NCP
NCP
Download as docx, pdf, or txt
At a glance
Powered by AI
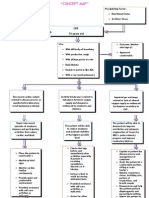
The document discusses nursing care for patients with decreased cardiac output and ineffective airway clearance, including assessments, goals, and nursing interventions.
Nursing interventions for a patient with decreased cardiac output include monitoring vital signs and lab results, giving oxygen, managing fluid balance, administering cardiac medications, encouraging rest, and patient education.
Nursing interventions for a patient with ineffective airway clearance include positioning, deep breathing exercises, suctioning, oxygen therapy, expectorant medications, and rest periods to promote airway clearance and reduce respiratory distress.
You might also like
- Lab ValuesDocument3 pagesLab Valuessurviving nursing school100% (3)
- High Sensitivity CRP - IMMULITE and IMMULITE 1000 - Rev 06 DXDCM 09017fe980297730-1538194293759Document36 pagesHigh Sensitivity CRP - IMMULITE and IMMULITE 1000 - Rev 06 DXDCM 09017fe980297730-1538194293759Deqsa Corporativo0% (1)
- NCP BronchopneumoniaDocument8 pagesNCP BronchopneumoniaCrisantaCasliNo ratings yet
- Concept Map - Abby !Document2 pagesConcept Map - Abby !Abegail Abaygar100% (3)
- The Impact of Social Media Powerpoint PresentationDocument36 pagesThe Impact of Social Media Powerpoint PresentationCamille Pineda60% (5)
- OSCE Station 1 Diabetic LL ExamDocument5 pagesOSCE Station 1 Diabetic LL ExamJeremy YangNo ratings yet
- Nursing Care Plan: General: Goals Met GenreralDocument3 pagesNursing Care Plan: General: Goals Met GenreralRomzy BasañesNo ratings yet
- Breast Self Exam BrochureDocument2 pagesBreast Self Exam Brochureapi-252329688100% (1)
- Impaired Tissue PerfusionDocument2 pagesImpaired Tissue PerfusionLyka Mae Imbat - PacnisNo ratings yet
- Decreased Cardiac OutputDocument4 pagesDecreased Cardiac OutputAdnan Khan100% (1)
- Healthcare - Nursing Care Plan - Excess Fluid VolumeDocument4 pagesHealthcare - Nursing Care Plan - Excess Fluid VolumeBenjamin CañalitaNo ratings yet
- Acute PainDocument3 pagesAcute PainJayr ChinNo ratings yet
- Assessment Diagnosis Scientific Explanation Objective Interventions Rationale Expected Outcome Short Term: Short TermDocument4 pagesAssessment Diagnosis Scientific Explanation Objective Interventions Rationale Expected Outcome Short Term: Short TermGensen Cu RoxasNo ratings yet
- Nursing Care PlanDocument4 pagesNursing Care Planapi-309251523No ratings yet
- NCPDocument2 pagesNCPNaidin Catherine De Guzman-AlcalaNo ratings yet
- Assessment Diagnosis Planning Nursing Intervention Rationale EvaluationDocument2 pagesAssessment Diagnosis Planning Nursing Intervention Rationale Evaluationjennelyn losantaNo ratings yet
- NCP Self CaRE DeficitDocument1 pageNCP Self CaRE Deficitnicole pageNo ratings yet
- Nursing Care PlanDocument3 pagesNursing Care PlanCrystelle MonaresNo ratings yet
- Ineffective Airway Clearance CareplanDocument6 pagesIneffective Airway Clearance CareplanderreshaNo ratings yet
- Nursing Care Plan - Mam EkaDocument7 pagesNursing Care Plan - Mam EkaGlenn Asuncion PagaduanNo ratings yet
- Nursing Care Plan Cues Nursing Diagnosis Objective Intervention Rationale Evaluation SubjectiveDocument2 pagesNursing Care Plan Cues Nursing Diagnosis Objective Intervention Rationale Evaluation SubjectiveFreisanChenMandumotanNo ratings yet
- Imbalanced NutritionDocument3 pagesImbalanced NutritionIlisa ParilNo ratings yet
- Nursing Care PlanDocument5 pagesNursing Care PlanPaola Marie VenusNo ratings yet
- NCP PTBDocument2 pagesNCP PTBMack Jhed AnarconNo ratings yet
- Excess Fluid Volume PPT (Case Press)Document10 pagesExcess Fluid Volume PPT (Case Press)Perrilyn PereyNo ratings yet
- San Francisco St. Butuan City 8600, Region XIII Caraga, PhilippinesDocument3 pagesSan Francisco St. Butuan City 8600, Region XIII Caraga, Philippineskuro hanabusaNo ratings yet
- Scribd 020922 Case Study-Oncology A&kDocument2 pagesScribd 020922 Case Study-Oncology A&kKellie DNo ratings yet
- NCP InfectionDocument3 pagesNCP InfectionPrince AhmirNo ratings yet
- Burns - Airway Clearance, Risk For IneffectiveDocument2 pagesBurns - Airway Clearance, Risk For Ineffectivemakyofrancis20No ratings yet
- Budget Plan For COPARDocument3 pagesBudget Plan For COPARPaolo Rafael D EsguerraNo ratings yet
- Assessment Diagnosis Planning Implementation Rationale EvaluationDocument3 pagesAssessment Diagnosis Planning Implementation Rationale EvaluationHanz AlecNo ratings yet
- NCP AirwayDocument2 pagesNCP AirwayjlucandoNo ratings yet
- Nursing Care PlanDocument4 pagesNursing Care PlanJobelyn TunayNo ratings yet
- Nursing Care Plan FinalDocument16 pagesNursing Care Plan FinalErickson OcialNo ratings yet
- Assignment For Oxy. Online BasedDocument5 pagesAssignment For Oxy. Online BasedNurhassem Nor AkangNo ratings yet
- NCP Ineffective Airway Clearance Related To The Accumulation of Secretions As Evidence by Decrease in Respiratory Rate and NGT and ET Tube Attached and Crackles at The Left Base of The LungsDocument3 pagesNCP Ineffective Airway Clearance Related To The Accumulation of Secretions As Evidence by Decrease in Respiratory Rate and NGT and ET Tube Attached and Crackles at The Left Base of The LungsSarah Ann Jamilla FaciolanNo ratings yet
- Nursing Care Plan 1: Diagnosis Goal Nursing Interventions RationaleDocument8 pagesNursing Care Plan 1: Diagnosis Goal Nursing Interventions RationaleTrysna Ayu Sukardi100% (1)
- NCP Copd4Document15 pagesNCP Copd4Alessa Marie Crisostomo Salazar100% (1)
- NCP TB MeningitisDocument1 pageNCP TB MeningitisMark Adrian D. DizorNo ratings yet
- Nursing Care Plan, Diagnosis, Interventions Hyperthermia, Fever, High TemperatureDocument2 pagesNursing Care Plan, Diagnosis, Interventions Hyperthermia, Fever, High TemperatureVanessa AbboudNo ratings yet
- NCPDocument5 pagesNCPRose AnnNo ratings yet
- Nursing Care Plan For LYING inDocument4 pagesNursing Care Plan For LYING inKarissa CiprianoNo ratings yet
- NCP BMDocument1 pageNCP BMSourabh MehraNo ratings yet
- Student NurseDocument2 pagesStudent NurseTAYABAN, KENNETH JAKE, Q.No ratings yet
- HTP of AsthmaDocument1 pageHTP of AsthmaMarland Faith Dela CruzNo ratings yet
- Rufino, Leslie Kriztel S. BSN 3-2 Group 1Document6 pagesRufino, Leslie Kriztel S. BSN 3-2 Group 1Deinielle Magdangal RomeroNo ratings yet
- Nursing Care Plan Renal FailureDocument18 pagesNursing Care Plan Renal FailureKundan KumarNo ratings yet
- NCP For StokeDocument5 pagesNCP For StokeMemedNo ratings yet
- Assessment Explanation of The Problem Planning Nursing Intervention Rationale EvaluationDocument2 pagesAssessment Explanation of The Problem Planning Nursing Intervention Rationale EvaluationRodolfo Bong SemaneroNo ratings yet
- MGH 8 - Ihd - NCPDocument12 pagesMGH 8 - Ihd - NCPSesinando Niez Quilao Jr.100% (1)
- Acute Renal Failure Nursing Care PlanDocument15 pagesAcute Renal Failure Nursing Care PlanRanusha AnushaNo ratings yet
- Impaired Physical Mobility R/T Neuromuscular ImpairmentDocument3 pagesImpaired Physical Mobility R/T Neuromuscular ImpairmentjisooNo ratings yet
- DHF NCP 2Document1 pageDHF NCP 2mavefigNo ratings yet
- NCP Blood Glucose Imbalance 4thDocument2 pagesNCP Blood Glucose Imbalance 4thRainier IbarretaNo ratings yet
- Nursing Care Plan: Group 4-Open Wound Head Injury After Debris FallDocument3 pagesNursing Care Plan: Group 4-Open Wound Head Injury After Debris FallNicole Villanueva, BSN - Level 3ANo ratings yet
- Wk2 NCP Edited2012Document6 pagesWk2 NCP Edited2012Jessely Caling SalasNo ratings yet
- Nursing Care PlanDocument3 pagesNursing Care PlanMarielle SorianoNo ratings yet
- NCP Acute PainDocument3 pagesNCP Acute PainNathalie kate petallarNo ratings yet
- Anatomy and Physiology PneumoniaDocument4 pagesAnatomy and Physiology PneumoniaJohnson MallibagoNo ratings yet
- Assessment of Patients in CCUDocument75 pagesAssessment of Patients in CCUShubham Singh Bisht100% (1)
- Assessment Diagnosis Planning Intervention Rationale Evaluation Subjective: Objective: Short Term: Independent: Short TermDocument3 pagesAssessment Diagnosis Planning Intervention Rationale Evaluation Subjective: Objective: Short Term: Independent: Short TermMicaela CrisostomoNo ratings yet
- NCPDocument3 pagesNCPJezza RequilmeNo ratings yet
- Welcome To The Case Study Presentation:-: Prostate CancerDocument22 pagesWelcome To The Case Study Presentation:-: Prostate CancerDengo ChapatieeNo ratings yet
- NCP-Case Presentation (CHF)Document4 pagesNCP-Case Presentation (CHF)Jessamine EnriquezNo ratings yet
- Nursing Care PlanDocument19 pagesNursing Care PlanChic Dian UsmanNo ratings yet
- NCPDocument22 pagesNCPMaricris S. Sampang100% (1)
- Health and Emergency Medical Services - MSRDocument37 pagesHealth and Emergency Medical Services - MSRCamille PinedaNo ratings yet
- Physical Assessment. - TyphoidDocument4 pagesPhysical Assessment. - TyphoidCamille PinedaNo ratings yet
- His T SpiritualityDocument83 pagesHis T SpiritualityCamille PinedaNo ratings yet
- Drug Study - LeptospirosisDocument19 pagesDrug Study - LeptospirosisCamille PinedaNo ratings yet
- Henrietta Lacks: Dr. Roz Iasillo Trinity High School River Forest, ILDocument13 pagesHenrietta Lacks: Dr. Roz Iasillo Trinity High School River Forest, ILRoz IasilloNo ratings yet
- Schizoaffective Disorder in The DSM 5 PDFDocument5 pagesSchizoaffective Disorder in The DSM 5 PDFpipiitopandabamboo247No ratings yet
- Pty 309Document2 pagesPty 309Geetanjali SaggarNo ratings yet
- Trigeminal Neuralgia (Agstri Dwi Marsela)Document11 pagesTrigeminal Neuralgia (Agstri Dwi Marsela)Agstri Dwi MarselaNo ratings yet
- Health SciencesDocument170 pagesHealth SciencesSabiran GibranNo ratings yet
- Endodontic TT OutcomesDocument22 pagesEndodontic TT OutcomesritikaNo ratings yet
- Medical EthicsDocument3 pagesMedical EthicsJona MagudsNo ratings yet
- Skradski Jaclyn CVDocument6 pagesSkradski Jaclyn CVapi-293245490No ratings yet
- Reporte Indicadores Proactivos y Reactivos Rev.2-1Document11 pagesReporte Indicadores Proactivos y Reactivos Rev.2-1Huber CallataNo ratings yet
- H21 261 2005eDocument26 pagesH21 261 2005eKartika Ramadhani BahriNo ratings yet
- Menstrual CycleDocument24 pagesMenstrual CycleMonika Bagchi100% (6)
- Aplastic AnemiaDocument16 pagesAplastic Anemiahazelposis100% (1)
- Resume 2021-6Document3 pagesResume 2021-6api-437078872100% (1)
- Vii. AssignmentDocument2 pagesVii. AssignmentRhodney BubudNo ratings yet
- MATS CurriculumDocument85 pagesMATS CurriculummamunpalashNo ratings yet
- Pharmacoeconomics: BY Mrs. K.Shailaja., M. Pharm., Lecturer Dept of Pharmacy Practice, SRM College of PharmacyDocument15 pagesPharmacoeconomics: BY Mrs. K.Shailaja., M. Pharm., Lecturer Dept of Pharmacy Practice, SRM College of Pharmacytsegaab yosephNo ratings yet
- Research EssayDocument13 pagesResearch Essayapi-609533251No ratings yet
- Laporan Diagnosa Pasien HarianDocument1 pageLaporan Diagnosa Pasien Hariansiti nurlailiyahNo ratings yet
- LP 8 Orif FemurDocument42 pagesLP 8 Orif FemurdaliaberseNo ratings yet
- The Mckenzie MethodDocument24 pagesThe Mckenzie MethodMohamed ElMeligieNo ratings yet
- The Ultimate Guide To Biohacking Exercise With Oxygen Therapy, Hypoxia, Elevation & Altitude TrainingDocument17 pagesThe Ultimate Guide To Biohacking Exercise With Oxygen Therapy, Hypoxia, Elevation & Altitude TrainingAlessandro QuercettiNo ratings yet
- Usage of Electronic Resources by The Medical, Dental and Paramedical Science Professionals in KarnatakaDocument7 pagesUsage of Electronic Resources by The Medical, Dental and Paramedical Science Professionals in KarnatakaSougata ChattopadhyayNo ratings yet
- Language For Understanding Covid19 Conversation Topics Dialogs Reading Comprehension 125476Document8 pagesLanguage For Understanding Covid19 Conversation Topics Dialogs Reading Comprehension 125476Deti Kurnia DewiNo ratings yet
- JRRMMC InternshipDocument48 pagesJRRMMC InternshipJason MontesaNo ratings yet
- Tetanus Case Discussion Draft 1Document22 pagesTetanus Case Discussion Draft 1Gio Tamaño BalisiNo ratings yet