cells? ,9 Recent stereological studies on the
actual numbers of CT and ST nuclei have altered this
view to one of a continuously renewing epithelium
(like small intestine), in which recruitment and
extrusion are regulated. ~°'H From the first trimester
onwards, trophoblast expands by the continuous proliferation of CT cells and increases in the absolute
numbers of CT and ST nuclei.
Because CT cells become more widely dispersed as
ST area expands, 6,J°the use of 2D histological sections
gives the erroneous impression that CT cells decline in
number during gestation. In fact, not only are CT cells
not depleted by recruitment into ST, but the numerical
ratio of ST:CT nuclei (about 9:1)and volume of protoplasm per nucleus (about 1100 ~tm3) are maintained.
Ratios are preserved despite the shedding of nucleated
ST fragments as syncytial knots. Maybe as many as
150 000 fragments per day enter the maternal systemic
circulation. The proportion of trophoblast volume
occupied by CT cells at term (about 15%) also remains
remarkably constant over the villous tree,4 suggesting
that trophoblast turnover occurs at all levels.
The notion of continuous recruitment is consistent
with CT cells still being mitotically active near term
and with discontinuity of the CT layer, but it is incompatible with nett loss of CT cells. 1,9,12In full-term placentae, CT cells can be seen forming desmosomes and
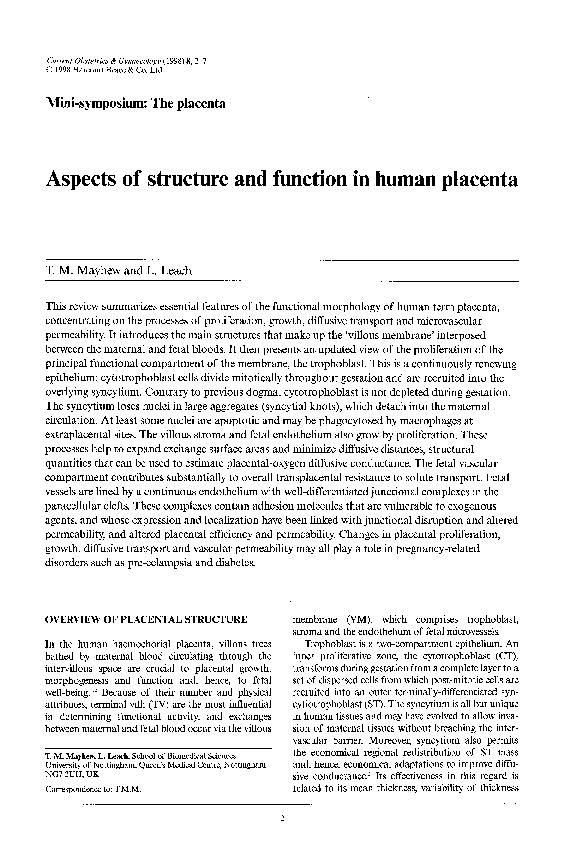
Fig. 1 Electronmicrographof a term placentalchorionicvillus
showinga syncytialknot (sk) arisingfrom the underlying
syncytiotrophoblast(syn).The nuclearaggregatesin the syncytial
knots appear pyknoticand, sometimes,apoptotic.Paler staining
cytotrophoblast(cy) and fetal vessels(fv)lined with continuous
endothelium(e) can be seen. The villousstroma (s) contains
macrophagesand pericytes.Bar = 10 gm
adhaerens junctions with the overlying ST. Immunochemistry reveals brightly fluorescent punctate staining of the epithelial adhaerens adhesion molecules
E-cadherin and ~-catenin on the apical surface of
CT cells (unpublished observation). The gradual
transformation from a two-layered to an essentially
single-layered epithelium has implications for
maternofetal transfer of immunoglobulins. The intact
CT layer may act as a barrier to IgG transfer ~3at least
until its cells separate and disperse. IgG is known to
be transcytosed through endosomal compartments of
the ST and fetal endothelium? 4
The qualitative morphology of trophoblast has been
examined microscopically.1,2 Such studies raise the
question of how a constant volume of trophoblast per
nucleus might be conserved. One possibility is via the
loss of nucleus-rich ST fragments (Fig. 1). CT nuclei
vary in size but tend to be rounded and euchromatic
with, occasionally, prominent nucleoli. ST nuclei are
smaller, indented and more heterochromatic. In syncytial knot regions, they are more pleiomorphic, densely
packed, heterochromatic and convoluted. Finally, certain regions of ST harbour closely packed nuclei with
apoptotic features. 15 In other tissues, apoptotic nuclei
are removed by macrophages. This appears not to happen in ST, although it is possible that syncytial-knot
�4
Current Obstetrics & Gynaecology
fragments in the maternal circulation are phagocytosed
by macrophages at extraplacental sites.
It is probable that extrusion of syncytial knots normally occurs without disrupting the integrity of the
VM. Occasionally, the VM is injured leading to local
denudation of ST and release of syncytial knot
fragments. Apoptosis may be another process that
initiates denudation? 5
PLACENTAL GROWTH IS MONOPHASIC AND
NOT BIPHASIC
Until recently, ~°'1~there was uncertainty about whether
placental growth is biphasic (a proliferation phase
followed after 36 gestational weeks by a hypertrophic
phase) or monophasic (solely proliferative). Wider
aspects of villous growth from 12 weeks to term have
been reassessed by stereological studies I°,Hwhose findings contradict the claim that placental growth is
biphasic. Numbers of CT, ST, stromal and endothelial
nuclei were found to increase exponentially and
roughly in parallel, outstripping changes in placental
volume and suggesting that growth in different compartments is tightly regulated. Growth varied between
compartments, but nuclear proliferation was always
dominant. In stroma, the volume of tissue per nucleus
declined. In capillaries, ,the mean area of an endothelial squame increased and squame density per unit
length declined. Immunochemical studies suggest that
there are centres of proliferation for epithelium,
stroma and vascular endothelium? 2 The growth constant for endothelial nuclei may be greater than that
for CT and stromal cells, and this fits the idea that
genesis and growth of TV are affected by the linear
growth of fetal vessels) Fetal endothelium expresses
CD44, thyl and A10-33/1, markers associated with
proliferating endothelial cells such as those present in
malignant tumours and in culture (unpublished,
results).
CORRELATING STRUCTURE WITH
DIFFUSIVE CONDUCTANCE
Variation in thickness of the VM is beneficial. It
allows more effective diffusion than would be possible
with a uniform membrane of identical arithmetic
mean thickness 3and is achieved, partly, by redistributing ST mass following obtrusion by underlying fetal
vessels or by active protoplasmic flow. 16'17The outcome is a Combination of vasculosyncytial membranes and syncytial knots.
The critical structural determinants of placental
diffusive conductance (diffusing capacity, Dp) are
exchange surface areas and effective (harmonic mean)
diffusion distances. Dp (ml.min-X.kPa -1) measures the
ease with which a gas or nutrient diffuses across the
placenta, and depends on the physical properties of
tissues and physicochemical properties of the diffusing substance. The intervascular pathway for oxygen
diffusion can be analysed as a set of up to six tissue
layers each of which offers a partial resistance to flow.
Being arranged serially, the partial resistances can be
summed to obtain overall resistance, which is the
reciprocal of total Dr. The six layers allow: (1) dissociation of oxygen from haemoglobin in maternal erythrocytes, me; diffusion across (2) maternal plasma,
mp; (3) trophoblast, tr; (4) villous stroma, st; (5) fetal
plasma, fp; and (6) association with haemoglobin in
fetal erythrocytes, fe. TM Hence, total resistance to
oxygen flow can be expressed as:
f
llDp = 1/Dme + l/Drop + l/Dtr + l/Dst + 1/Dfp + l/Dr.
The partial conductances Dm~ and Df~ depend on vascular-space volumes and oxygen-haemoglobin reaction
rates. The conductances Drop, D,~r Dst and Dfp are governed by Fick's law of diffusion and, consequently, by
exchange surface areas (S), tissue-layer thicknesses (T)
and tissue permeability to oxygen (K). Each conductance can be estimated via a modified Fick equation:
D = K.S/T h
where T h is harmonic mean thickness and S is the
average of the upstream (maternal) and downstream
(fetal) surfaces of each layer.
A modified Fick equation is required because the
arrangement of tissue ingredients in human placenta
is complex. Trophoblast varies in thickness (from vasculosyncytial membranes to syncytial knots) and so
oxygen conductances vary locally. For this reason, it is
better to estimate harmonic rather than arithmetic
thicknesses 3 thereby giving greater weight to thinner
regions. In addition, the downstream side of the
stroma is represented, not by a sheet, but by the
endothelium of individual capillaries. Consequently,
capillary and villous surface areas may be unequal.
The same may apply to trophoblast and other layers.
Since oxygen must cross both surfaces of each layer, it
is preferable to take S as the mean of two surfaces.
Provided that certain sampling requirements are
met, stereological estimation of the key structural
quantities provides a theoretically maximal Dp that
might be found under optimal conditions. In reality,
malperfusion, mismatching of maternal and fetal
blood flows, and arteriovenous shunting reduce the
efficiency of oxygen diffusion. Physiological estimation o f Dp is complicated further by the problems of
estimating oxygen tensions at the sites of exchange.
An added advantage of this morphometric
approach is that changes in all compartments of the
pathway are assessed and given appropriate weighting. The approach has been used to explore the relative resistance to oxygen transfer contributed by each
layer, and has indicated that VM accounts for about
90% of total resistance. 1819
,
The surface available for oxygen diffusion increases
during gestation whilst the harmonic mean thickness
�Placental structure and function
of the VM falls. Therefore, D P should increase and,
indeed, evidence for this has been adduced ~ suggesting that earlier uncertainties about how fetal growth
continues despite declining relative volumes and surfaces of villi might be attributed to failure to monitor
a sufficient set of structural variables. Influential
changes occur in the trophoblast and stroma and,
from l0 to 41 weeks, the rise in total D P is commensurate with the gain in fetal weight, indicating that functional maturation of the placenta is matched to fetal
growth.
Estimates o f Dp for oxygen have also been made
in abnormal pregnancies associated with hypoxia.
These include high altitude (hypobaric hypoxia),
maternal anaemia (normobaric hypoxia), preeclampsia (ischaemic hypoxia) and maternal diabetes
mellitus (in which chronic fetal stress is indicated by
elevated levels of fetal haemoglobin and erythropoietin). In all cases, there is thinning of the VM (with or
without impoverished growth of villi and expansion
of the intervillous space) and partial, total or specific
diffusion conductances are increased) °43 On the Fick
model, exchange surface area and harmonic thickness
strongly influence D P. Of the two, the latter has the
more impact, and this makes good sense because it is
an economical and effective strategy for improving
Dp. 19As an adaptive strategy, producing more TV has
the possible disadvantage of increasing blood volume
and placing an extra burden on the fetal cardiovascular system beyond that afforded by, for example,
elevated haematocrits.
BARRIER FUNCTION OF THE FETAL
MICROVASCULAR ENDOTHELIUM
The general consensus of endothelial biologists is that
permeability of continuous microvessels is conferred
by resistances in series: the luminal gl~ycocalyx, fibre
matrix of the inter-endothelial wide zones, tight
junctions and basement ,membrane. The structural
complexity and molecular organization of these ingredients depend on the tissue in which the vessels are
located and on whether they lie in the arteriolar, capillary or venular parts of the local circulation. The
ultrastructure of placental fetal endothelium suggests
that it is a fairly restrictive barrier to transport of
solutes. Unlike other non-brain continuous capillaries, the dilated capillaries in TV contain few caveolae.
Coated vesicles, endosomes and free vesicles are present, so the endothelium is capable of vesicular transport? ~ The paracellular clefts between adjoining
endothelial cells offer the major transport pathway for
hydrophilic solutes, and possess from one to four tight
junctional regions? Where adjoining membrane
leaflets are closely apposed, but not fused, there is a
roughly 4 nm separation. This gap may allow transport of water and solutes less than 4 nm in diameter.
Serial sectioning of tight junctions has shown that
5
Fig. 2 Confocal micrographs of term placental fetal microvessels
which have been tilted in the Y axis. VE-cadherin, an adhesion
molecule exclusive to endothelial adhaerens junctions, can be seen
as bright fluorescent blebs (arrowheads) on the luminal membrane
of the endothelium lining fetal vessels (fv). Progressive tilting
(5 ° tilts, a~:l) reveals that staining is not continuous but is punctate
along the paracellular clefts of vessels (arrows). Trophoblast (t) is
also indicated. Bar = 10 gm.
they are not continuous throughout the length of the
capillaries but disappear within four to seven serial
sections when section 60-70 nm thick are used. The
separation of leaflets in these discontinuities (wide
zones) is about 17 nm. Hydrophilic molecules, therefore, have a tortuous route to negotiate as they cross
from the abluminal to luminal side of the blood vessel. The discontinuous tight junctions are a common
feature of non-brain capillaries.
The wide zones of paracellular clefts contain junctional complexes called adhaerens junctions (Fig. 2).
These contain transmembrane adhesion molecules
that belong to the cadherin group of cell-cell adhesion
molecules. The latter are linked to the internal actin
cytoskeleton viX peripheral linking molecules ~catenin, [3-catenin, plakoglobin, vinculin and c~actinin. 24 All cadherins have an extracellular portion
with calcium binding, adhesive and glycosylation sites,
as: well as a transmembrane domain and cytoplasmic
tail that possess phosphorylation and ~cytoskeletal
binding sites. Thus, their structure suggests susceptibility to both external and internal cues that may affect
homophilic binding a n d s o
regulate junctional
integrity and permeability. The extracellular portions
of cadherins may, along with their role in endothelial
cell-cell adhesion, be part of the fibre-matrix molecular sieve that influences solute transport. Placental
adhaerens junctions are rich in VE-cadherin. 25In vitro
studies using human umbilical vein endothelial cell
(HUVEC) monolayers have shown tha( VE-cadherin
is expressed in cell-cell contact only when cells reach
�6
Current Obstetrics & Gynaecology
confluence. Furthermore, blocking VE-cadherin with
antibodies results in gap formation and leakage of
haem proteins? 4 VE-cadherin is linked to cytoplasmic
actin via cx-catenin, J3-catenin and plakoglobin. These
peripheral linking molecules are also vulnerable to
phosphorylation and are thought, therefore, to be
ligands for signal transduction. Changes in these
molecules, or in actin, may affect localization and
binding of VE-cadherin with resultant junctional
separation and increased permeability.
Perfusion of human placental microvessels for
30rain with 100 gM histamine 26 results in altered
localization of VE-cadherin, a twofold increase in the
separation observed in tight junctional regions, and
an 80% increase in leakage of cyanocobalamin
(RMM 1200). Recent observations in our laboratory
have revealed that histamine also affects immunolocalization of catenins. In vitro studies using HUVEC
cells have demonstrated that adhaerens junctional
molecules are Vulnerable to a range of inflammatory
mediators and cytokines such as thrombin,
bradykinin, tumour necrosis factor-~ and interleukins
1 and 6. Incubations with these vasoactive agents
result in changes in both the expression and
immunolocalization of these molecules, as well as
altering permeability. Endothelial cells can be isolated
from microvessels of the term placenta 27 and also
express junctional adhesion molecules that appear
vulnerable to exogenous agents. The effects of long
duration diseases such as diabetes and pre-eclampsia,
where elevated glucose levels and abnormal blood
flow are major factors, is an area of recent interest.
Endothelial cells in culture are vulnerable to high glucose, there are reports of altered expression of
PECAM-1 ?8 Ongoing research in our laboratory suggests that diabetes and high glucose may be linked
with differential expression of VE-cadherin and
PECAM-1 in placental microvessels.
PECAM-1, a molecule thought to be involved in
adhesion and transmigration of leucocytes, is found
on the luminal membrane and the intercellular cleft of
placental microvessels. It was localized to separate but
neighbouring membrane microdomains to that seen
for VE-cadherin. 25 This molecule appears to be vulnerable to histamine ~6 and its downregulation has
been linked to increased endothelial permeability.
Ultrastructural studies show that" placental
endothelium possesses luminal and abluminal caveolae
that are connected to one or the other plasma
membrane with no interconnecting vesicles or
transendothelial channels. The endothelial cells possess coated vesicles, early and late endosomes, lysosomes and free vesicles - organelles for endocytosis
and transcytosis of macromolecules such as I g G ? 4'29
The endothelial plasma membranes contain heterogeneous-receptor populations necessary for uptake and
transcytosis of macromolecules, such as insulin-like
growth factor and IgG? 9 The luminal surface of
microvessels is lined by an extensive glycocalyx that
extends into the mouth of the paracellular cleft and
luminal caveolaeY It is therefore, a constituent of both
the transcellular and paracellular diffusion pathway.
As stated before, the overall surface area of the
microvessels plays an important role in transplacental
diffusion of solutes. TV cont]ain very long, looped
capillaries that form sinusoids. These may be adaptations to reduce the thickness of the intervascular barrier (thus increasing the diffusion capacity) and slow
fetal blood flow (thus increasing the time available for
the exchange of substances between maternal and
fetal circulations). Both hypobaric hypoxia and gestational diseases, such as pre-eclampsia and diabetes,
appear to influence the extent of vascularization and
capillary diameter. 19,22
MICROVASCULAR PERMEABILITY
Placental physiologists have been concerned mainly
with the permeability of the intervascular barrier, the
individual contribution of endothelium being largely
ignored. However, it has been pointed out that the
placenta has the characteristics of a filter with infrequent large pores and numerous small pores in series,
and that the latter could well be endothelial. 3°Human
placental microvessels appear to be fairly restrictive.
Although horseradish peroxidase (HRP, R M M
40 000 Da) crosses the paracellular clefts when placental vessels are perfused with high concentrations
of cationic HRP, larger molecules such as IgG appear
to take a transcellular route?"
By using the single-passage multiple=tracer dilution
technique, it has been shown that there is a substantial
restriction to the diffusion of radiolabelled cyanocobalamin (RMM 1353, molecular radius 0.84 nm) in
term human placental microvessels perfused extracorporeally. 7 Comparing the permeability values for
cyanocobalamin and EDTA in placental microvessels
with those published for some other microvascular
beds shows that term human microvessels are
marginally less permeable than skeletal muscle capillaries, and far more restrictive than cardiac capillaries.
ACKNOWLEDGEMENTS
We wish to thank all our colleagues who have worked with us on the
research cited in this paper, including Wan Ismail, an Honours
student, for supplying the electron micrograph of Figure 1. Our
placental researches have been supported by The Anatomical
Society of Gt Britain & Ireland, The Cunningham Trust,
Leverhulme Trust and Wellcome Trust.
REFERENCES
1. Dearden L, Ockleford CD. Structure of human trophoblast:
correlation with function. In: Loke C, White H (eds). Biology
of Trophoblast. London: Elsevier, 1983:69-110
2. Kaufmann P, Burton GJ. Anatomy and genesis of the
placenta. In: Knobil E, Neil JD (eds). The Physiology of
Reproduction. New York: Raven Press, 1994:441-484
3. Jackson MR, Joy CF, Mayhew TM, Haas JD. Stereological
studies on the true thickness of the villous membrane in
�Placental structure and function
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
human term placentae: a study of placentae from highaltitude pregnancies. Placenta 1985; 6:249~58
Sen DK, Kaufmann P, Schweikhart G. Classification of
human placental villi. II. Morphometry. Cell Tissue Res 1979;
200:425-434
Boyd PA. Quantitative structure of the normal human
placenta from 10 weeks of gestation to term. Early Human
Develop 1984; 9:297-307
Jackson MR, Mayhew TM, Boyd PA. Quantitative description
of the elaboration and maturation of villi from 10 weeks of
gestation to term. Placenta 1992; 13: 357-370.
Eaton BM, Leach L, Firth JA. Permeability of perfused
term human placental microvessels. J Physiol 1993; 463:
141-155
Leach L, Firth JA. Fine structure of the paracellular junctions
of terminal villous capillaries in the perfused human placenta.
Cell Tiss Res 1992; 268:447-452
Arnholdt H, Meisel F, Fandrey K, Lohrs U. Proliferation of
villous trophoblast of the human placenta in normal and
abnormal pregnancies. Virchows Archiv B Cell Pathol 1991;
60:365-372
Mayhew TM, Simpson RA. Quantitative evidence for the
spatial dispersal of trophoblast nuclei in human placental villi
during gestation. Placenta 1994; 15:837-844
Mayhew TM, Wadrop E, Simpson RA. Proliferative versus
hypertrophic growth in tissue subcompartments of human
placental villi during gestation. J Anat 1994b; 184:535-543
Blankenship TN, King BE Developmental expression of Ki67 antigen and proliferating cell nuclear antigen in Macaque
placentas. Develop Dynamics 1994; 201:324-333
Bright NA, Ockleford CD. Cytotrophoblast cells: a barrier to
maternofetal transmission of passive immunity? J Histochem
Cytochem 1995; 43:933 944
Leach L, Eaton BM, Firth JA, Contractor SE
Immunocytochemical and labelled tracer approaches to
uptake and intracellular routing of immunoglobulin-G (IgG)
in the human placenta. Histochem J 1991; 23:444449
Nelson DM. Apoptotic changes occur in syncytiotrophoblast
of human placental villi where fibrin type fibrinoid is
deposited at discontinuities in the villous trophoblast.
Placenta 1996; 17:382391
Jackson MR, Mayhew TM, Haas JD. On the factors which
contribute to thinning of the villous membrane in human
placentae at high altitude. I. Thinning and regional variation
in thickness of trophoblast. Placenta 1988a; 9:1-8
Jackson MR, Mayhew TM, Haas JD. On the factors which
contribute to thinning of the villous membrane in human
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
7
placentae at high altitude. II. An increase in the degree of
peripheralization of fetal capillaries. Placenta 1988b; 9:9-18
Mayhew TM, Jackson MR, Boyd PA. Changes in oxygen
diffusive conductances of human placentae during gestation
(10-41 weeks) are commensurate with the gain in fetal weight.
Placenta 1993a; 14:51-61
Mayhew TM, Jackson MR, Haas JD. Microscopical
morphology of the human placenta and its effects on oxygen
diffusion: a morphometric model. Placenta 1986; 7:121-131
Jackson MR, Mayhew TM, Haas JD. Morphometric studies
on villi in human term placentae and the effects of altitude,
ethnic grouping and sex of newborn. Placenta 1987b, 8:
487-495
Mayhew TM, Sorensen FB, Klebe JG, Jackson MR. Oxygen
diffusive conductances in placentae from control and diabetic
women. Diabetologia 1993b; 36:955-960
Mayhew TM, Sorensen FB, Klebe JG, Jackson MR. Growth
and maturation of villi in placentae from well-controlled
diabetic women. Placenta 1994a; 15:57-65
Reshetnikova OS, Burton GJ, Teleshova OV. Placental
histomorphometry and morphometric diffusing capacity of
the villous membrane in pregnancies complicated by maternal
iron-deficiency anemia. Am J Obstet Gynecot 1995; 173:
724-727
Dejana E, Corada M, Lampugnani MG. Endothelial cell-cell
junctions. The FASEB Journal 1995; 916:910-917
Leach L, Clark P, Lampugnani M-G, Arroyo AG, Dejana E,
Firth JA. Immuno-electron characterisation of the interendothelial junctions of human term placenta. J Cell Sci 1993;
104:1073-1081
Leach L, Eaton BM, Westcott EDA, Firth JA. Effect of
histamine on endothelial permeability and structure and
adhesion molecules of the paracellular junctions of perfused
human placental microvessels. Microvasc Res 1995; 50:
323-337
Leach L, Bhasin Y, Clark P, Firth JA. Isolation of endothelial
cells from human term placental villi using immunomagnetic
beads. Placenta 1994; 15:355-364
Baumgartner-Parzer S, Wagner L, Pettermann M, Gessl A,
Waldhausl W. Modulation by high glucose of adhesion
molecule expression in cultured endothelial cells. Diabetologia
1995; 38:1367-1370
Bright NA, Ockleford CD, Anwar M. Ontogeny and
distribution of Fc gamma receptors in the human placenta.
Transport or immune surveillance? J Anat 1994; 184:297-308
Stulc J. Extracellular transport patlaways in the haemochorial
placenta. Placenta 1989; 10:113-119
�
 L. Leach
L. Leach