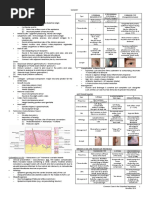
Pediatric GI Radiology
Pediatric GI Radiology
Download as doc, pdf, or txt
You might also like
- QuestionsDocument47 pagesQuestionsCharizza Yvette100% (1)
- Patho Intussusception RevisedDocument8 pagesPatho Intussusception RevisedPj Gabano60% (5)
- Neonatal Intestinal ObstructionDocument21 pagesNeonatal Intestinal ObstructionShahzad Bashir ShamsNo ratings yet
- Test Bank On GI PathologyDocument14 pagesTest Bank On GI PathologySeff CausapinNo ratings yet
- Small BowelDocument4 pagesSmall Bowelsarguss14100% (1)
- Kidney, Ureter, BladderDocument12 pagesKidney, Ureter, Bladdersarguss14100% (1)
- Bone TumorsDocument15 pagesBone Tumorssarguss1450% (2)
- (RADIO 250) LEC 03 Genitourinary and KUB ImagingDocument7 pages(RADIO 250) LEC 03 Genitourinary and KUB ImagingWilliam PinzonNo ratings yet
- ENDOCRINE PATHOLOGY WebpathDocument35 pagesENDOCRINE PATHOLOGY Webpathapi-3766657No ratings yet
- Prostate GlandsDocument3 pagesProstate GlandsDragan PetrovicNo ratings yet
- Cyanotic Congenital Heart Diseases, Etc.Document12 pagesCyanotic Congenital Heart Diseases, Etc.sarguss14100% (2)
- Accordion Sign-Appearance (C. Difficile)Document41 pagesAccordion Sign-Appearance (C. Difficile)Andra HijratulNo ratings yet
- Hepatic AbscessesDocument6 pagesHepatic Abscessesmohamed mowafeyNo ratings yet
- SURGERY Lecture 5 - Abdominal Wall, Omentum, Mesentery, Retroperitoneum (Dr. Wenceslao)Document13 pagesSURGERY Lecture 5 - Abdominal Wall, Omentum, Mesentery, Retroperitoneum (Dr. Wenceslao)Medisina101No ratings yet
- Surgery by GiselleDocument15 pagesSurgery by GiselleTris100% (1)
- Exam OS 214: Nephrology: Lec 08: Pathology of Tubular DiseasesDocument5 pagesExam OS 214: Nephrology: Lec 08: Pathology of Tubular DiseasesKarl Jimenez SeparaNo ratings yet
- Pathology Week 17 p31-41Document11 pagesPathology Week 17 p31-41zeroun24No ratings yet
- Red Vascular: Polygonal Cells Growing in Nests or Cords Lamellae of Dense CollagenDocument3 pagesRed Vascular: Polygonal Cells Growing in Nests or Cords Lamellae of Dense CollagenMaryam FadahNo ratings yet
- Cardiac ImagingDocument7 pagesCardiac Imagingsarguss14No ratings yet
- Pathogenesis Bleeding DisordersDocument4 pagesPathogenesis Bleeding DisordersGerardLumNo ratings yet
- Surgical Anatomy of The Chest Wall, Pleura, and MediastinumDocument8 pagesSurgical Anatomy of The Chest Wall, Pleura, and MediastinumNooneNo ratings yet
- Pathology Week 6 p1-17Document17 pagesPathology Week 6 p1-17zeroun24No ratings yet
- Hematology Anemia Clinical Manifestations of Anemia MECHANISM OF ANEMIA (How It Develops)Document10 pagesHematology Anemia Clinical Manifestations of Anemia MECHANISM OF ANEMIA (How It Develops)Jüdith Marie Reyes BauntoNo ratings yet
- COVID-19 - Diagnosis - UpToDateDocument28 pagesCOVID-19 - Diagnosis - UpToDateTerang MelialaNo ratings yet
- Genitourinary SystemDocument8 pagesGenitourinary Systemsarguss14100% (1)
- Metabolic Bone DiseasesDocument4 pagesMetabolic Bone DiseasesGerardLum100% (1)
- 4.1c - MEN Syndromes - Nov.10 - Dr. GalangDocument2 pages4.1c - MEN Syndromes - Nov.10 - Dr. GalangMiel Raphael AranillaNo ratings yet
- Superficial Parotidectomy Through Retrograde Facial Nerve DissectionDocument8 pagesSuperficial Parotidectomy Through Retrograde Facial Nerve DissectionAnonymous LnWIBo1GNo ratings yet
- Genetic Disorders-Www - Qworld.co - inDocument13 pagesGenetic Disorders-Www - Qworld.co - inQworld100% (1)
- NeuropathologyDocument66 pagesNeuropathologyKaramsi Gopinath NaikNo ratings yet
- PleuraDocument6 pagesPleuraameerabest100% (1)
- Dokumen - Tips Rubins Pathology Clinicopathologic Foundations of Medicine 7th Edition ChairmanDocument21 pagesDokumen - Tips Rubins Pathology Clinicopathologic Foundations of Medicine 7th Edition ChairmanNare NNo ratings yet
- (Surg2) 5.3 Urology Part 2 - Dr. YusiDocument19 pages(Surg2) 5.3 Urology Part 2 - Dr. YusiAlloiBialbaNo ratings yet
- STEPS MalrotationDocument30 pagesSTEPS MalrotationsyafiqNo ratings yet
- Acute LeukemiaDocument16 pagesAcute Leukemianouval_iqbalNo ratings yet
- 1.33 (Surgery) Hepatobiliary Tract Part 2Document8 pages1.33 (Surgery) Hepatobiliary Tract Part 2Leo Mari Go LimNo ratings yet
- Harrison-Principals of Internal Medicine 20th. Ed. Prt.7-11Document707 pagesHarrison-Principals of Internal Medicine 20th. Ed. Prt.7-11Choi DongYiNo ratings yet
- AV UWorld EOs (Rough Draft) - Data - Repeat LandscapeDocument139 pagesAV UWorld EOs (Rough Draft) - Data - Repeat LandscapeJonathan AiresNo ratings yet
- Pulmonary PathologyDocument6 pagesPulmonary PathologyjamesjaanNo ratings yet
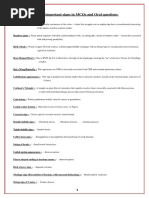
- Some Important Signs in Mcqs and Oral QuestionsDocument3 pagesSome Important Signs in Mcqs and Oral Questionsخلدون سليمNo ratings yet
- Surgicl Pathology of OesophagusDocument91 pagesSurgicl Pathology of Oesophagusmikaaa000No ratings yet
- Pathology Week 5 p41-42Document2 pagesPathology Week 5 p41-42zeroun24No ratings yet
- Benign Gyne LesionsDocument133 pagesBenign Gyne LesionsJulie Ann ValenciaNo ratings yet
- Anatomy Imporatant Points by Dr. Asif AliDocument31 pagesAnatomy Imporatant Points by Dr. Asif AliSyed imran AbbasNo ratings yet
- Stage 1: Dorsal Induction: Pediatric NeuroradiologyDocument8 pagesStage 1: Dorsal Induction: Pediatric Neuroradiologysarguss14100% (1)
- MIS-C: Clinic-Diagnostic/Dispo Recs For Multisystem Inflammatory Syndrome in ChildrenDocument8 pagesMIS-C: Clinic-Diagnostic/Dispo Recs For Multisystem Inflammatory Syndrome in ChildrenJosselle Sempio CalientaNo ratings yet
- HerniaDocument5 pagesHerniasarguss14100% (5)
- Basic Ercp InterpretationDocument19 pagesBasic Ercp Interpretationhoneyworks100% (2)
- Underground Clinical Vignettes Pa Tho Physiology IIIDocument116 pagesUnderground Clinical Vignettes Pa Tho Physiology IIImagunesNo ratings yet
- Rapid Review of Hematology (Aug 31, 2013) - (9350909618) - (Jaypee Brothers Medical Pub)Document149 pagesRapid Review of Hematology (Aug 31, 2013) - (9350909618) - (Jaypee Brothers Medical Pub)Dana AhmedNo ratings yet
- Breast CancerDocument6 pagesBreast Cancersarguss14No ratings yet
- Amboss:CardioDocument18 pagesAmboss:CardioNicole Juliette CCNo ratings yet
- #MediastinumDocument4 pages#Mediastinumameerabest100% (1)
- Neck Swelling MotaweaDocument8 pagesNeck Swelling MotaweaMahmoud MotaweaNo ratings yet
- Quizlet (4) MMMMMMDocument30 pagesQuizlet (4) MMMMMMnaimNo ratings yet
- Hereditary Spherocytosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHereditary Spherocytosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Surgical Principles in Inguinal Hernia Repair: A Comprehensive Guide to Anatomy and Operative TechniquesFrom EverandSurgical Principles in Inguinal Hernia Repair: A Comprehensive Guide to Anatomy and Operative TechniquesMelissa Phillips LaPinskaNo ratings yet
- Singer and Monaghan's Cervical and Lower Genital Tract Precancer: Diagnosis and TreatmentFrom EverandSinger and Monaghan's Cervical and Lower Genital Tract Precancer: Diagnosis and TreatmentRating: 5 out of 5 stars5/5 (1)
- Axial Arthritis: Degenerative Annular DiseaseDocument18 pagesAxial Arthritis: Degenerative Annular Diseasesarguss14100% (1)
- Epidural and Spinal AnesthesiaDocument86 pagesEpidural and Spinal Anesthesiasarguss1478% (9)
- Stage 1: Dorsal Induction: Pediatric NeuroradiologyDocument8 pagesStage 1: Dorsal Induction: Pediatric Neuroradiologysarguss14100% (1)
- Inhalational Anesthetics: Patigas, Requinta, ResuelloDocument88 pagesInhalational Anesthetics: Patigas, Requinta, Resuellosarguss140% (1)
- Cyanotic Congenital Heart Diseases, Etc.Document12 pagesCyanotic Congenital Heart Diseases, Etc.sarguss14100% (2)
- NeuroradiologyDocument11 pagesNeuroradiologysarguss14100% (2)
- Mental Retardation and Learning DisordersDocument4 pagesMental Retardation and Learning Disorderssarguss14100% (1)
- Cardiac ImagingDocument7 pagesCardiac Imagingsarguss14No ratings yet
- From Doc Bandong's Own Words:: Shar 1 of 20Document20 pagesFrom Doc Bandong's Own Words:: Shar 1 of 20sarguss14100% (1)
- Introduction To RadiologyDocument3 pagesIntroduction To Radiologysarguss14No ratings yet
- Substance AbuseDocument4 pagesSubstance Abusesarguss14No ratings yet
- Pleura and MediastinumDocument16 pagesPleura and Mediastinumsarguss14100% (1)
- NeuroradiologyDocument25 pagesNeuroradiologysarguss14100% (2)
- Gallbladder, Liver, Pancreas and SpleenDocument19 pagesGallbladder, Liver, Pancreas and Spleensarguss14100% (3)
- Congenital Cystic Adenomatoid Malformation (CCAM)Document7 pagesCongenital Cystic Adenomatoid Malformation (CCAM)sarguss14No ratings yet
- Genitourinary SystemDocument8 pagesGenitourinary Systemsarguss14100% (1)
- Developmental AssessmentDocument3 pagesDevelopmental Assessmentsarguss14No ratings yet
- Dissociative and Eating DisordersDocument6 pagesDissociative and Eating Disorderssarguss14No ratings yet
- Child Abuse and NeglectDocument3 pagesChild Abuse and Neglectsarguss14No ratings yet
- DepressionDocument3 pagesDepressionsarguss14No ratings yet
- The Normal Kidney: Pediatrics 2 The Urinary System and Urinary Tract InfectionsDocument4 pagesThe Normal Kidney: Pediatrics 2 The Urinary System and Urinary Tract Infectionssarguss14No ratings yet
- Bipolar DisordersDocument8 pagesBipolar Disorderssarguss14100% (2)
- Respiratory Distress of The NewbornDocument3 pagesRespiratory Distress of The Newbornsarguss14100% (1)
- Pediatric Endocrinology Part 2: Pediatrics 2Document8 pagesPediatric Endocrinology Part 2: Pediatrics 2sarguss14No ratings yet
- Case Presentation VolvulusDocument34 pagesCase Presentation Volvulusanjawi5No ratings yet
- DR. Bikash BK Thapa MS-General Surgery: 1 BbthapaDocument75 pagesDR. Bikash BK Thapa MS-General Surgery: 1 BbthapaNinaNo ratings yet
- Mini Osce 2021Document31 pagesMini Osce 2021anashuseinmalkawiNo ratings yet
- Benefit Packages (Private)Document103 pagesBenefit Packages (Private)You Are Not Wasting TIME HereNo ratings yet
- Nursing Care Plan of Ulcerative ColitisDocument1 pageNursing Care Plan of Ulcerative ColitisFlower AnneNo ratings yet
- Medical Facts and Mcq's Pediatric Surgery MCQDocument34 pagesMedical Facts and Mcq's Pediatric Surgery MCQMohammed Kassim Abdul Jabbar100% (3)
- Intestinal Diseases in Cattle 2023Document30 pagesIntestinal Diseases in Cattle 2023Krystyna WędrychowskaNo ratings yet
- Bowel ObstructionDocument48 pagesBowel ObstructionPatrick John100% (1)
- Recognizing SBO, LBO and IleusDocument51 pagesRecognizing SBO, LBO and IleusLanny Dwi ChandraNo ratings yet
- Intestinal ObstructionDocument12 pagesIntestinal ObstructionNurul Nurnita100% (1)
- Radiological Anatomy With Barium MealDocument58 pagesRadiological Anatomy With Barium MealjmuhilanNo ratings yet
- Abdominal X RayDocument64 pagesAbdominal X RayabhishekbmcNo ratings yet
- Acute Abdomen, Nyeri Akut AbdomenDocument35 pagesAcute Abdomen, Nyeri Akut AbdomenYanuar Yudha SudrajatNo ratings yet
- Laparoscopy in The Acute AbdomenDocument15 pagesLaparoscopy in The Acute AbdomenDragoiu AlexandraNo ratings yet
- Acute Appendicitis in Children Management - 2019 - UptodateDocument20 pagesAcute Appendicitis in Children Management - 2019 - Uptodatewinnie MontalvoNo ratings yet
- Marquez 12d NCP Mod 3Document2 pagesMarquez 12d NCP Mod 3Macy MarquezNo ratings yet
- Abdominal Tuberculosis PDFDocument54 pagesAbdominal Tuberculosis PDFNashif Rayhan100% (1)
- Surgery NotesDocument200 pagesSurgery NotesJasneet SinghNo ratings yet
- Head To Toe AssessmentDocument17 pagesHead To Toe Assessmentjasyjes100% (2)
- Adhesive Small Bowel Obstruction-2Document16 pagesAdhesive Small Bowel Obstruction-2Indra WisesaNo ratings yet
- Complete Download Emergency Imaging Case Review Series 2e Jun 12 2019 _ 0323428754 _ Elsevier 2nd Edition Johnson Md PDF All ChaptersDocument65 pagesComplete Download Emergency Imaging Case Review Series 2e Jun 12 2019 _ 0323428754 _ Elsevier 2nd Edition Johnson Md PDF All Chaptersnorcarigona77100% (1)
- Large Bowel Obstruction by Nic MDocument42 pagesLarge Bowel Obstruction by Nic MRisky OpponentNo ratings yet
- QUESTION BANK For NursesDocument56 pagesQUESTION BANK For NursesJohn PaulNo ratings yet
- DISTURBANCES IN ABSORPTION AND ELIMINATION NotesDocument7 pagesDISTURBANCES IN ABSORPTION AND ELIMINATION NotesHoneylette Darunday100% (1)
- Dnb-General Surgery: Competency Based Training ProgrammeDocument49 pagesDnb-General Surgery: Competency Based Training ProgrammeLakshmi Mounica Grandhi100% (2)
- Ventriculoperitoneal Shunt Complications in Children An Evidence-Based Approach To Emergency Department Management PDFDocument24 pagesVentriculoperitoneal Shunt Complications in Children An Evidence-Based Approach To Emergency Department Management PDFGavin TexeirraNo ratings yet
- Final Draft Discussion Board 3-EthicsDocument3 pagesFinal Draft Discussion Board 3-Ethicsapi-324566318No ratings yet