Tebala et al.
World Journal of Emergency Surgery
(2022) 17:22
https://doi.org/10.1186/s13017-022-00425-z
Open Access
RESEARCH
The weekend effect on the provision
of Emergency Surgery before and during
the COVID-19 pandemic: case–control analysis
of a retrospective multicentre database
Giovanni D. Tebala1,2*, Marika S. Milani3, Roberto Cirocchi2, Mark Bignell1, Giles Bond-Smith1,
Christopher Lewis1, Vanni Agnoletti4, Marco Catarci5, Salomone Di Saverio6, Gianluigi Luridiana7,
Fausto Catena8, Marco Scatizzi9, Pierluigi Marini10 and the CovidICE-International Collaborative
Abstract
Introduction: The concept of “weekend effect”, that is, substandard healthcare during weekends, has never been
fully demonstrated, and the different outcomes of emergency surgical patients admitted during weekends may be
due to different conditions at admission and/or different therapeutic approaches. Aim of this international audit was
to identify any change of pattern of emergency surgical admissions and treatments during weekends. Furthermore,
we aimed at investigating the impact of the COVID-19 pandemic on the alleged “weekend effect”.
Methods: The database of the CovidICE-International Study was interrogated, and 6263 patients were selected for
analysis. Non-trauma, 18+ yo patients admitted to 45 emergency surgery units in Europe in the months of March–
April 2019 and March–April 2020 were included. Demographic and clinical data were anonymised by the referring
centre and centrally collected and analysed with a statistical package. This study was endorsed by the Association of
Italian Hospital Surgeons (ACOI) and the World Society of Emergency Surgery (WSES).
Results: Three-quarters of patients have been admitted during workdays and only 25.7% during weekends. There
was no difference in the distribution of gender, age, ASA class and diagnosis during weekends with respect to
workdays. The first wave of the COVID pandemic caused a one-third reduction of emergency surgical admission both
during workdays and weekends but did not change the relation between workdays and weekends. The treatment
was more often surgical for patients admitted during weekends, with no difference between 2019 and 2020, and procedures were more often performed by open surgery. However, patients admitted during weekends had a threefold
increased risk of laparoscopy-to-laparotomy conversion (1% vs. 3.4%). Hospital stay was longer in patients admitted
during weekends, but those patients had a lower risk of readmission. There was no difference of the rate of rescue surgery between weekends and workdays. Subgroup analysis revealed that interventional procedures for hot gallbladder
were less frequently performed on patients admitted during weekends.
*Correspondence: gtebala@gmail.com
2
Digestive and Emergency Surgery Unit, Azienda Ospedaliera “S.Maria”,
“S.Maria” Hospital, Viale Tristano di Joannuccio, 05100 Terni, Italy
Full list of author information is available at the end of the article
A complete list of Collaborators of the CovidICE-International
Collaborative can be found in Appendix.
© The Author(s) 2022. Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which
permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the
original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or
other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line
to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory
regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this
licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativeco
mmons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
�Tebala et al. World Journal of Emergency Surgery
(2022) 17:22
Page 2 of 10
Conclusions: Our analysis revealed that demographic and clinical profiles of patients admitted during weekends do
not differ significantly from workdays, but the therapeutic strategy may be different probably due to lack of availability
of services and skillsets during weekends. The first wave of the COVID-19 pandemic did not impact on this difference.
Keywords: Weekend effect, Emergency surgery, Hot gallbladder
Introduction
The so-called weekend effect is a suspected epidemiological effect representing a source of serious concern for
healthcare professionals, policy-makers and the general
public. It has been claimed that during weekends workload and capacity of healthcare systems may change completely with respect to workdays, causing substandard
care and suboptimal results. The first definition of “weekend effect” was related to a reported increase of mortality
in patients admitted during weekends, but nowadays it
refers—more widely—to the differences in the provision
of healthcare between workdays and weekend. In the present paper, the “weekend effect” will be considered in this
wider sense.
In 2016, the then UK Secretary of State for Health
claimed that 11,000 deaths per year could be caused by
the “weekend effect”, raising concerns among the population and leading to the implementation of the “seven-day
hospital services” policy in the NHS [1]. However, that
statement was subsequently found to be inaccurate as
the comparison between workdays and weekends did not
take into consideration that patients admitted to Emergency Departments during weekends were usually more
ill and in poorer general conditions. At that time, several
academics wrote to the Secretary of State for Health to
complain about that misrepresentation of facts based on
“bad” evidence, only for political convenience. Nevertheless, the evidence behind an alleged weekend effect is still
unclear. Moreover, the massive shake-up of our healthcare systems caused in the last 2 years by the COVID
pandemic could have exacerbated an eventual weekend effect, due to an alleged further reduction of capacity during lockdown weekends, but this has not been
demonstrated.
To confirm or rule out the impact of a “weekend effect”
on emergency surgical admissions, we have interrogated
our large international database on emergency surgical
admission before and during the COVID pandemic.
Materials and methods
Data for this study were derived from the CovidICEInternational Study database, whose characteristics have
been reported elsewhere [2].
The initial recruitment of participating units was
done by emailing an invitation letter to more than 6000
surgeons in Europe. Forty-five Emergency Surgical units
decided to contribute to the CovidICE-International
database. A local team led by a Principal Local Investigator (PLI) for each centre collected anonymised demographic and clinical data of patients and transmitted
them to the Principal Investigator (PI) and the Study
Coordinator (SC) within an encrypted electronic database (MS Excel for Mac). Data were centrally collected,
double-checked and analysed with a statistical package (StatPlus for Mac). Only 18+, non-trauma patients
admitted for a surgical emergency during the months of
March–April 2019 and March–April 2020 were analysed.
The final database comprises data of 6263 completely
anonymised patients.
Primary endpoint of the present analysis was to see
whether there was any difference in admissions, diagnoses and treatments during the weekend (Saturday–Sunday) with respect to workdays. In particular, we evaluated
if distribution of demographic and clinical variables (age,
gender, ASA, frailty [3], diagnosis, primary treatment,
surgical access, laparoscopy-to-laparotomy conversion
rate, length of stay, rate of rescue surgery, rate of readmission) changed during weekends versus workdays. The
category "hot gallbladder" includes acute cholecystitis
and intractable biliary colic. The categories "pancreatitis"
and "diverticulitis" include both complicated and noncomplicated acute pancreatitis and acute diverticulitis,
respectively.
Secondary endpoint was to see whether the so-called
weekend effect changed during the COVID-19 pandemic
with respect to the pre-pandemic period. The months
of March and April 2020 were chosen as they represent
the onset of the pandemic. They were compared with the
same 2 months of 2019 to avoid seasonal bias.
Trauma patients, patients < 18 yo and those with more
than 20% of incomplete data were excluded from the
analysis. Factors with more than 10% of missing data
were excluded from the analysis. Missing data were
excluded listwise.
Frequency variables were analysed with the Pearson
Chi-square test and with the 2-way ANalysis-Of-VAriance (ANOVA). Continuous variables were compared
with the Mann–Whitney U test after a first distribution
analysis confirmed non-normal distribution. Statistical
significance was confirmed when p < 0.05.
�Tebala et al. World Journal of Emergency Surgery
(2022) 17:22
Ethical committee approval was not deemed to be necessary as this study is a retrospective audit on completely
anonymised data. The study was endorsed by the Association of Italian Hospital Surgeons (Associazione dei
Chirurghi Ospedalieri Italiani—ACOI) and by the World
Society of Emergency Surgery (WSES).
This paper has been drafted according to the
STrengthening the Reporting of OBservational studies
in Epidemiology (STROBE) checklist [4].
Results
Results are summarised in Tables 1, 2, 3, 4, 5, 6, 7, 8, 9
and 10 and Figs. 1 and 2.
Table 1 Basic characteristics
Total
Workday (Monday–
Friday)
Weekend (Saturday–
Sunday)
4654 (74.3%)
1609 (25.7%)
p
Gender
M
2380
797
F
2274
812
0.267
Age
59.5 ± 20.8
59.2 ± 20.7
0.735
0.825
ASA
1
1104
379
2
1483
519
3
1307
446
4
379
136
5
21
11
Frailty score
1–2
2384
841
>2
2269
768
0.49235
*
2019
2020
2019
2020
1–2
1504
880
556
285
>2
1302
967
448
320
p = 0.00008
p = 0.00116
* Bold indicates distribution of Frailty Score in the two periods of the study
Page 3 of 10
Of the 6263 patients, 74.3% were admitted during the
working days, while only 25.7% were admitted during
the weekends.
Gender distribution, average age, ASA class and distribution of frailty score did not change during the
weekend with respect to working days (Table 1). However, our data showed that the distribution of frailty
score was significantly different between 2019 and
2020, both during weekdays and weekends (Table 1).
The general profile of admissions during the week is
quite constant, but for each day of the week there is an
evident difference in the number of admissions between
March–April 2019 and March–April 2020. This different is pretty much constant for the whole week (Monday − 30.5%,
Tuesday − 35.3%,
Wednesday − 31.7%,
Thursday − 30.7%, Friday − 42.5%, Saturday − 45.2%,
Sunday − 33.4%) (Fig. 1). The average reduction of admissions between 2019 and 2020 was 34.2% during workdays
and 39.7% during weekends (p = 0.143).
The seven most common diagnoses were: (1) hot gallbladder, (2) acute appendicitis, (3) small bowel obstruction (SBO), (4) diverticulitis, (5) complicated inguinal
hernia, (6) pancreatitis, (7) complicated colorectal (CRC)
cancer (Table 2). Their distribution did not show any significant difference between weekends and working days
(Table 2), although the number of admitted hot gallbladders tends to be highest on Mondays and then progressively reduces to become lowest on Sundays (Fig. 2).
The treatment was more frequently surgical in the
patients admitted during weekends (p = 0.037) with
respect to workdays, but the distribution of the three
types of treatments (medical, surgical or interventional) did not show any change between 2019 and 2020
(Table 3).
The surgical access (laparoscopic vs. open) did not
change, but patients admitted during weekends experienced a threefold increased risk of laparoscopy-to-laparotomy conversion (1% vs. 3.4%, p = 0.001). The risk of
conversion was lowest in patients admitted on workdays
during the pandemic (Table 3).
Table 2 Variation of the most frequent diagnoses
Tot
Hot gallbladder
Acute appendicitis
Workday (Monday–Friday)
Weekend (Saturday–Sunday)
2019
2019
2020
2020
p
1148
533
347
168
100
0.5334
983
437
263
184
99
0.4461
SBO
611
266
159
113
73
0.6671
Diverticulitis
403
208
102
60
33
0.6434
Complicated inguinal hernia
309
147
87
52
23
0.3053
Pancreatitis
295
119
93
55
28
0.1116
Complicated CRC
268
117
82
37
32
0.4541
�Tebala et al. World Journal of Emergency Surgery
(2022) 17:22
Page 4 of 10
Table 3 Results
Workday (Monday–Friday)
2019
Weekend (Saturday–Sunday)
2020
2019
p
2020
Primary treatment
Medical
1489 (75.1%) (32.0%)
494 (24.9%) (30.7%)
Surgical
2861 (73.4%) (61.5%)
1035 (26.6%) (64.3%)
0.037
IR/Endo
301 (79.0%) (6.5%)
Medical
875
614
300
80 (21.0%) (5.0%)
194
Surgical
1744
1117
647
388
0.379
IR/Endo
187
114
57
23
0.131
0.441
Surgical access
Laparos
1110 (73.5%) (42.0%)
401 (26.5%) (41.4%)
Open
1522 (73.3%) (57.6%)
553 (26.7%) (57.1%)
0.004
Convert
11 (44.0%) (0.4%)
Laparos
696
414
256
145
0.686
Open
915
607
342
211
0.477
11
0
8
6
Converted
Conversion rate
11/1121 (1.0%)
11/707
Length of stay
14 (56.0%) (1.4%)
14/415 (3.4%)
0/414
8/264
p = 0.011
p = 0.609
7.6 ± 9.9, 5 (0–231)$
8.1 ± 11.4, 5 (0–220)$
7.7 ± 10.7
7.4 ± 8.6
7.9 ± 10.0
p = 0.664
0.013
0.001
6/151
0.033$
8.6 ± 13.5
p = 0.011
Rescue surgery
No
4323 (74.6%) (96.9%)
1468 (25.3%) (95.9%)
Yes
139 (68.8%) (3.1%)
63 (31.2%) (4.1%)
84
55
36
0.061
27
0.659
Readmission
No
4182 (74.1%) (91.1%)
1463 (25.9%) (92.9%)
Yes
408 (78.5%) (8.9%)
112 (21.5%) (7.1%)
265
143
70
0.028
42
0.631
Data presented as absolute number and percentage within row and within column, respectively
$
= Data reported as mean ± standard deviation, median (range); comparison with Mann–Whitney U test
Nonparametric comparison showed that hospital stay
was longer in patients admitted during the weekend
(p = 0.033) and, within this group, it was significantly
longer during the COVID period (Table 3).
The rate of rescue surgery—defined as an operation
performed due to failure of the primary treatment (medical, surgical or endoscopic/interventional)—was not
statistically different in the two groups (workdays vs.
weekends).
Readmission rate was lower in patients admitted during weekends (p = 0.028). No variation was
found in the rate of readmission during weekend versus workdays between 2019 and 2020 (Table 3). An ad
hoc regression analysis was performed to investigate
the relation between risk of readmission and length
of stay (LOS), and this confirmed the presence of a
minimal but significant direct association (risk of readmission = − 2.44862 + 0.00787 * LOS, p = 0.03762). This
finding was confirmed at Pearson’s correlation analysis
(R = 0.029, p = 0.0233).
Subgroup analysis has been performed on the seven
most frequent diagnoses (Tables 4, 5, 6, 7, 8, 9, 10).
Patients with hot gallbladder have been mostly treated
with emergency surgery, but the percentage of those
having an interventional procedure (cholecystostomy)
almost halved during the weekend with respect to workdays. Also, length of stay for patients admitted with hot
gallbladder during the weekend is significantly longer
than for those admitted during workdays. Surgical operations for small bowel obstruction (SBO) were more often
performed by open surgery, but the percentage of those
having a laparoscopic operation was higher during the
�Tebala et al. World Journal of Emergency Surgery
(2022) 17:22
Page 5 of 10
Table 6 Subgroup analysis. Appendicitis
Table 4 Subgroup analysis. Pancreatitis
Workday
(Monday–
Friday)
Weekend
(Saturday–
Sunday)
p
Medical
167 (78.8%)
61 (73.5%)
0.5052
Surgical
32 (15.1%)
14 (16.9%)
IR/Endo
13 (6.1%)
8 (9.6%)
Primary treatment
Workday
(Monday–
Friday)
Weekend
(Saturday–
Sunday)
p
0.8041
Primary treatment
Surgical access
Medical
58 (8.3%)
27 (9.5%)
Surgical
640 (91.4%)
255 (90.1%)
IR/Endo
2 (0.3%)
1 (0.4%)
Laparos
492 (80.8%)
198 (80.5%)
45 (18.3%)
Surgical access
Laparos
23 (85.2%)
13 (86.7%)
0.8954
Open
4 (14.8%)
2 (13.3%)
Open
112 (18.4%)
Converted
0
0
Converted
5 (0.8%)
3 (1.2%)
Conversion rate
0
0
Conversion rate
5/497 (1.0%)
3/201 (1.5%)
0.5850
Length of stay$
7.5 ± 8.9
8.8 ± 13.2
Length of stay$
4.0 ± 3.7
4.4 ± 4.6
0.1176
5 (0–82)
5 (1–79)
3 (0–36)
3 (0–55)
No
160 (70.2%)
68 (84.0%)
Yes
48 (29.8%)
13 (16.0%)
0.8797
Readmission
0.8606
Readmission
0.1885
No
677 (97.4%)
272 (96.5%)
Yes
18 (2.6%)
10 (3.5%)
0.4170
Data presented as absolute number and percentage within column, respectively
Data presented as absolute number and percentage within column, respectively
$
= Data reported as mean ± standard deviation, median (range); comparison
with Mann–Whitney U test
$
Table 5 Subgroup analysis. Hot gallbladder
Table 7 Subgroup analysis. Diverticulitis
Workday
(Monday–
Friday)
Weekend
(Saturday–
Sunday)
p
Medical
252 (28.7%)
86 (32.1%)
0.0157
Surgical
490 (55.8%)
159 (59.3%)
IR/Endo
136 (15.5%)
23 (8.6%)
Primary treatment
Workday
(Monday–
Friday)
Weekend
(Saturday–
Sunday)
p
0.3752
Primary treatment
Surgical access
Medical
184 (59.4%)
48 (51.6%)
Surgical
115 (37.1%)
42 (45.2%)
IR/Endo
11 (3.5%)
3 (3.2%)
Surgical access
Laparos
374 (80.9%)
113 (73.4%)
Open
85 (18.4%)
38 (24.7%)
Converted
= Data reported as mean ± standard deviation, median (range); comparison
with Mann–Whitney U test
0.0774
Laparos
16 (14.3%)
9 (21.4%)
Open
96 (85.7%)
33 (78.6%)
3 (50.0%)
3 (50.0%)
Converted
0
0
Conversion rate
3/377 (0.8%)
3/116 (2.6%)
0.124
Conversion rate
0
0
Length of stay$
6.5 ± 6.6
7.3 ± 7.1
0.0228
Length of stay$
5 (0–67)
5 (0–60)
No
765 (87.8%)
239 (90.5%)
Yes
106 (12.2%)
25 (9.5%)
Readmission
10.0 ± 11.7
9.4 ± 7.6
7 (0–150)
7 (2–42)
0.2843
0.4917
Readmission
0.2290
No
277 (91.4%)
81 (90.0%)
Yes
26 (8.6%)
9 (10.0%)
0.6781
Data presented as absolute number and percentage within column, respectively
Data presented as absolute number and percentage within column, respectively
$
= Data reported as mean ± standard deviation, median (range); comparison
with Mann–Whitney U test
$
weekend. Similarly, conversion rate was significantly
higher during weekends (17.9% vs. 2.4%, p = 0.046). Conversion rate was significantly higher during the weekend
also for the operations for complicated colorectal cancer (18.2% vs. 0, p = 0.031). Patients with complicated
inguinal hernia were almost always treated with open
surgery both during weekends and weekdays, but the rate
of those operated on by laparoscopy was much higher
during weekend (4.2% vs. 0.5%).
= Data reported as mean ± standard deviation, median (range); comparison
with Mann–Whitney U test
�Tebala et al. World Journal of Emergency Surgery
(2022) 17:22
Table 8 Subgroup analysis. Small bowel obstruction
Page 6 of 10
Table 10 Subgroup analysis. Complicated inguinal hernia
Workday
(Monday–
Friday)
Weekend
(Saturday–
Sunday)
p
Medical
170 (40.0%)
64 (34.4%)
0.3827
Surgical
249 (58.6%)
120 (64.5%)
IR/Endo
6 (1.4%)
2 (1.1%)
Primary treatment
Workday
(Monday–
Friday)
Weekend
(Saturday–
Sunday)
p
0.1491
Primary treatment
Surgical access
Medical
17 (7.3%)
2 (2.7%)
Surgical
217 (92.7%)
73 (97.3%)
IR/Endo
0
0
Laparos
1 (0.5%)
3 (4.2%)
69 (95.8%)
Surgical access
Laparos
40 (17.0%)
23 (19.7%)
0.0235
Open
194 (82.6%)
89 (76.1%)
Open
206 (99.5%)
Converted
1 (0.4%)
5 (4.3%)
Converted
0
0
Conversion rate
1/41 (2.4%)
5/28 (17.9%)
0.046
Conversion rate
0
0
Length of stay$
8.6 ± 7.6
8.1 ± 5.8
0.3542
Length of stay$
6.5 (0–58)
7 (0–31)
No
396 (94.5%)
173 (94.0%)
Yes
23 (5.5%)
11 (6.0%)
Readmission
4.4 ± 6.3
4.2 ± 4.2
2 (0–50)
3 (0–25)
0.0235
0.1150
Readmission
0.8105
No
224 (96.1%)
72 (96.0%)
Yes
9 (3.9%)
3 (4.0%)
0.9574
Data presented as absolute number and percentage within column, respectively
Data presented as absolute number and percentage within column, respectively
$
$
= Data reported as mean ± standard deviation, median (range); comparison
with Mann–Whitney U test
Table 9 Subgroup analysis. Complicated colorectal cancer
Workday
(Monday–
Friday)
Weekend
(Saturday–
Sunday)
p
0.3757
Primary treatment
Medical
17 (8.5%)
3 (4.3%)
Surgical
172 (86.4%)
64 (92.7%)
IR/Endo
10 (5.0%)
2 (2.9%)
Surgical access
Laparos
24 (14.8%)
9 (15.3%)
Open
138 (85.2%)
48 (81.4%)
0.0616
Converted
0
2 (3.4%)
Conversion rate
0
2/11 (18.2%)
0.031
13.7 ± 10.8
13.3 ± 14.3
0.3232
11 (1–68)
11 (1–117)
$
Length of stay
Readmission
No
178 (89.9%)
62 (91.2%)
Yes
20 (10.1%)
6 (8.8%)
0.7596
Data presented as absolute number and percentage within column, respectively
$
= Data reported as mean ± standard deviation, median (range); comparison
with Mann–Whitney U test
Discussion
The so-called weekend effect is a much-studied but yet
to be demonstrated and clarified alleged effect claiming that patients admitted and treated during weekends may have different outcomes with respect to those
= Data reported as mean ± standard deviation, median (range); comparison
with Mann–Whitney U test
admitted during normal workdays. Most published
studies using mortality as primary endpoint gave contrasting evidence [5–8]. An increased weekend mortality was demonstrated for laparotomy, adhesiolysis,
colectomy and small bowel resection, but this was due
to patients being in poorer conditions and considered
more urgent than those treated during workdays [9].
On the contrary, an analysis of the UK National Emergency Laparotomy Audit (NELA) database revealed
that quality of care and outcomes for emergency laparotomies did not differ significantly between weekdays
and weekends [4].
We decided not to use mortality as endpoint but analysed some of the factors that can potentially impact on
mortality and morbidity during weekends. In fact, we
wondered whether there was any difference in diagnosis and therapeutical strategy between workdays and
weekends.
Moreover, our secondary aim was to verify whether the
first wave of COVID-19 pandemic, and consequent lockdown, impacted in any way with the eventual differences
of admissions and treatments between workdays and
weekends.
We could not demonstrate any significant difference of
emergency surgical admissions during weekend as compared to workdays. This is quite interesting as we would
have expected that some pathologies, such as pancreatitis, could be more frequent during weekends for cultural
reasons (binge drinking, partying, etc.). This has not been
�Tebala et al. World Journal of Emergency Surgery
(2022) 17:22
Page 7 of 10
700
600
500
400
300
200
100
0
2019 2020
Mon Mon
2019 2020
Tue Tue
2019 2020
Wed Wed
2019 2020
Thu Thu
2019 2020
Fri Fri
2019 2020
Sat Sat
2019 2020
Sun Sun
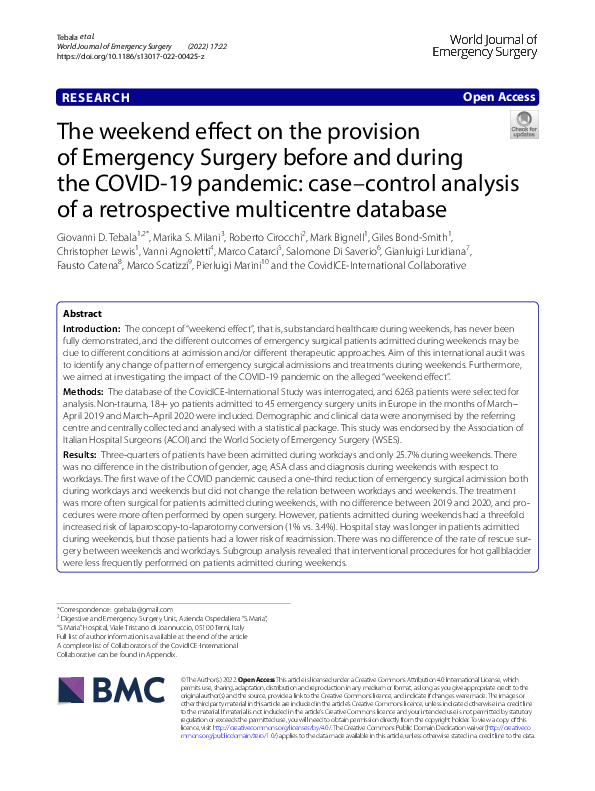
Fig. 1 Admissions by period (March–April 2019 vs. March–April 2020) and day of the week
pancreatitis
hot gallbladder
appendicitis
diverticulitis
SBO
compl CRC
compl inguinal hernia
250
200
150
100
50
0
Mon
Tue
Wed
Thu
Fri
Sat
Sun
Fig. 2 Admissions per day of the week, seven most common diagnoses. The category “hot gallbladder” includes acute cholecystitis and intractable
biliary colic. SBO small bowel obstruction, CRC colorectal cancer
demonstrated, but there is an evident trend for “hot gallbladders”, whose incidence tends to increase on Monday,
probably associated with a less than healthy diet during
weekends. It is possible, but not demonstrated, that the
lockdown effect in 2020 might also have played a role.
However, these differences were not significant, and it
is not unlikely that the profile of admissions for hot gallbladder during the week is only a random effect.
Similarly, we could not demonstrate any difference in
the distribution of ASA classes and frailty scores; that
is, we could not confirm that patients admitted during
weekends are more frail or comorbid. However, a significant difference has been found for both weekdays
and weekends in the rate of frail versus non-frail patients
admitted into the participating surgical units during the
�Tebala et al. World Journal of Emergency Surgery
(2022) 17:22
COVID first wave versus non-COVID period, with more
frail patients admitted during the COVID period (2020).
This finding has already been highlighted and discussed
in another paper [2].
Interestingly, the modalities of treatment changed
significantly during the weekend, probably due to local
availability or reduced adherence to guidance and protocols. In fact, apparently a greater percentage of patients
are treated surgically during weekends with respect to
working days. This may reflect a more severe acute presentation of those patients, but also the lack of availability
of alternative treatments such as interventional radiology
or endoscopy.
Among the patients treated with surgery, most have
been operated on by open surgery and this percentage
did not change during the weekend with respect to working days (57.1% vs. 57.6%), but for some reasons laparoscopic-to-open conversion triples during weekends. This
may be related to more advanced presentations during
weekends but also to the reduced availability of skilled
laparoscopic surgeons in emergency during weekends.
It is also possible that organisation factors played a role,
with the operating surgeons during the weekend trying to
reduce the burden on the already reduced surgical staff
by avoiding long and tedious laparoscopic operations.
It is more difficult to explain why this difference was
more significant on working days during the COVID19 pandemic, when there was no conversion in 2020
with respect to 2019. There is the possibility that official guidelines during COVID suggesting the avoidance
of laparoscopy as much as possible to reduce the risk of
viral transmission through the surgical smoke may have
suggested a more selective application of this technique
to the easiest cases.
Although length of stay was longer for patients admitted during weekends, their readmission rate is significantly lower. To try to clarify this finding, we performed
a regression analysis and a Pearson’s correlation analysis
on the entire series to confirm the initial idea that longer
stay would be associated with reduced risk of readmission. Surprisingly, both analyses showed that there is
a direct correlation (and not inverse as we expected)
between length of stay and risk of readmission, probably
since patients in poorer general conditions had a longer
stay and a higher risk of long-term complications causing
readmission. However, an in-depth analysis of this aspect
is beyond the scope of this work and may require a wider
collection of data.
Zapf et al. found a direct correlation between weekend admission and length of stay, in particular for hot
gallbladders [10]. Our subgroup analysis confirmed this
Page 8 of 10
finding. This may be possibly explained by the fact that
some surgeons (and some units) are not particularly keen
to embark into potentially difficult cholecystectomies
during the weekend and prefer to postpone the difficult
operations to workdays, when subspecialist expertise
may be available.
In actual facts, the treatment of acute cholecystitis may be extremely tricky and may need a multidisciplinary approach. Our analysis showed that the
interventional treatment for acute cholecystitis (cholecystostomy) may not be widely available during the
weekends, hence the reduced percentage of those who
benefit of it.
Interestingly, it seems that the laparoscopic approach
was used more often during weekend for complicated
inguinal hernias and small bowel obstruction. This finding contrasts with the alleged difficulties in performing
emergency laparoscopic surgery off-hours and during
weekends and represents a very good sign of maturity
and flexibility of European health systems. It may be
explained, possibly, by the reduced pressure of elective
surgery, and the consequently more relaxed environment, on Saturdays and Sundays.
Strengths of this study are its multicentric nature and
its large sample. This allowed us to get a reliable snapshot
on the differences in emergency surgical admissions and
treatments in Europe during weekends versus weekdays.
Limitations are its retrospective nature and possibly the
imbalanced distribution of participating units, most of
them being from Italy.
Conclusions
Our analysis demonstrated that (1) there is no significant difference in the distribution of emergency diagnoses between workdays and weekend, other than for hot
gallbladders, (2) there is no difference in the rate of frail
and comorbid patients admitted during workdays with
respect to weekend, (3) the first wave of the COVID-19
pandemic did not impact on the weekdays versus weekend relation, (4) the approach to surgical emergencies
changes significantly during the week end, probably due
to different available skillset and therapeutic capacity,
in particular for hot gallbladders, and this may prolong
the length of stay and reduce the turnover. This may or
may not lead to different outcomes in terms of mortality
and morbidity, but managers and policy-makers should
be aware of this minimal but significant discrepancy to
be able to reshape the emergency surgical services to
meet the need of the population with the same level of
healthcare 7 days a week.
�Tebala et al. World Journal of Emergency Surgery
(2022) 17:22
Appendix: The CovidICE‑International
Collaborative
FRANCE
• Paris: Lo Dico R (PLI)
ITALY
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
Acireale: Stracqualursi A (PLI), Russo G, D’Errico S
Andria: Cianci P (PLI), Restini E, Scialandrone G
Ascoli Piceno: Guercioni G (PLI)
Bari: Martinez G (PLI), Pezzolla A, Altomare DF,
Picciariello A, Trigiante G, Dibra R, Papagni V
Biella: Righetti C (PLI), Polastri R
Brescia: Andreuccetti J (PLI), Pignata G, D’Alessio
R, Arici E, Canfora I
Cagliari: Cillara N (PLI), Deserra A, Sechi R
Castellammare di Stabia: Bianco F (PLI), Gili S,
Cappiello A, Incollingo P
Cattinara: Biloslavo A (PLI), Bellio G, Germani P,
De Manzini N
Cernusco sul Naviglio e Vaprio d’Adda: Buiatti M
(PLI), Paladino FP
Cuneo: Sasia D (PLI), Borghi F, Testa V, Giraudo G,
Allisiardi F, Giuffrida MC
Desio: Gerosa M (PLI), Fogliati A, Maggioni D
Ferrara: Fabbri N (PLI), Feo CV, Bianchini E, Panzini I
Foggia (Chirurgia Generale Ospedaliera): Lizzi V
(PLI), Tricarico FG, Di Gioia G, Melino R
Foggia (Chirurgia Generale Universitaria): Tartaglia
N (PLI), Ambrosi A, Pavone G, Pacilli M, Vovola F
Genova: Belli F (PLI), Barberis A, Azzinnaro A
Grosseto: Coratti A (PLI), Benigni R
La Spezia: Berti S (PLI), Saracco M, Gennai A,
Dova L
Manerbio: Farfaglia R (PLI), Pata G, Arizzi V, Pandolfo G
Milano (Fatebenefratelli-Sacco): Frontali A (PLI),
Danelli P, Ferrario L, Guerci C
Milano (Santi Paolo e Carlo): Mariani NM (PLI),
Pisani Ceretti A, Nicastro V, Opocher E
Modena: Gozzo D (PLI), Casoni Pattacini G
Napoli: Castriconi M (PLI), Amendola A, Gaudiello
M, Palomba G
Page 9 of 10
• Parma: Catena F (PLI), Petracca GL, Perrone G,
Giuffrida M
• Peschiera del Garda: Moretto G (PLI), Impellizzeri
H, Casaril A
• Piacenza: Filosa M (PLI), Caizzone A, Agrusti S,
Cattaneo GM, Capelli P
• Pinerolo: Muratore A (PLI), Calabrò M, Pipitore
Federico N, Cuzzola B, Danna R, Murgese A
• Pisa: Coccolini F (PLI), Pieroni E, Chiarugi M, Tartaglia D
• Pistoia: Giannessi S (PLI), Somigli R, Trafeli M,
Fedi M, De Vincenti R
• Ravenna: Guariniello A (PLI)
• Roma (PTV): Grande M (PLI), Bagaglini G, Pirozzi
B, Guida AM, Ingallinella S, Don CP, Siragusa L,
Capone O, Cerbo D
• Roma (S.Giovanni): Santoro E (PLI), Pende V, Fassari A
• Roma (Sapienza): Mingoli A (PLI), Brachini G,
Cirillo B, Zambon M, Cicerchia P, Meneghini S,
Sapienza P, Puzzovio A, La Torre F
• Roma (UCSC): Fransvea P (PLI), Di Grezia M,
Sganga G
• Salerno: Armellino MF (PLI), Ioia G, Rampone B,
Della Corte M
• Sondrio: Fleres F (PLI), Clarizia G, Bordoni P, Spolini A, Franzini M, Grechi A
• Torino: Suppo M (PLI), Bono D, Scaglione D
• Vimercate: Cotsoglou C (PLI), Paleini S, Chierici
AP
• Zingonia: Uccelli M (PLI), Olmi S, Cesana G
PORTUGAL
• Tras-os-Montes e Alto Douro: Tenreiro N (PLI),
Marcal A, Martins D, Leal C, Vieira B
SPAIN
• Galdakao: Ugarte-Sierra B (PLI), Vincene-Rodriguez I, Duran-Ballesteros M, Sanz-Larrainzar A,
Ibanez-Aguirre FJ
• Saragoza: Yanez-Benites C (PLI), Talal I, Blas JL
�Tebala et al. World Journal of Emergency Surgery
(2022) 17:22
UNITED KINGDOM
• Edinburgh: Garau R (PLI), Clark-Stuart S, Wallace
A, Di Carlo A, Wisnia E, Ehsan K, Beck-Sanders K,
Godson E, Campbell P
• Oxford: Tebala GD (SC), Bignell M (PI), BondSmith G, Lewis C, Ahmad R, Ali R, Aswani SS,
Barza A, Carrillo C, Dawani A, Dey A, Elserafy
A, Gaspar D, Lazzareschi L, Patel M, Shabana A,
Shams M, Shams O, Slack Z
Page 10 of 10
Author details
Surgical Emergency Unit, Oxford University Hospitals NHS Foundation Trust,
Oxford, UK. 2 Digestive and Emergency Surgery Unit, Azienda Ospedaliera
“S.Maria”, “S.Maria” Hospital, Viale Tristano di Joannuccio, 05100 Terni, Italy.
3
Department of General Surgery, Causa Pia Luvini Hospital, Cittiglio, Italy.
4
Department of Anaesthesia and Intensive Care, “M. Bufalini” Hospital, Cesena,
Italy. 5 Department of General Surgery, “S. Pertini” Hospital, Rome, Italy. 6 Department of General Surgery, Madonna del Soccorso Hospital, S.Benedetto del
Tronto, Italy. 7 Department of Oncologic Surgery, “A. Businco” Hospital, Cagliari,
Italy. 8 Department of General and Emergency Surgery, “M. Bufalini” Hospital,
Cesena, Italy. 9 Department of General Surgery, S.Maria Annunziata Hospital,
Florence, Italy. 10 Department of General and Emergency Surgery, S.CamilloForlanini Hospital, Rome, Italy.
1
Received: 13 January 2022 Accepted: 22 April 2022
PI
PLI
SC
Principal Investigator
Principal Local Investigator
Study Coordinator
Availability of data and materials
The dataset generated and analysed during the current study is available from
the corresponding author upon reasonable request.
References
1. NHS England. Seven-day hospital services: the clinical case. 2017. https://
www.england.nhs.uk/seven-day-hospital-services/the-clinical-case. Last
accessed 25/12/21.
2. Tebala GD, Milani M, Bignell M, et al. Emergency surgery admissions and
the COVID-19 pandemic: did the first wave really change our practice?
Results of an ACOI/WSES international retrospective cohort audit on 6263
patients. World J Emerg Surg. 2022;17:8.
3. Rockwood Clinical Frailty Scale. https://www.bgs.org.uk/sites/default/files/
content/attachment/2018-07-05/rockwood_cfs.pdf. Last accessed 12/01/22.
4. von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke
JP, STROBE Initiative. The Strengthening the Reporting of Observational
Studies in Epidemiology (STROBE) statement: guidelines for reporting
observational studies. J Clin Epidemiol. 2008;61:344–9.
5. Nageswaran H, Rajalingam V, Sharma A, Joseph AP, Davies M, Jones
H, Evans M. Mortality for emergency laparotomy is not affected
by the weekend effect: a multicentre study. Ann R Coll Surg Engl.
2019;101:366–72.
6. Gillies MA, Lone NI, Pearse RM, Haddow C, Smyth L, Parks RW, Walsh TS,
Harrison EM. Effect of day of the week on short- and long-term mortality
after emergency general surgery. Br J Surg. 2017;104(7):936–45.
7. Hatchimonji JS, Kaufman EJ, Sharoky CE, Ma LW, Holena DN. A
“weekend effect” in operative emergency general surgery. Am J Surg.
2020;220(1):237–9.
8. Metcalfe D, Castillo-Angeles M, Rios-Diaz AJ, Havens JM, Haider A, Salim
A. Is there a “weekend effect” in emergency general surgery? J Surg Res.
2018;222:219–24. https://doi.org/10.1016/j.jss.2017.10.019.
9. Hoehn RS, Go DE, Dhar VK, Kim Y, Hanseman DJ, Wima K, Shah SA.
Understanding the “weekend effect” for emergency general surgery. J
Gastrointest Surg. 2018;22:321–8.
10. Zapf MAC, Kothari AN, Markossian T, Gupta GN, Blackwell RH, Wai PY,
Weber CE, Driver J, Kuo PC. The “weekend effect” in urgent general operative procedures. Surgery. 2015;158:508–14.
Declarations
Publisher’s Note
Abbreviations
ACOI: Associazione dei Chirurghi Ospedalieri Italiani (Association of Italian
Hospital Surgeons); ANOVA: Analysis of Variance; ASA: American Society
of Anaesthesiologists; CRC: Colorectal cancer; NELA: National Emergency
Laparotomy Audit; PI: Principal Investigator; PLI: Principal Local Investigator;
SBO: Small bowel obstruction; SC: Study Coordinator; STROBE: Strengthening
the Reporting of Observational studies in Epidemiology; WSES: World Society
of Emergency Surgery.
Author contributions
GDT, MSM, RC, MB, GBS, CL, VA, MC, SDS, GL, FC, MS and PM contributed to
conceptualisation and study plan and interpretation of data; GDT was study
coordinator; MB was principal investigator; CovidICE-International Collaborative* was involved in local data collection and anonymisation; GDT, MSM and
MB contributed to central data collection and analysis; GDT, VA, SDS and FC
were involved in WSES relationships; GDT, MC, GL, MS and PM contributed to
ACOI relationships; GDT, MSM and RC were involved in manuscript drafting;
and all authors including the CovidICE-International Collaborative contributed
to manuscript final version approval. All authors read and approved the final
manuscript.
Funding
No funding was available for this study.
Ethics approval and consent to participate
Formal ethical committee approval was not deemed to be necessary due
to the retrospective nature and anonymised nature of the audit. However,
the study was approved by the Comitato Etico ATS Sardegna on 22.12.2020
and was sponsored by the World Society of Emergency Surgery and by the
Associazione dei Chirurghi Ospedalieri Italiani.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests. All authors certify
that they have no affiliations with or involvement in any organisation or entity
with any financial or non-financial interest in the subject matter or materials
discussed in this manuscript.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
�
 A. Marcal
A. Marcal