Physiotherapy in PCOS
Physiotherapy in PCOS
Download as pptx, pdf, or txt
At a glance
Powered by AI
Some key takeaways are that PCOS was originally described in 1935 and includes symptoms like amenorrhea, hirsutism and obesity. It also increases risks for conditions like diabetes, heart disease and infertility.
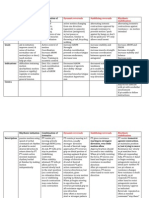
The 1990 NICHD and 2003 Rotterdam guidelines outline diagnostic criteria including signs of hyperandrogenism and oligo/anovulation with exclusion of other causes.
Treatment options include lifestyle changes, medications to regulate hormones and periods, cosmetic treatments for hair growth, and surgeries like ovarian drilling or bariatric surgery in severe cases.
You might also like
- Textbook of Physiotherapy For Obstetric and Gynecological Conditions MASUD PDFDocument205 pagesTextbook of Physiotherapy For Obstetric and Gynecological Conditions MASUD PDFAlina Gherman-Haiduc75% (4)
- Physiotherapy For Tennis ElbowDocument2 pagesPhysiotherapy For Tennis ElbowenadNo ratings yet
- Research Methodology: For All Physiotherapy and Allied Health Sciences StudentsDocument1 pageResearch Methodology: For All Physiotherapy and Allied Health Sciences StudentsProductivity 100100% (1)
- A Practical Guide to the Self-Management of Lower Back Pain: A Holistic Approach to Health and FitnessFrom EverandA Practical Guide to the Self-Management of Lower Back Pain: A Holistic Approach to Health and FitnessNo ratings yet
- Divine Intervention Episode 22 Obgyn Shelf Review PDFDocument167 pagesDivine Intervention Episode 22 Obgyn Shelf Review PDFSwisskelly1100% (1)
- Gynecologic Problems of Childhood: Anne Margrette C. VelasquezDocument46 pagesGynecologic Problems of Childhood: Anne Margrette C. VelasquezAnne Margrette Velasquez50% (2)
- Polycystic Ovarian SyndromeDocument36 pagesPolycystic Ovarian SyndromeRaras Mayang100% (1)
- Physiotherapy For Stroke Patients - Physiotherapy Remedies For Victims of StrokeDocument9 pagesPhysiotherapy For Stroke Patients - Physiotherapy Remedies For Victims of StrokeHumaira RahmanNo ratings yet
- Antenatal ExercisesDocument52 pagesAntenatal ExercisesPooja jainNo ratings yet
- Active and Passive MovementsDocument20 pagesActive and Passive MovementsSajida Bibi Noonari57% (7)
- Physiotherapy PTDocument25 pagesPhysiotherapy PTPriyank KhokareNo ratings yet
- Physiotherapy in Obstetrics GynaecologyDocument90 pagesPhysiotherapy in Obstetrics Gynaecologyمركز ريلاكس للعلاج الطبيعيNo ratings yet
- Scoliosis PPT B IngDocument11 pagesScoliosis PPT B IngSyifa Anindya100% (1)
- International Classification of Impairments, Disabilities and HandicapsDocument22 pagesInternational Classification of Impairments, Disabilities and HandicapsTimoteo Timothy WilliamsNo ratings yet
- History Taking Form Final - Doc Version 1Document5 pagesHistory Taking Form Final - Doc Version 1Mahnoor AqeelNo ratings yet
- Physiotherapy For Women Obs PDFDocument167 pagesPhysiotherapy For Women Obs PDFvidyasagar pagilla100% (2)
- Physiotherapy Neurological Assessment Form: Glasgow Coma Scale: /15Document6 pagesPhysiotherapy Neurological Assessment Form: Glasgow Coma Scale: /15PC LaptopNo ratings yet
- 07.03.09 Chest PhysiotherapyDocument9 pages07.03.09 Chest PhysiotherapyLuqmanul HakimNo ratings yet
- WCPT (World Confederation For Physical Therapy) Declarations of PrincipleDocument37 pagesWCPT (World Confederation For Physical Therapy) Declarations of PrincipleRivo100% (2)
- Gyne Assessment FormDocument8 pagesGyne Assessment FormLal KhanNo ratings yet
- Walking AidsDocument27 pagesWalking AidsFarah ZahidNo ratings yet
- Role of Physiotherapy in Antenatal and Post-Natal Care: Dr. Venus Pagare (PT)Document96 pagesRole of Physiotherapy in Antenatal and Post-Natal Care: Dr. Venus Pagare (PT)Haneen Jehad Um MalekNo ratings yet
- Prinicples of PhysiotherapyDocument29 pagesPrinicples of PhysiotherapyKumaravel MuruganNo ratings yet
- Role of Physiotherapy in Antenatal and Post-Natal Care: Dr. Venus Pagare (PT)Document74 pagesRole of Physiotherapy in Antenatal and Post-Natal Care: Dr. Venus Pagare (PT)Haneen Jehad Um Malek100% (1)
- Exercise Prescription in Pre and Post-NatalDocument63 pagesExercise Prescription in Pre and Post-NatalSim ShkNo ratings yet
- 4 NCV1Document115 pages4 NCV1sridhar100% (2)
- Physiotherapy in Obstetrics and GynaecologyDocument6 pagesPhysiotherapy in Obstetrics and GynaecologyGul RockzzNo ratings yet
- Unhappy Triad of O'DonahueDocument14 pagesUnhappy Triad of O'DonahueGuadalupe GuzmánNo ratings yet
- Obstretics AssessmentDocument6 pagesObstretics AssessmentToli kkakrNo ratings yet
- Training For The Female Athlete Children and Special PopulationDocument25 pagesTraining For The Female Athlete Children and Special PopulationAqsa ZaheerNo ratings yet
- Assignment: Cervical SpondylosisDocument14 pagesAssignment: Cervical SpondylosisJaspreet kaurNo ratings yet
- Introduction To Physiotherapy in General Surgical ConditionsDocument20 pagesIntroduction To Physiotherapy in General Surgical Conditionsakheel ahammedNo ratings yet
- ICUDocument12 pagesICUNabilahNo ratings yet
- BPT Biomechanics Repeated Questions AllDocument12 pagesBPT Biomechanics Repeated Questions AllT. AFFRANo ratings yet
- Case of Peripheral Vascular Disease: Dr. Shresth ManglikDocument18 pagesCase of Peripheral Vascular Disease: Dr. Shresth ManglikShresth ManglikNo ratings yet
- The Indian Association of Physiotherapists - IAP Constitutions PDFDocument17 pagesThe Indian Association of Physiotherapists - IAP Constitutions PDFHasan Rahman100% (2)
- Physiotherapy For PoliomyelitisDocument16 pagesPhysiotherapy For Poliomyelitisabdalsucs100% (1)
- Physiotherapy Management ForDocument28 pagesPhysiotherapy Management Formayuri zanwarNo ratings yet
- Paediatric Physiotherapy Involves The AssessmentDocument2 pagesPaediatric Physiotherapy Involves The AssessmentL RNo ratings yet
- MPT PDFDocument141 pagesMPT PDFSWATHI G ANo ratings yet
- Physiotherapy in Gastrectomy CholecystectomyDocument19 pagesPhysiotherapy in Gastrectomy Cholecystectomyakheel ahammedNo ratings yet
- Physiotherapy Neurological Assesment Form: JH RehabilitationDocument9 pagesPhysiotherapy Neurological Assesment Form: JH RehabilitationSureaka PonnusamyNo ratings yet
- 14 Biomechanics of Normal Human Gait PDFDocument26 pages14 Biomechanics of Normal Human Gait PDFDiego A. MezaNo ratings yet
- Pregnancy and PhysiotherapyDocument40 pagesPregnancy and PhysiotherapyMotherBee Support100% (1)
- Muscle Re-EducationDocument41 pagesMuscle Re-EducationS.JAIVIGNESH OTNo ratings yet
- Case Studies Physiotherapy: Practice-Based LearningDocument14 pagesCase Studies Physiotherapy: Practice-Based LearningAnwar moosa100% (1)
- Presented by DR Muhammad Usman Senior Lecturer BUCPT: Introduction To Screening For Referral in Physical TherapyDocument27 pagesPresented by DR Muhammad Usman Senior Lecturer BUCPT: Introduction To Screening For Referral in Physical Therapysaba ramzanNo ratings yet
- Posture PhysiotherapyDocument19 pagesPosture Physiotherapyjijo123408No ratings yet
- McKenzie CONCEPT AnilDocument12 pagesMcKenzie CONCEPT AnilSOUMYADEEP BHUINYANo ratings yet
- Fluidotherap by DR VVR ChowdharyDocument3 pagesFluidotherap by DR VVR Chowdharyvenkata ramakrishnaiahNo ratings yet
- Contemporary Task Oriented ApproachDocument17 pagesContemporary Task Oriented ApproachAkshay BadoreNo ratings yet
- Role of Physiotherapy in Management of Polio..seminarDocument14 pagesRole of Physiotherapy in Management of Polio..seminarAmandeep SinghNo ratings yet
- Clinical Guidelines For The Physiotherapy Management of Females Aged 16-65 With Stress Urinary IncontinenceDocument72 pagesClinical Guidelines For The Physiotherapy Management of Females Aged 16-65 With Stress Urinary IncontinenceAndré RodriguesNo ratings yet
- Amputation: Dr. Abdul Rashad Senior Lecturer DPT, Mphill (Opt), Mppta United College of Physical TherapyDocument31 pagesAmputation: Dr. Abdul Rashad Senior Lecturer DPT, Mphill (Opt), Mppta United College of Physical Therapypasha100% (1)
- Posture LectureDocument33 pagesPosture Lectureapi-301417414No ratings yet
- Pelvic Floor Physiotherapy HOACllDocument9 pagesPelvic Floor Physiotherapy HOACllEsteban CayuelasNo ratings yet
- PNF TableDocument4 pagesPNF Tableblitzkrieg5891100% (1)
- Physiotherapy Guidelines For Manual HyperinflationDocument5 pagesPhysiotherapy Guidelines For Manual HyperinflationAhmed Abd Elrauf100% (2)
- Women's Health & Physical Rehabilitation.Document31 pagesWomen's Health & Physical Rehabilitation.Arham ShamsiNo ratings yet
- Physiotherapy in AmputationsDocument6 pagesPhysiotherapy in Amputationskrissh20100% (1)
- Compartment Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandCompartment Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- PROLOG: Obstetrics, Ninth Edition (Assessment & Critique)From EverandPROLOG: Obstetrics, Ninth Edition (Assessment & Critique)No ratings yet
- Jurnal Pcos InternationalDocument5 pagesJurnal Pcos InternationalPuput Anistiya Hariani100% (1)
- My Experience With Kali Brom in A Case of Polycystic Ovarian SyndromeDocument6 pagesMy Experience With Kali Brom in A Case of Polycystic Ovarian SyndromeHomoeopathic Pulse100% (1)
- Epidemiology, Diagnosis, and Management of Polycystic Ovary SyndromeDocument14 pagesEpidemiology, Diagnosis, and Management of Polycystic Ovary SyndromeAlyssa JenningsNo ratings yet
- Reproductive Endocrinology and HyperandrogenismDocument11 pagesReproductive Endocrinology and HyperandrogenismaamnakamalkqNo ratings yet
- Secondary Amenorrhea: DR Hanaa AlaniDocument44 pagesSecondary Amenorrhea: DR Hanaa AlaniAakashNo ratings yet
- Laboratory Diagnosis of Polycystic Ovary Syndrome (PCOS) : Nkem Okoye, PH.DDocument43 pagesLaboratory Diagnosis of Polycystic Ovary Syndrome (PCOS) : Nkem Okoye, PH.DRabab HosseiniNo ratings yet
- Evaluation and Management of Primary Amenorrhea - UpToDateDocument14 pagesEvaluation and Management of Primary Amenorrhea - UpToDateCristinaCaprosNo ratings yet
- Unas Mei 2020 (Sule) : Yang Dianggap Soal BaruDocument15 pagesUnas Mei 2020 (Sule) : Yang Dianggap Soal Baruhari ilman toniNo ratings yet
- AlopeciaDocument90 pagesAlopeciasmbawasainiNo ratings yet
- Hiperandrogenismo ArtigoDocument11 pagesHiperandrogenismo ArtigoFernando RibeiroNo ratings yet
- No. 34. Management of Infertility Caused by Ovulatory DysfunctionDocument19 pagesNo. 34. Management of Infertility Caused by Ovulatory DysfunctionAnnisa JuwitaNo ratings yet
- Acne and DiabetesDocument5 pagesAcne and DiabetesMuhammad Nur ArifinNo ratings yet
- Uerm Board Review - ObDocument15 pagesUerm Board Review - ObCamilla FernandezNo ratings yet
- Polycystic Ovarian Disease or Polycystic Ovarian Syndrome How To Identify and Manage A ReviewDocument5 pagesPolycystic Ovarian Disease or Polycystic Ovarian Syndrome How To Identify and Manage A ReviewshivaniNo ratings yet
- IJRAR23D2391Document6 pagesIJRAR23D2391Itti MishraNo ratings yet
- 03 DM Typ 2 ISAPAD 22Document23 pages03 DM Typ 2 ISAPAD 22Awais ArshadNo ratings yet
- Polycystic Ovary SyndromeDocument6 pagesPolycystic Ovary SyndromeHAVIZ YUADNo ratings yet
- GynaecologyDocument123 pagesGynaecologyKiranNo ratings yet
- Ebook Download Immunology of Recurrent Pregnancy Loss and Implantation Failure 1st Edition Joanna Kwak-Kim (Editor) - Ebook PDF All ChapterDocument54 pagesEbook Download Immunology of Recurrent Pregnancy Loss and Implantation Failure 1st Edition Joanna Kwak-Kim (Editor) - Ebook PDF All Chapterjadynlebet100% (6)
- PCOS Patient HandoutDocument16 pagesPCOS Patient HandoutAnonymous NI5oJfd2cNo ratings yet
- RA - Effect of Metformin in Patient With Polycystic Ovary Syndrome (PCOS)Document11 pagesRA - Effect of Metformin in Patient With Polycystic Ovary Syndrome (PCOS)raman osmanNo ratings yet
- Insulin Resistance and PCOS-dr. Hilma Final 11 Juli 2021 FIXDocument48 pagesInsulin Resistance and PCOS-dr. Hilma Final 11 Juli 2021 FIXputrihealthirezaNo ratings yet
- AmenorrheaDocument51 pagesAmenorrheabisharatNo ratings yet
- Accelerated Episodic Luteinizing Hormone Release Accompanies Blunted Progesterone Regulation in PCOS-like Female Rhesus Monkeys (Macaca Mulatta) Exposed To Testosterone During Early-to-Mid GestationDocument14 pagesAccelerated Episodic Luteinizing Hormone Release Accompanies Blunted Progesterone Regulation in PCOS-like Female Rhesus Monkeys (Macaca Mulatta) Exposed To Testosterone During Early-to-Mid GestationEricko Ongko JoyoNo ratings yet
- Saliva Test Report: Your Results at A GlanceDocument7 pagesSaliva Test Report: Your Results at A GlanceKaveh EshkoftiNo ratings yet
- Natural Selection For Genetic Variants in Sport: The Role of Y Chromosome Genes in Elite Female Athletes With 46, XY DSDDocument6 pagesNatural Selection For Genetic Variants in Sport: The Role of Y Chromosome Genes in Elite Female Athletes With 46, XY DSDGilang Ridha FathurrahmanNo ratings yet
- Divya AmbetkarDocument13 pagesDivya AmbetkarAnonymous CwJeBCAXpNo ratings yet