NCP Gouty Arthritis
NCP Gouty Arthritis
Download as doc, pdf, or txt
At a glance
Powered by AI
The document discusses several common nursing diagnoses like acute pain, anxiety, weakness and proposes nursing care plans to address them. It outlines problems, nursing diagnoses, objectives, interventions and expected outcomes.
Common nursing diagnoses discussed include acute pain, mild anxiety, weakness and anxiety related to lack of knowledge about the disease condition.
Some nursing interventions mentioned are assessing vital signs, administering analgesics, teaching deep breathing exercises, encouraging diversional activities and patient education.
You might also like
- Feeling Unreal - Depersonalization Disorder and The Loss of The SelfDocument253 pagesFeeling Unreal - Depersonalization Disorder and The Loss of The SelfJo F. Teichmann100% (3)
- Neuropsychological Rehabilitation The International Handbook by Barbara A. Wilson Et Al. (Eds.)Document69 pagesNeuropsychological Rehabilitation The International Handbook by Barbara A. Wilson Et Al. (Eds.)Ana Jiménez Jiménez100% (1)
- Case Scenario: Prostate CancerDocument5 pagesCase Scenario: Prostate Cancer24 PAULINO ALDRIN MUJARNo ratings yet
- Epilepsy (Gregory D. Cascino, Joseph I. Sirven Etc.)Document514 pagesEpilepsy (Gregory D. Cascino, Joseph I. Sirven Etc.)Georgiana Frunza100% (3)
- NCP - Altered ComfortDocument2 pagesNCP - Altered ComfortJhudiel Gabriel Go0% (1)
- 217 RF Peripheral Neurovascular DysfunctionDocument8 pages217 RF Peripheral Neurovascular Dysfunctionapi-271775750No ratings yet
- Gouty Arthritis-NcpDocument2 pagesGouty Arthritis-NcpJohn D100% (2)
- NCP Post Op PainDocument2 pagesNCP Post Op PainLiz Liwag0% (1)
- COLLEGE OF ST. JOHN - ROXAS Member: Association ofDocument6 pagesCOLLEGE OF ST. JOHN - ROXAS Member: Association ofCrisha Ann Billones BacutaNo ratings yet
- The Philippine Health Care Delivery SystemDocument19 pagesThe Philippine Health Care Delivery SystemArianne Kamille AndesNo ratings yet
- NCP Cushing's SyndromeDocument2 pagesNCP Cushing's SyndromeChristine LebicoNo ratings yet
- NCP ImmobilityDocument2 pagesNCP Immobilityxxxcamzxxx67% (6)
- Cues Nursing Diagnosis Scientific Reason Objective Nursing Intervention Rationale EvaluationDocument4 pagesCues Nursing Diagnosis Scientific Reason Objective Nursing Intervention Rationale Evaluationjomsportg0% (1)
- NCP Loss of AppetiteDocument5 pagesNCP Loss of AppetiteStenneli Gumban Trojillo50% (2)
- NCP Breast CADocument3 pagesNCP Breast CAHannah Lacambra100% (1)
- NCP MCMC Post OperativeDocument3 pagesNCP MCMC Post OperativeKristiyanong KabataanNo ratings yet
- NCP - EdemaDocument1 pageNCP - Edemavipncpusers100% (1)
- Assessment Healt H Patte RN Nursing Diagnosis Desired Outcome (Edit) Intervention (Edit) Evaluation (EDIT) Rema RKSDocument3 pagesAssessment Healt H Patte RN Nursing Diagnosis Desired Outcome (Edit) Intervention (Edit) Evaluation (EDIT) Rema RKStflorenzNo ratings yet
- Fatigue Related To Autoimmune Disease As Evidenced by Patient Inability To Maintain Usual Level of Physical ActivityDocument5 pagesFatigue Related To Autoimmune Disease As Evidenced by Patient Inability To Maintain Usual Level of Physical ActivityJordz PlaciNo ratings yet
- NCP Impaired SkinDocument2 pagesNCP Impaired Skinarjay2306_obcq100% (1)
- NCP GastroenteritisDocument1 pageNCP GastroenteritisFranchesca PaunganNo ratings yet
- NCP 2Document3 pagesNCP 2klawdin100% (1)
- Impaired Verbal CommunicationDocument3 pagesImpaired Verbal CommunicationCalimlim KimNo ratings yet
- NCP Alteration ComfortDocument2 pagesNCP Alteration Comforttinea nigraNo ratings yet
- NCP PpwardDocument15 pagesNCP PpwardKarl Vincent Soso100% (1)
- NCP Ineffective Breathing GunshotDocument3 pagesNCP Ineffective Breathing GunshotMikko Enoc100% (1)
- Nursing Care Plans For AppendicitisDocument2 pagesNursing Care Plans For AppendicitisRodnie Insauriga GonzalesNo ratings yet
- NCPDocument4 pagesNCPAndrea BroccoliNo ratings yet
- Pleural EffusionDocument5 pagesPleural EffusionTerizla MobileNo ratings yet
- NCP For UtiDocument3 pagesNCP For UtiAaron Sanchez100% (1)
- Chinese General Hospital College of Nursing Nursing Care PlanDocument2 pagesChinese General Hospital College of Nursing Nursing Care PlanLoveli Yuchongtian Kiok100% (2)
- NCP OrthoDocument6 pagesNCP OrthoRuth Anne Arriesgado NañozNo ratings yet
- Subjective: The Client's Grandmother Stated " Hindi Pa Nga Siya Dumudumi Simula Nung Nahospital Siya Ngayon. Mga Apat Na Araw Na Ata." ObjectiveDocument2 pagesSubjective: The Client's Grandmother Stated " Hindi Pa Nga Siya Dumudumi Simula Nung Nahospital Siya Ngayon. Mga Apat Na Araw Na Ata." ObjectiveAngelou MortosNo ratings yet
- NCP For Post Op Wound and FractureDocument6 pagesNCP For Post Op Wound and FractureAlyssa Marie50% (2)
- n320 Peds NCP wk3Document2 pagesn320 Peds NCP wk3api-301826049No ratings yet
- Electrolyte Imbalance NCPDocument8 pagesElectrolyte Imbalance NCPManuel Jacob YradNo ratings yet
- Nursing Care PlanDocument3 pagesNursing Care PlanJayalakshmi David50% (2)
- NCP Activity IntoleranceDocument2 pagesNCP Activity IntoleranceAce Dioso TubascoNo ratings yet
- Cholecystitis NCPDocument5 pagesCholecystitis NCPtsukino143No ratings yet
- Cues Nursing Diagnosis Rationale Goals and Objectives Nursing Intervention Rationale Evaluation SubjectiveDocument4 pagesCues Nursing Diagnosis Rationale Goals and Objectives Nursing Intervention Rationale Evaluation SubjectiveFaye Dianne Damian-BuenafeNo ratings yet
- NCP For OxygenationDocument6 pagesNCP For OxygenationChriz LechNo ratings yet
- NCP PediaDocument2 pagesNCP PediaMick De LeonNo ratings yet
- Acute Pain Related To Body Response To An Infective AgentDocument2 pagesAcute Pain Related To Body Response To An Infective AgentSheril Sularte CasanesNo ratings yet
- NCP - Ineffective Airway ClearanceDocument4 pagesNCP - Ineffective Airway ClearanceKen RegalaNo ratings yet
- NCP StrokeDocument6 pagesNCP StrokeIrish TatelNo ratings yet
- NCP Nursing Care Plan For Urinary Tract InfectionsDocument4 pagesNCP Nursing Care Plan For Urinary Tract InfectionsRaveen mayi89% (9)
- NCP Impaired SkinDocument3 pagesNCP Impaired SkinRuby AnneNo ratings yet
- Impaired Skin IntegrityDocument3 pagesImpaired Skin IntegrityAubrey SungaNo ratings yet
- Short Term: Independent: Independent: Short TermDocument2 pagesShort Term: Independent: Independent: Short TermAndre ImperialNo ratings yet
- Short Term: Nursing Care Plan Cues Nursing Diagnosis Objectives Interventions Rationale EvaluationDocument3 pagesShort Term: Nursing Care Plan Cues Nursing Diagnosis Objectives Interventions Rationale EvaluationChristy BerryNo ratings yet
- NCP Knowledge Deficit PDFDocument2 pagesNCP Knowledge Deficit PDFskylertNo ratings yet
- High Percentage of Sleep Disturbances Can Affect The Recovery of The PatientDocument1 pageHigh Percentage of Sleep Disturbances Can Affect The Recovery of The PatientMatt SinnungNo ratings yet
- NCP - Risk Impaired Skin RT Altered Circulation (Spinal Injury)Document2 pagesNCP - Risk Impaired Skin RT Altered Circulation (Spinal Injury)yanny0350% (2)
- Breast Cancer Risk For InfectionDocument6 pagesBreast Cancer Risk For Infectionam peNo ratings yet
- Gout N C P BY BHERU LALDocument1 pageGout N C P BY BHERU LALBheru LalNo ratings yet
- NCP For Acute PainDocument2 pagesNCP For Acute PainEmman RamosNo ratings yet
- Nursing Care PlanDocument3 pagesNursing Care PlanInah Arcellana100% (2)
- Nursing Care Plan PreoperativeDocument5 pagesNursing Care Plan Preoperativekuro hanabusaNo ratings yet
- Fistula NCPDocument1 pageFistula NCPHasna LisnaNo ratings yet
- Ceftriaxone and CiprofloxacinDocument4 pagesCeftriaxone and CiprofloxacinRae DaWn VaLesNo ratings yet
- Ventricular Septal Defect, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandVentricular Septal Defect, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- NCPDocument6 pagesNCPAngelaTrinidadNo ratings yet
- NCP FinalDocument7 pagesNCP FinalRuss RussNo ratings yet
- NCPDocument7 pagesNCPLouis RoderosNo ratings yet
- Suvendrini Kakuchi. Global Information Network. New York: Apr 12, 2007. Pg. 1Document5 pagesSuvendrini Kakuchi. Global Information Network. New York: Apr 12, 2007. Pg. 1Arianne Kamille AndesNo ratings yet
- Health Care Delivery SystemDocument40 pagesHealth Care Delivery SystemArianne Kamille Andes100% (1)
- Case Report - Nissen FundoplicationDocument4 pagesCase Report - Nissen FundoplicationArianne Kamille AndesNo ratings yet
- Economics of ProductionDocument26 pagesEconomics of ProductionaleachonNo ratings yet
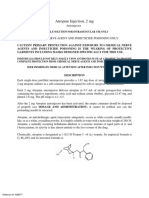
- Atropine Injection, 2 MGDocument14 pagesAtropine Injection, 2 MGJake DavisNo ratings yet
- MIDTERM TEST 9.docx Đề 9 Lớp 10Document7 pagesMIDTERM TEST 9.docx Đề 9 Lớp 10nguyenthikimtruc15No ratings yet
- Adc HTN CPSCRDocument40 pagesAdc HTN CPSCRaditya.3757No ratings yet
- Health Care System in India at Central LevelDocument11 pagesHealth Care System in India at Central LevelKailash NagarNo ratings yet
- Typology of Learners With Special Needs C. Learners With Physical Disability - 1. Visual ImpairmentDocument41 pagesTypology of Learners With Special Needs C. Learners With Physical Disability - 1. Visual ImpairmentArvinB. NarcisoNo ratings yet
- DsaDocument235 pagesDsaLalaine De Jesus100% (1)
- TLCR 20 635 Author Proof1Document17 pagesTLCR 20 635 Author Proof129milce17No ratings yet
- 8 National Nutrition Survey: Philippine Nutrition Facts and Figures 2013Document148 pages8 National Nutrition Survey: Philippine Nutrition Facts and Figures 2013Mia DangaNo ratings yet
- Manual HIV1 2WesterBlotDocument4 pagesManual HIV1 2WesterBlotayuningtyas wahyuNo ratings yet
- MicroPara LabDocument10 pagesMicroPara LabLyra FeliceNo ratings yet
- Niversity of The Philippines Manila: Nursing Health History Date of Interview: (Input) A. Biographic DataDocument4 pagesNiversity of The Philippines Manila: Nursing Health History Date of Interview: (Input) A. Biographic DataConstance Isabelle MercadoNo ratings yet
- MOriamin ForteDocument1 pageMOriamin Forteianecunar100% (3)
- Vera7 Strategic Marketing CorporationDocument23 pagesVera7 Strategic Marketing CorporationmarkanthonyrllamesNo ratings yet
- Neomycin and Prednisolone Acetate Ophthalmic SuspensionDocument10 pagesNeomycin and Prednisolone Acetate Ophthalmic SuspensionInne Widya UtamiNo ratings yet
- Unit 2.2 (Complete)Document11 pagesUnit 2.2 (Complete)Génesis DuránNo ratings yet
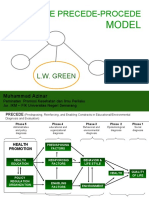
- The Precede-Procede: ModelDocument12 pagesThe Precede-Procede: ModelArda Krisnata100% (1)
- Critical Reading 3 (2Document17 pagesCritical Reading 3 (22762904542mbcNo ratings yet
- Chapter 1 5 Not FinalDocument102 pagesChapter 1 5 Not FinalKc Alecks V. BaliwasNo ratings yet
- Placental Exosomes Research Day v3Document29 pagesPlacental Exosomes Research Day v3Rasha TelebNo ratings yet
- Disinfection GatewayDocument6 pagesDisinfection GatewaylynnNo ratings yet
- Review General & USMLE Microbiology MCQsDocument51 pagesReview General & USMLE Microbiology MCQsM7md Allahham100% (1)
- A Case of Complete Heart Block With Diagnostic Challenge and Therapeutic DilemmaDocument4 pagesA Case of Complete Heart Block With Diagnostic Challenge and Therapeutic DilemmaXo YemNo ratings yet
- Zimmer Tourniquet Ats 4000 Operator Service ManualDocument76 pagesZimmer Tourniquet Ats 4000 Operator Service ManualImane ObalahcenNo ratings yet
- Deciphering The Association Between Psoriasis and Obesity Current Evidence and Treatment ConsiderationsDocument14 pagesDeciphering The Association Between Psoriasis and Obesity Current Evidence and Treatment ConsiderationsnikhithnixNo ratings yet
- Written Assessment Information Booklet Website July 2018Document11 pagesWritten Assessment Information Booklet Website July 2018aaditi2mudaliarNo ratings yet
- KBA Dyslipidemia 2023 Oct 31 TueDocument36 pagesKBA Dyslipidemia 2023 Oct 31 TueKamran B AliNo ratings yet