ORIGINAL ARTICLE
Medycyna Ogólna i Nauki o Zdrowiu, 2019, Tom 25, Nr 1, 27–32
www.monz.pl
Perception of European nurses of
culturally-appropriate health care –
a cross-sectional study
Martin Červený1, Leilani A. Siaki2, Paula McGee3, Mária Kilíková1
1
Department of Health Sciences, St. Elizabeth University of Health and Social Sciences, Bratislava, Slovak Republic
Center for Nursing Science and Clinical Inquiry, Madigan Army Medical Center, United States
3
Birmingham City University, United Kingdom
2
Červený M, Siaki A, McGee P, Kilíková M. Perception of European nurses of culturally-appropriate health care – a cross-sectional study. Med
Og Nauk Zdr. 2019; 25(1): 27–32. doi: 10.26444/monz/102392
Abstract
Introduction and objective. Increased migration within Europe is leading to rapid population changes in every country.
Nurses increasingly care for patients with whom they do not share a common culture or language. The aim of this study is
to ascertain nurses’ perceptions of difficulties in providing culturally appropriate care.
Materials and method. Survey questions derived from the literature were translated from Slovak into 5 languages, then
distributed to nurses in 25 European States. The survey sample consisted of 1,264 respondents from 25 European countries.
Statistical analysis was performed by IBM SPSS version 18.
Results. Over 60% of nurses regularly cared for patients from different cultures. 70.6% of nurses declared challenges during
nursing care for patients from different culture. The main challenges were language, religion, and lack of cultural knowledge.
Statistical significance was demonstrated in terms of the preparedness of nurses to provide culturally appropriate care.
Multilingual nurses were statistically significantly better prepared for nursing care of patients from other cultures.
Conclusions. Despite existing standards and guidelines, nurses working in European countries who regularly care for migrant
populations do not perceive themselves to be adequately prepared to deliver culturally appropriate care. A multifaceted
approach that includes policymakers, educators, and clinicians is needed. This study highlights the challenges experienced
by nurses in Europe which can be informative for educational programmes for nurses and other healthcare professionals.
Key words
culturally competent care, Europe, transcultural nursing, challenges
INTRODUCTION
Increased migration within and into Europe is transforming
the population of every country in the region. The Schengen
Agreement, which came into force in 1995, allows the free
movement of European Union (EU) nationals between
most member states [1]. Refugees fleeing conflict zones,
persecution and disaster areas, as well as economic migrants
seeking better opportunities, have all contributed to
inward migration into European states. Consequently, even
countries with little previous history of immigration have
increasingly diverse populations whose members originate
from different parts of the world. These population changes
pose challenges for healthcare providers. For example,
effective communication and providing appropriate care is
very difficult when patients and professionals do not share
a common language or cultural background [2, 3].
Research focused on health inequalities conducted by
the European Union Agency for Fundamental Rights
(FRA) [4] revealed enormous deficiencies in the following
areas: multidimensional inequality in health care
provision, discrimination against ethnic minority patients,
misinformation about patients from other cultures, lack
of accessible interpreters in health care facilities, and
Address for correspondence: Martin Červený, Department of Health Sciences,
St. Elizabeth University of Health and Social Sciences, Bratislava, Kósu Schoppera 22,
048 01, Rožňava, Slovak Republic
E-mail: m.cerveny.m@gmail.com
Received: 16 November 2018; Accepte: 28 December 2018
unpreparedness of healthcare professionals to cope with
patients from diverse cultural backgrounds.
In 2015, an international work group of transcultural
nursing experts developed the American Nurses Association’s
(ANA) first Standard for Culturally Congruent Practice, and
prompted a “Call to Action” for registered nurses worldwide
[5]. In the call, there was included a recommendation for
nurses to become knowledgeable about existing standards
and guidelines and evaluate and implement culturally
congruent care in their practice. Education in transcultural
nursing within the common European Economic Area (EEA)
is governed by the 2013/55 / EU Directive. However, this
directive does not specify the subject’s curriculum [6].
This study reports the results of a survey completed
by nurses from 25 European countries regarding their
perceptions of the issues involved in caring for patients
from culturally diverse backgrounds.
Theoretical framework of transcultural nursing. Madeleine
Leininger pioneered the field of transcultural nursing; her
theory of Culture Care Diversity and Universality, and
the Sunrise Enabler are based on the concepts of holistic
health, i.e. bio-psycho-social and spiritual well-being.
Among the major tenets of Leininger’s theory that inform
about interactions with patients from different cultures, are
health, culture, culture care, culture care and social structure
dimensions, as well as worldview [7, 8].
According to Leininger, health is “a state of well-being that is
culturally defined and constituted” [9], a state in which people
�28
Medycyna Ogólna i Nauki o Zdrowiu, 2019, Tom 25, Nr 1
Martin Červený, Leilani A. Siaki, Paula McGee, Mária Kilíková. Perception of European nurses of culturally-appropriate health care – a cross-sectional study
are capable of carrying out everyday activities. Enabling
others to achieve this state requires nurses to understand
the socio-cultural factors that define, influence and drive
health. Examples include religious and philosophical ideas,
economics, education, technology, political, and legal factors.
Language is a particularly important issue with regard to
health and health care. Clear communications between health
professionals and health consumers is crucial. In addition
to Leininger, transcultural nursing knowledge was further
developed by other theoreticians, like Davidhizar, Giger [10],
Campinha-Bacote [11], Purnell [12], Papadopoulos, Tilki and
Taylor [13]. These more recent theoreticians have expanded
the field and developed educative tools to enhance nurses’
ability to care for patients of diverse cultures. However, gaps
remain.
Historically, the preparedness of nurses in Europe to care
for patients from different cultures may be linked to recent
immigration trends. Kačorová et al. [14] divided European
countries into 3 groups. The first group consisted of countries
with a long history of contacts with diverse cultures via
former colonial empires: Portugal, Spain, France and the
UK. The second group consisted of countries which became
multicultural due to migration trends after the Second World
War. This group included the Scandinavian countries [15,
16] and Switzerland [14]. The third group included countries
with little or no previous experience with immigration. These
included countries in Eastern Europe and Ireland where the
transformation from a mono-cultural to a multicultural
society brought about recent dramatic changes [17].
OBJECTIVE
European inward migration poses challenges for nurses who
may not share a common language or cultural background
with the patients for whom they provide care. The aim
of this survey was to explore clinical nurses’ perception
of challenges that prevented or hindered the provision of
culturally appropriate care.
MATERIALS AND METHOD
This study was descriptive, cross-sectional and involved
European nurses directly involved in clinical practice.
Nurses were surveyed across the European Union (EU)
which consists of 28 countries, with a population of over 510
million, and includes many diverse languages and cultures.
Consequently, a survey seemed to offer the best method of
reaching a large sample of nurses. The limitations of survey
research were recognized. For example, the reliability of
methods of distribution may vary. People may not respond,
may not complete the task fully or may pass questionnaires to
others for completion. However, the survey method was used
as this method is easily distributed, less time consuming, and
the results can be processed objectively.
The questionnaire was developed specifically for this
study. Developing the questionnaire began with a review
of pertinent literature focused on transcultural nursing
and the challenges health care providers encounter when
delivering culturally appropriate care. Questions were
developed, in the Slovak language, based on the outcomes
of this review.
Once the questionnaire was finalised in the Slovak
language, it was translated into the English, German,
Hungarian, Polish and Italian languages. Translations were
conducted by professional translators who spoke Slovak
and had relevant certifications for one or more of the target
languages.
The process included two independent translations from
which the final version was created. This was subsequently
back-translated into the source language, and compared
with the original Slovak version. In the second phase,
questionnaires in foreign languages were validated by using
piloting. Two native speakers in English, German, Polish,
Hungarian and Italian languages were invited to pilot the
testing of the translated questionnaires. Changes were
made to the questionnaire based on the findings from the
pilot study. The most mistakes were found in the German
questionnaire, for example, questionnaires were translated
according to the grammar rules. Despite this, native
speakers showed that they understood what was written
in the german questionnaries yet hinted that it was written
convolutedly.
The questionnaire contained six questions. Questions in
the final version were organised around four topics.
Demographics. These included the geographic location of
the respondents.
Interaction between nurses and patients from different
cultures. With the focus on how frequently respondents
cared for patients from cultures other than their own, and
how often they experienced challenges when caring for
patients from different cultures.
Challenges in nursing patients from different cultures.
Examples in this topic included religion, language, lack of
knowledge about culture prejudice against patients from
other cultures, patients’ distrust of the health care and the
patient’s special needs. For the subjective evaluation of the
challenges, the respondent had the opportunity to express
their opinion on 4-step Likert scale: highly occurring,
substantially occurring, a less significant challenge or no
challenge.
Subjective view of preparedness of nurses to deliver
culturally appropriate health care. These questions focused
on the preparation of nurses and whether they perceived
culturally appropriate care. The last two questions in the
questionnaire were addressed to respondents who already
had 10 or more years of nursing practice. To determine the
subjective evaluation, a 5-step Likert scale was used, ranging
from 1 – indicating not ready, to 5 – indicating maximum
readiness.
Sample and distribution of the questionnaire. Recruitment
began with emails to local nursing organizations or
associations in each country. If the response was positive,
further work was maintained with a local contact in that
country. If this was not possible, the researchers attempted
to contact other organizations, nursing publications and
individuals in the country concerned. These contacts were
then asked to send e-questionnaires to their professional
colleagues via email. A professional colleague was defined
as an individual currently working as a nurse in any setting
�29
Medycyna Ogólna i Nauki o Zdrowiu, 2019, Tom 25, Nr 1
Martin Červený, Leilani A. Siaki, Paula McGee, Mária Kilíková. Perception of European nurses of culturally-appropriate health care – a cross-sectional study
(e.g. hospital, school, outpatient clinic) either full or part
time. The sample for this study consisted of 1,264 respondents
from 25 European countries.
Ethical considerations. All ethical principles outlined by
the World Medical Association [18] were adhered to. The
participants were given information regarding the purpose
and voluntary, anonymous nature of this survey. Completion
of the questionnaire was considered consent. No personally
identifiable data or health information was collected.
Data analysis. For analysis of the answers obtained from
questionnaires, the following statistical methods were
applied: Descriptive statistics, Mann Whitney U test (for 2
independent variables) and Kruskal Wallis test – One-way
ANOVA (for more than 2 independent variables – number
of languages, territory of respondent, types of challenges).
Statistical analysis was performed by statistical package IBM
SPSS version 18.
RESULTS
The number of valid questionnaires received according to
country is summarized in Table 1. The largest number of
responses were received from Central Europe (n=762), the
least from Western Europe (n=59). The mean number of
respondents› years in clinical practice was 14.41 years.
Interactions among nurses and patients from different
cultures. Respondents were asked how frequently they cared
for patients from cultures other than their own. Responses
showed that 36.16% did so every day, 19.94% once a week,
and a further 25.08% at least once a month. Only 1.74% stated
that they had never provided nursing care for a patient of
different culture.
Challenges in nursing patients from different cultures.
Respondents were asked about whether cultural differences
between nurses and patients affected the provision of nursing
care. Responses differed. A total of 28.96% stated that there
were no challenges. However, 38.13% reported some minor
difficulties and 32.91% reported major problems. These
problems were attributed to language challenges (44.9%),
lack of knowledge about other cultures (35.19%), patients’
religious beliefs (30.18%), and nurses’ preconceptions about
patients from other cultures (26.50%). However, the degree
to which these were thought to affect nursing care varied
considerably. Results are listed in Table 2.
Differences in perception of challenges across European
territories. In this survey, 895 respondents (70.9%) from 1,264
respondents perceived challenges when caring for patients
from different cultures. Results of testing for significance with
differences in types of challenges are summarized in Table 2.
Table 2. Differences in perception of types of challenges across the
European territories
Kruskal-Wallis test
(p-value)
Table 1. Number of respondents from European countries
European territory
Northern Europe
Western Europe
Middle Europe
Southern Europe
Lack of knowledge about culture is the same across
European territories
0.0001
1 (0.08)
Patient’s religious beliefs is the same across European
territories
0.0001
Country
n (%)
Denmark
54 (4.27)
Finland
Iceland
80 (6.33)
Language challenges are the same across European territories
0.001
Norway
1 (0.08)
Sweden
69 (5.46)
Nurses’ preconceptions are the same across European
territories
0.004
Accessibility of health care is the same across European
territories
0.117
Distrust to health care is the same across European territories
0.0001
Demands of patient to special satisfying are the same across
European territories
0.0001
Belgium
2 (0.16)
United Kingdom
38 (3.01)
Ireland
16 (1.26)
The Netherlands
3 (0.24)
Austria
119 (9.41)
Czech Republic
114 (9.02)
Germany
166 (13.13)
Hungary
122 (9.65)
Poland
117 (9.25)
Slovakia
123 (9.73)
Switzerland
1 (0.08)
Andorra
1 (0.08)
Croatia
2 (0.16)
Cyprus
1 (0.08)
Greece
3 (0.24)
Italy
217 (17.17)
Malta
3 (0.24)
Portugal
1 (0.08)
Slovenia
2 (0.16)
Spain
8 (0.63)
Differences in perception of challenges were statistically
significant across European territories, with the exception
of accessibility to health care (p = 0.117).
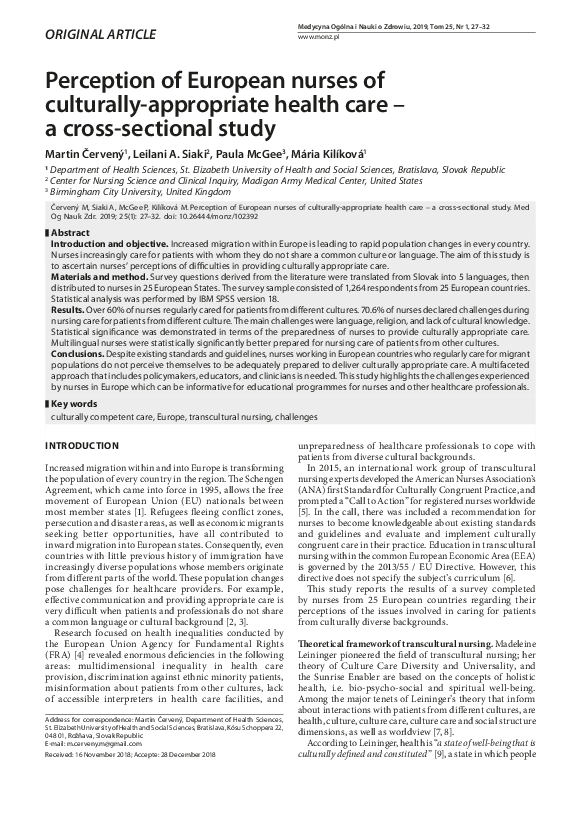
Subjective view of nurses’ preparedness to deliver culturally
appropriate care across European territories. Statistically
significant differences were found in the preparedness of
nurses among European territories. Nurses from Western,
Northern and Southern Europe were better prepared for
nursing care for patients from other countries, compared
with Central Europe (Tab. 3).
Preparedness of nursing staff regarding knowledge of
languages 10 years ago, and at the time of their study, was
the same (p= 0.55). The preparedness 10 years ago and at the
present time show statistically significant differences across
European territories (0.001). Results of this study indicate
that preparedness depends on the number of languages
(p=0.001).
�30
Medycyna Ogólna i Nauki o Zdrowiu, 2019, Tom 25, Nr 1
Martin Červený, Leilani A. Siaki, Paula McGee, Mária Kilíková. Perception of European nurses of culturally-appropriate health care – a cross-sectional study
Table 3. Subjective preparedness of nurses to care for patients according
to the number of languages and across European territories
Table 4. Duration of practice and perception of preparedness and
challenges
Kruskal-Wallis test
(p-value)
Mann-Whitney test
(p-value)
Previous preparedness of respondents (10 years ago) was the
same across the number of languages
0.550
Grading challenges in nursing is the same across duration of
respondent practice
0.94
Current preparedness of respondents is the same across the
number of languages
0.001
Previous preparedness of nurses (10 years ago) is the same
as duration of respondent practice
0.12
Previous preparedness of respondents (10 years ago) was the
same across European territories
0.001
Current preparedness in nursing is the same across duration
of respondent practice
0.42
Current preparedness of respondents is the same across
European territories
0.001
The graphical presentation of testing according to
territories (item 3) is demonstrated in Figure 1 and, according
to the number of languages, in Figure 2.
Figure 1 Current preparedness for nursing patients from different culture across
European territories (p = 0.001)
Figure 2. Current preparedness for nursing patients from different cultures
according to number of languages (p = 0.001)
Testing the influence of duration of practice for challenges
and perceived preparedness. No differences were found in
the perception of preparedness or challenges according to
duration of practice (Tab. 4).
DISCUSSION
This study explored the challenges encountered by European
nurses when caring for patients from different cultural
backgrounds, aided by Leininger’s transcultural nursing
theory. The results showed that across Europe, nurses
encountered 3 main challenges: language, religion, and
cultural knowledge. Nurses’ preconceptions about patients
from diverse cultures also affected the provision of nursing
care. Ethnocentric feelings or stereotypes complicated the
delivery of care to patients from other cultures [19]. It was
found that lack of a shared language was a major factor
affecting patient care. This finding is consistent with those
of previous studies. For example, Kuševova [20] found that
language challenges were the most significant problem in
providing nursing care for patients in asylum camps. Ryska
and Botíková [21] found that language challenges deterred
nurses from working with patients from other cultures.
Inadequate culturally appropriate care is known to
contribute to healthcare disparities and suboptimal
outcomes, particularly among vulnerable populations, such
as immigrants. While research in this area remains limited,
progress is being made [22, 5]. Research [15] undertaken in
Sweden focused on nurses’ interactions with children from
diverse cultures. Findings showed that the nurses lacked
knowledge about the children’s culture, which resulted
in educational courses directed at providing culturally
appropriate care. Healthcare professionals from Ireland were
not adequately prepared for problems they encountered while
treating patients from another culture. Due to research and
identified deficiencies, the Irish government implemented
several educational activities [17]. In their study, Ruddock and
Turner [23] found that despite the rise of multiculturalism in
Denmark, their health education and health system stayed
mono-cultural. Hart and Mareno [24] reported that nurses
expressed their frustration about their inability to work
within professional standards, along with limited resources,
to address the individual needs of a growing population of
migrant patients in a south-eastern state of the USA.
The aim of this survey was to discover how nurses perceive
culture-appropriate care for patients from different cultures.
The current migration of people in the European Union
is affecting all Member States. This survey statistically
demonstrates that sessions with more language skills have
experienced less subjective challenges in treating a patient
from a different culture. It was also noted that there is
a statistically significant difference in the current readiness
of nurses from Western, Northern and Southern Europe
to Central Europe, to nursing care in patients from other
cultures. Further, based on the results of statistical testing,
�Medycyna Ogólna i Nauki o Zdrowiu, 2019, Tom 25, Nr 1
Martin Červený, Leilani A. Siaki, Paula McGee, Mária Kilíková. Perception of European nurses of culturally-appropriate health care – a cross-sectional study
it can also be concluded that differences in perception of
challenges are statistically significant across European
regions, with the exception of accessibility to health care.
Implications for Nursing & Health Policy. Culturallyappropriate care conveys respect for persons, impacts
health disparities, and improves health outcomes [22, 5].
However, the provision of nursing care for patients from
different cultures is very demanding. Not every nurse or
healthcare provider is able to meet these demands. Based on
the results of this study, it is recommended that nurses apply
theoretical concepts found in the Theory of Culture Care
Diversity and Universality, or other transcultural theories,
when developing healthcare interventions. For policy makers
and healthcare leaders, the following are recommended: a)
implementing training programmes focused on providing
culturally appropriate care; b) supporting the development
of international cooperation in research projects for this
field; and c) supporting development of readily available
healthcare-focused language courses.
The results from this study are in alignment with the
ANA’s Standard 8, and underlines the recommendations in
the Call to Action.
Limitations of the study. Several limitations were identified
in this study. Not all countries within the EU were
represented. Less than 10 responses were received from about
half of the participating countries, limiting generalization.
The immigration status of respondents themselves was
unknown, potentially impacting on the results. The results
highlight some of the challenges in attempting to survey
nurses across the EU which comprises twenty-eight countries
and an increasing number of languages. There is no single
mechanism through which nurses can be contacted as part of
research projects. The International Council of Nurses, based
in Geneva, is a member organization for nursing associations
worldwide; however, not every country is a member, even in
the EU, and not all nurses are members of their country’s
nursing organization. Additionally, the specific type, length,
and methods of cultural competence training received, were
not collected.
The questionnaire used was developed specifically for
this study and translated into multiple languages. While
questions were based on relevant literature, more research
is needed to determine the reliability and validity of
the instrument. It is planned to repeat this study in the
future to include respondents from all EU Member
States. Also under consideration is whether to expand the
demographic questions to include the immigration status of
the nurses themselves, and questions about actual training
received.
CONCLUSIONS
Despite existing standards and guidelines, nurses working
in European countries who regularly care for migrant
populations do not perceive themselves to be adequately
prepared to deliver culturally-appropriate care. More
research is needed to evaluate current training programmes,
determine what gaps exist, and how best to address these
gaps. A multifaceted approach that includes policymakers,
educators, and clinicians is needed.
31
Conflict of Interests
The authors declare that there are no conflicts of interest.
Disclaimer: The views expressed in this presentation are
those of the author(s) and do not reflect the official policy
or position of the Department of the Army, Department of
the Defense, or the US Government
Acknowledgement
First of all, I would like to express my gratitude to co-authors
Leilani A. Siaki, Paula McGee, and Maria Kilíková. This article
could not be published without your support. Furthermore,
I would like to express my gratitude to the doc. PhDr. Lucia
Dimunová, PhD. for her supporting consultations, critical
contribution, and to the doc. RNDr. Pavel Matula, CSc. for his
technical cooperation in the statistical elaboration of outputs.
REFERENCES
1. Eurostat. EU population up to almost 512 million at 1 January
2017. http:// c.europa.eu/eurostat/documents/2995521/8102195/310072017-AP-EN.pdf/a61ce1ca-1efd-41df-86a2-bb495daabdab. (access:
2018.10.12).
2. Klímová M, Rosková L. The economic consequences of the contemporary
European migration crisis on the Czech Republic. Kontakt. 2017; 19(4):
e253–e262; http://dx.doi.org/10.1016/j.kontakt.2017.09.011.
3. World Health Organization. [Closing the Gap in a generation: health
equity through action on the social determinants of health. Final report
of the Commission on Social Determinants of Health]. http://apps.who.
int/iris/bitstream/handle/10665/69832/WHO_IER_CSDH_08.1_slo.pd
f;jsessionid=439B2DFB0B44EEA9AFDF3D67CBF79977?sequence=8
(access: 2018.10.11). Slovak
4. European union agency for fundamental rights. Inequalities and
multiple discrimination in access to and quality of healthcare.
Luxembourg: Publications Office of the European Union; 2013.
5. Marion L, Douglas M, Lavin M, Barr N, Gazaway S, Thomas L, Bickford
C. Implementing the New ANA Standard 8: Culturally Congruent
Practice. OJIN. 2016; 22(1): 9. doi: 10.3912/OJIN.Vol22No01PPT20.
6. European Parlament. Directive 2013/55/EU of the European Parliament
and of the Council of 20 November 2013 amending Directive 2005/36/
EC on the recognition of professional qualifications and Regulation (EU)
No 1024/2012. Official Journal of the European Union. 2013; 56(12):
L354. doi: 10.3000/19770677.L_2013.354.eng.
7. Leininger M, McFarland MR. Culture Care Diversity and Universality:
a Worldwide Nursing Theory, 2nd ed. Sudbury (MA) Jones and Bartlett
Publishers, 2006.
8. Červený M. [The fundamental concepts of transcultural nursing].
Nővér. 2016; 29(5): 1–44. Hungarian.
9. McFarland M, Wehbe-Alamah H. Leininger´s Culture Care Diversity
and Universality: a Wordwide Nursing Theory. 3rd ed. Boston (MA)
Jones & Bartlett, 2015.
10. Giger NJ. Transcultural Nursing: Assessment and Intervention. 7th ed.
St. Louis (MO) Elsevier, 2017.
11. Campinha-Bacote, J. The process of cultural competence in the delivery
of health care services: A culturally competent model of care. 3rd ed.
Cincinnati (OH) Transcultural C.A.R.E. Associates, 1998.
12. Purnell L, Paulanka, B. Transcultural healthcare: A culturally competent
approach (3rd ed.). Philadelphia (PA) Davis Company, 2008.
13. Papadopoulos I. Culturally Competent Compassion: A guide for
healthcare students and practitioners. London (UK) Routledge Books,
2018.
14. Kačorová J, Hlubková Z, Heiderová H. [European view of transcultural
nursing]. In: [Quo vadis heath service. Proceedings of the scientific
and professional conference with international participation] Prešov:
Fakulta zdravotníckych odborov Prešovské univerzity v Prešove; 2012.
p. 95–105. Slovak.
15. Berlin A, Törnkvist L, Hylander I. Watchfully checking rapport with
the Primary Child Health Care nurses – a theoretical model from the
perspective of parents of foreign origin. BMC Nursing. 2010; 9(1): 1–10.
doi: 10.1186/1472-6955-9-14.
16. Wikberg A, Eriksson K. Intercultural caring. An abductive model. Scand J
Caring Sci. 2008; 22(3): 485–96. doi: 10.1111/j.1471-6712.2007.00555.x.
�32
Medycyna Ogólna i Nauki o Zdrowiu, 2019, Tom 25, Nr 1
Martin Červený, Leilani A. Siaki, Paula McGee, Mária Kilíková. Perception of European nurses of culturally-appropriate health care – a cross-sectional study
17. Tuohy D, McCarthy J, Cassidy I, Graham, MM. Educational needs of
nurses when nursing people of a different culture in Ireland. Int Nurs
Rev. 2008; 55(2): 164–70. doi: 10.1111/j.1466-7657.2007.00600.x.
18. World Medical Association. Declaration of Helsinki Ethical Principles
for Medical Research Involving Human Subjects. JAMA. 2013; 310(20):
2191–2194. doi: 10.1001/jama.2013.281053.
19. Almutairi FA, Aldan AA, Nasim M. Perceptions of the critical cultural
competence of registered nurses in Canada. BMC Nursing. 2017; 16:47
doi: 10.1186/s12912-017-0242-2.
20. Kuševová S. [The role of a nurse in asylum center]. In. [The 1-st
International Science Conference, Multicultural Dialogue in Assisting
Professions 2012. Together in Diversity]. Bratislava: VŠZaSP sv. Alžbety;
2012. p. 149–153. Slovak.
21. Ryska M, Botíková A. [Nursing in theory and practice]. Praha (CZ)
Ottova tiskárna, 2011. Slovak.
22. Gallagher RW, Polanin JR. A meta-analysis of educational interventions
designed to enhance cultural competence in professional nurses and
nursing students. Nurse Educ Today. 2014; 35(2): 333–40. doi: 10.1016/j.
nedt.2014.10.021.
23. Ruddock HC, Turner S. Developing Cultural Sensitivity: Nursing
students ‘experiences of Study Abroad Programme. J Adv Nurs. 2007;
59(4): 361–369. doi:10.1111/j.1365–2648.2007. 04312.x.
24. Hart PL, Mareno N. Cultural challenges and barriers through the voices
of nurses. J Clin Nurs. 2014; 23(15–16): 2223–32. doi:10.1111/jocn.12500.
Postrzeganie odpowiedniej kulturowo opieki zdrowotnej
przez europejskie pielęgniarki – badanie przekrojowe
Streszczenie
Wprowadzenie i cel. Nasilająca się w Europie migracja prowadzi do gwałtownych zmian populacyjnych w każdym z krajów.
Coraz częściej pielęgniarki opiekują się pacjentami, z którymi nie dzielą wspólnej kultury i języka. Celem badania było
ustalenie postrzegania przez pielęgniarki problemów w zapewnieniu odpowiedniej kulturowo opieki.
Materiały i metody. Pytania kwestionariusza wywiadu pochodzące z literatury przetłumaczono z języka słowackiego na
5 języków i rozdano pielęgniarkom w 25 krajach europejskich. Badanie ankietowe objęło 1264 respondentów z 25 krajów
europejskich. Analizę statystyczną przeprowadzono za pomocą oprogramowania IBM SPSS wersja 18.
Wyniki. Ponad 60% pielęgniarek regularnie świadczyło opiekę pacjentom pochodzącym z różnych kultur. 70,6% pielęgniarek
zgłosiło problemy podczas opieki pielęgniarskiej nad pacjentami pochodzącymi z innych kultur. Główne wyzwania związane
były z językiem, religią i brakiem wiedzy kulturowej. Wykazano istotne różnice statystyczne w zakresie przygotowania
pielęgniarek do świadczenia opieki odpowiedniej kulturowo. Wielojęzyczne pielęgniarki były statystycznie istotnie lepiej
przygotowane do opieki pielęgniarskiej nad pacjentami z innych kultur niż te, które posługiwały się tylko własnym językiem
ojczystym.
Wnioski. Wbrew istniejącym standardom i wytycznym, pielęgniarki pracujące w krajach europejskich, które regularnie
opiekują się migrantami, nie uważają, że są odpowiednio przygotowane do świadczenia odpowiedniej kulturowo opieki.
Niezbędne jest wieloaspektowe podejście obejmujące decydentów, dydaktyków i klinicystów. Badanie to podkreśla
wyzwania, przed jakimi stoją pielęgniarki w Europie i może dostarczyć informacji przydatnych przy opracowywaniu
programów edukacyjnych dla pielęgniarek i innych pracowników opieki zdrowotnej.
Słowa kluczowe
opieka kompetentna kulturowo, Europa, transkulturowa opieka pielęgniarska, wyzwania
�
 Leilani Siaki
Leilani Siaki