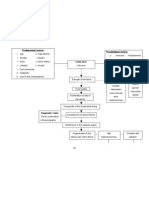
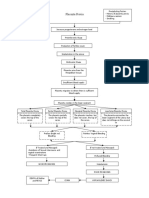
Pathophysiology
Pathophysiology
Download as doc, pdf, or txt
You might also like
- Lecture 7 - Physiology of LaborDocument30 pagesLecture 7 - Physiology of LaborMelissa Aina Mohd Yusof100% (1)
- NCP Impaired Physical MobilityDocument2 pagesNCP Impaired Physical MobilityDante Sales67% (6)
- School of Health and Allied Health Sciences Nursing Department Self-Directed Learning (Nur 146 - Clinical Area)Document3 pagesSchool of Health and Allied Health Sciences Nursing Department Self-Directed Learning (Nur 146 - Clinical Area)Milagros FloritaNo ratings yet
- Cervical Cancer Patho.2Document2 pagesCervical Cancer Patho.2Verni Dela CruzNo ratings yet
- SchistosomiasisDocument92 pagesSchistosomiasisIvan Juan75% (4)
- Bowel Obstruction PathophysiologyDocument4 pagesBowel Obstruction PathophysiologyAya BolinasNo ratings yet
- Pa Tho Physiology of Hiatal HerniaDocument1 pagePa Tho Physiology of Hiatal HerniaChiskie Faldas Genodia100% (1)
- Nursing Care Plan: Subjective: Short Term Goal: Independent: Short Term GoalDocument1 pageNursing Care Plan: Subjective: Short Term Goal: Independent: Short Term GoalDante Sales75% (4)
- Dengue Fever Health TeachingDocument3 pagesDengue Fever Health TeachingDante Sales100% (3)
- Pathophysiology PRINTDocument1 pagePathophysiology PRINTNichole Audrey SaavedraNo ratings yet
- PrefixDocument8 pagesPrefixleian28No ratings yet
- Pathophysiology of Myoma and EndometriosisDocument15 pagesPathophysiology of Myoma and EndometriosisEarle Jimenez Niervo RNNo ratings yet
- Patho MyomaDocument1 pagePatho MyomaJurilyne Rose TundagNo ratings yet
- Labor Nursing Care PlansDocument58 pagesLabor Nursing Care PlansMuhamad AriNo ratings yet
- NCP H MoleDocument6 pagesNCP H MoleMina RacadioNo ratings yet
- Drug Study - Epidural AnesthesiaDocument5 pagesDrug Study - Epidural AnesthesiaMarie PotayreNo ratings yet
- Ampicillin PDFDocument3 pagesAmpicillin PDFandriNo ratings yet
- Bleeding NCPDocument13 pagesBleeding NCPBiway Regala100% (1)
- ParacetamolDocument2 pagesParacetamolBlesyl Sison Mabano100% (1)
- Anatomy and Physiology For HELLP SyndromeDocument6 pagesAnatomy and Physiology For HELLP SyndromeRosemarie Carpio100% (1)
- Pathophysiology - AppendicitisDocument5 pagesPathophysiology - AppendicitisAzielle Joyce RosquetaNo ratings yet
- Introduction HmoleDocument32 pagesIntroduction HmoleBrian Montales BaggayanNo ratings yet
- Discharge PlanDocument4 pagesDischarge PlanVillanueva NiñaNo ratings yet
- MYOMA PathoDocument1 pageMYOMA Pathobsn2011100% (1)
- Nursing Care Plan: Angeles University Foundation College of NursingDocument3 pagesNursing Care Plan: Angeles University Foundation College of NursingPatricia Ellyne DizonNo ratings yet
- H-Mole Pathophysiology in Schematic DiagramDocument1 pageH-Mole Pathophysiology in Schematic DiagramFaith Lumayog100% (2)
- H Mole PathoDocument1 pageH Mole PathoKyle AlmeroNo ratings yet
- Preterm Labor, Hyperemesis Gravidarum - PathophysiologyDocument2 pagesPreterm Labor, Hyperemesis Gravidarum - PathophysiologyreyneldanNo ratings yet
- OB Drug Study - OxytocinDocument3 pagesOB Drug Study - OxytocinJustin AncogNo ratings yet
- Pathophysiology of Ectopic PregnancyDocument1 pagePathophysiology of Ectopic PregnancyLiza MinonaNo ratings yet
- Modifiedpatho ToyodaDocument4 pagesModifiedpatho ToyodaCaneEscabarteNo ratings yet
- Pih-Ncp - BSN2D ZacalDocument3 pagesPih-Ncp - BSN2D ZacalIllaizah EdictoNo ratings yet
- Maternal Problems With PowerDocument2 pagesMaternal Problems With PowerAlex CvgNo ratings yet
- Drug StudyDocument3 pagesDrug StudyFloribelle SamaniegoNo ratings yet
- CASE STUDY Cesarean DeliveryDocument15 pagesCASE STUDY Cesarean Deliverydirkdarren100% (3)
- NCP CholeraDocument2 pagesNCP CholeraMichael Angelo Garcia RafananNo ratings yet
- PathophysiologyDocument2 pagesPathophysiologyapi-19762967100% (1)
- Diagram Myoma IDocument1 pageDiagram Myoma IJoann100% (12)
- 8 Drug StudyDocument9 pages8 Drug StudyJohn Michael M. RosalesNo ratings yet
- Pathophysiology Cholelithiasis 2Document2 pagesPathophysiology Cholelithiasis 2Jamie HaravataNo ratings yet
- DRUG STUDY New BornDocument3 pagesDRUG STUDY New BornNikolai FuncionNo ratings yet
- Uterine MYOMADocument5 pagesUterine MYOMARoss Manalang100% (2)
- Pathophysiology of Uterine CancerDocument1 pagePathophysiology of Uterine CancerCharlotte Cordero0% (1)
- Albendazole - Drug Information PDFDocument7 pagesAlbendazole - Drug Information PDFjjjkkNo ratings yet
- Omeprazole: (Oh Me' Pray Zol)Document3 pagesOmeprazole: (Oh Me' Pray Zol)Athea MelosantosNo ratings yet
- Complications With The Power of LaborDocument8 pagesComplications With The Power of LaborEdrea Aquino MendezNo ratings yet
- NCP Acute PainDocument2 pagesNCP Acute PainNecheal BaayNo ratings yet
- Myoma PathoDocument3 pagesMyoma PathoJan Michael Artiaga100% (1)
- Rle 107 Maternal and Child Health Nursing: University of The Assumption College of Nursing and PharmacyDocument6 pagesRle 107 Maternal and Child Health Nursing: University of The Assumption College of Nursing and PharmacyEvangeline Anne Macanas100% (2)
- Scientific Analysis Goal: Goal:: Subjective CuesDocument2 pagesScientific Analysis Goal: Goal:: Subjective CuesChloie Marie RosalejosNo ratings yet
- CPD PathophysiologyDocument3 pagesCPD PathophysiologyTeanne Bathan100% (1)
- NCP Abruptio PlacentaDocument2 pagesNCP Abruptio PlacentaCarson Birth100% (1)
- Case Study Benign Tumors of The Uterus: MyomaDocument3 pagesCase Study Benign Tumors of The Uterus: MyomaToto RyanNo ratings yet
- Ectopic Pregnancy - PathophysiologyDocument1 pageEctopic Pregnancy - PathophysiologyMarimiel PagulayanNo ratings yet
- Drug Study Form OxyDocument3 pagesDrug Study Form OxyRyan OdioNo ratings yet
- Discharge Plan Methods InstructionsDocument5 pagesDischarge Plan Methods InstructionsKirk CabasaNo ratings yet
- Pathophysiology-Ng Hirschsprung DiseaseDocument3 pagesPathophysiology-Ng Hirschsprung DiseaseJan Rae Barnatia AtienzaNo ratings yet
- Ventricular Septal Defect, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandVentricular Septal Defect, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Theories of Labor OnsetDocument4 pagesTheories of Labor OnsetCzarina PorciunculaNo ratings yet
- 1st and 2nd Stage of LabourDocument137 pages1st and 2nd Stage of Labournixon odoyoNo ratings yet
- Chapter 25 NotesDocument7 pagesChapter 25 NotesJori Domini Llacuna AwayanNo ratings yet
- First Stage of LabourDocument48 pagesFirst Stage of LabourRose NyamburaNo ratings yet
- Labor and Delivery MCNDocument1 pageLabor and Delivery MCNMarinill SolimanNo ratings yet
- HyperthyroidismDocument17 pagesHyperthyroidismDante SalesNo ratings yet
- Pa Tho PhysiologyDocument1 pagePa Tho PhysiologyDante SalesNo ratings yet
- I CaseDocument20 pagesI CaseDante SalesNo ratings yet
- Obstetric Nursing DrillsDocument14 pagesObstetric Nursing DrillsClarence AnescoNo ratings yet
- Amniocentesis ProcedureDocument6 pagesAmniocentesis Proceduresweta50% (2)
- Family Planning Tubal Ligation LeafletDocument2 pagesFamily Planning Tubal Ligation LeafletTomasina Portia OrteaNo ratings yet
- The Exploitation Argument Against Commercial Surrogacy: Stephen WilkinsonDocument19 pagesThe Exploitation Argument Against Commercial Surrogacy: Stephen WilkinsonjahanviNo ratings yet
- Research Final Part 1Document5 pagesResearch Final Part 1dolly kate cagadasNo ratings yet
- Total and Acute Uterine Inversion After Delivery: A Case ReportDocument5 pagesTotal and Acute Uterine Inversion After Delivery: A Case ReportMuhammad AzkaNo ratings yet
- Problems With The 4ps of LaborDocument10 pagesProblems With The 4ps of LaborhoohooNo ratings yet
- Antenatal Assessment of Fetal WellbeingDocument67 pagesAntenatal Assessment of Fetal WellbeingPaunami Dey50% (2)
- Post Partum Hemorrhage: Presented by Banita Rana Nursing Tutor SmvdconDocument27 pagesPost Partum Hemorrhage: Presented by Banita Rana Nursing Tutor SmvdconSahil Chadgal67% (3)
- Transient &tachypnea of The Newborn: Prepared By: Laith Abd Alhameed Jabar Supervised By: Dr. Oğr Üyesi Erdal ÜnlüDocument16 pagesTransient &tachypnea of The Newborn: Prepared By: Laith Abd Alhameed Jabar Supervised By: Dr. Oğr Üyesi Erdal ÜnlüAli FalihNo ratings yet
- NCM 107 Module 2FDocument15 pagesNCM 107 Module 2FFilane AntonetteNo ratings yet
- Managing FP Side Effects and Complications: Prepared by Tsiyon. K Jimma Ethiopia JULY 2021Document59 pagesManaging FP Side Effects and Complications: Prepared by Tsiyon. K Jimma Ethiopia JULY 2021Yonas AbebeNo ratings yet
- Postnatal Care PDF 66142082148037Document64 pagesPostnatal Care PDF 66142082148037veronia widayantiNo ratings yet
- Twin Anemia Polycythemia SyndromesDocument67 pagesTwin Anemia Polycythemia SyndromesBhupendra GuptaNo ratings yet
- Placenta Previa PathophysiologyDocument1 pagePlacenta Previa Pathophysiologykathy85% (20)
- Ertility RatesDocument3 pagesErtility RateslameshnamiwaNo ratings yet
- Apply The HBM and HPM in The Following SituationDocument1 pageApply The HBM and HPM in The Following SituationMary Ruth CruzNo ratings yet
- Hubungan Dukungan Suami Terhadap Tingkat Kecemasan Ibu Hamil Menjelang Persalinan Di Ruang Persalinan Rumah Sakit Umum Daerah Karanganyar Tahun 2017Document10 pagesHubungan Dukungan Suami Terhadap Tingkat Kecemasan Ibu Hamil Menjelang Persalinan Di Ruang Persalinan Rumah Sakit Umum Daerah Karanganyar Tahun 2017DianNo ratings yet
- Faktor Dominan Penyebab Kejadian Kekurangan Energi Kronik Pada Ibu HamilDocument16 pagesFaktor Dominan Penyebab Kejadian Kekurangan Energi Kronik Pada Ibu HamilZaki MubarokNo ratings yet
- Procedure Guide Leopold's ManeuverDocument3 pagesProcedure Guide Leopold's ManeuverAubrey Justine GaleonNo ratings yet
- Project Charter New 2pptDocument22 pagesProject Charter New 2pptashagrieNo ratings yet
- 21 038 Unfpa Sowmy2021 Report Env4302Document80 pages21 038 Unfpa Sowmy2021 Report Env4302Ainul Latifa100% (1)
- Congenital HydroceleDocument1 pageCongenital HydroceleVedant KumarNo ratings yet
- Postpartum Assessment (Bubblehed)Document2 pagesPostpartum Assessment (Bubblehed)skz19914No ratings yet
- Periodontal Infection and Preterm Low Birth Weight InfantsDocument31 pagesPeriodontal Infection and Preterm Low Birth Weight InfantsTamanna KalraNo ratings yet
- Demography: Sources of Demographic DataDocument8 pagesDemography: Sources of Demographic DataSHERMINA HASANNo ratings yet
- Module 1-5Document6 pagesModule 1-5Seika SouiNo ratings yet
- Drugs Used in ObstetricsDocument37 pagesDrugs Used in ObstetricsWhirmey ChinyamaNo ratings yet
- Accomplishment Report: CH 190: Community Practicum IDocument9 pagesAccomplishment Report: CH 190: Community Practicum ILourdes Yessamin MartejaNo ratings yet
- Aysha KhalilDocument55 pagesAysha Khalilayesha khalilNo ratings yet