Cardiac Study Guide
Cardiac Study Guide
Download as pdf or txt
You might also like
- The Borax ConspiracyDocument14 pagesThe Borax ConspiracyMiroslav Ilic92% (52)
- ECG Interpretation Cheat SheetDocument1 pageECG Interpretation Cheat Sheethirsi20051883% (30)
- Cardiac Dysrhythmia Chart Med-Surg NUR4Document3 pagesCardiac Dysrhythmia Chart Med-Surg NUR4ktfosterfd2095% (100)
- Cardiac DysrhythmiasDocument3 pagesCardiac DysrhythmiasKatherine Santiago92% (62)
- EKG ExamplesDocument9 pagesEKG ExamplesMayer Rosenberg99% (240)
- Cardiac DrugsDocument10 pagesCardiac DrugsNursePoor98% (53)
- Adult CCRN Exam Premium: Study Guide for the Latest Exam Blueprint, Includes 3 Practice Tests, Comprehensive Review, and Online Study PrepFrom EverandAdult CCRN Exam Premium: Study Guide for the Latest Exam Blueprint, Includes 3 Practice Tests, Comprehensive Review, and Online Study PrepNo ratings yet
- Could This Be Magic? Tattooing As Liberation WorkDocument68 pagesCould This Be Magic? Tattooing As Liberation Workem100% (1)
- Ecg Cheat Sheet 35Document2 pagesEcg Cheat Sheet 35jessjaylee80% (10)
- Cardiac Meds ChartDocument1 pageCardiac Meds ChartCharlotte Louise80% (5)
- EKG Cheat SheetDocument9 pagesEKG Cheat SheetAlert Twitter100% (10)
- ArrhythmiaDocument2 pagesArrhythmiaChris Pritchard94% (31)
- Cheat Sheet 1Document1 pageCheat Sheet 1Rick Frea100% (10)
- EKG | ECG Interpretation. Everything You Need to Know about 12-Lead ECG/EKG InterpretationFrom EverandEKG | ECG Interpretation. Everything You Need to Know about 12-Lead ECG/EKG InterpretationRating: 3 out of 5 stars3/5 (1)
- Cheetsheet 6Document1 pageCheetsheet 6Rick Frea92% (12)
- Haemodynamic Pocket GuideDocument2 pagesHaemodynamic Pocket GuideDarryl Betts86% (14)
- Cardiac Med ChartsDocument6 pagesCardiac Med ChartsNursingSchoolNotes100% (15)
- Cardiac DrugsDocument5 pagesCardiac Drugseric100% (18)
- Lab CheatsheetDocument1 pageLab CheatsheetRick Frea86% (7)
- UserManual-EN Version 4 Respons 910Document244 pagesUserManual-EN Version 4 Respons 910Deni Ardian100% (10)
- The 12-Lead Electrocardiogram for Nurses and Allied ProfessionalsFrom EverandThe 12-Lead Electrocardiogram for Nurses and Allied ProfessionalsNo ratings yet
- Surviving the ICU: A Toolkit for the Critical Care NurseFrom EverandSurviving the ICU: A Toolkit for the Critical Care NurseRating: 5 out of 5 stars5/5 (1)
- ECG Interpretation Cheat SheetDocument14 pagesECG Interpretation Cheat Sheetrenet_alexandre75% (8)
- Nursing: Lab Values: a QuickStudy Laminated 6-Page Reference GuideFrom EverandNursing: Lab Values: a QuickStudy Laminated 6-Page Reference GuideRating: 5 out of 5 stars5/5 (1)
- Ecg StripsDocument39 pagesEcg StripsNursyNurse100% (3)
- EKG | ECG: An Ultimate Step-By-Step Guide to 12-Lead EKG | ECG Interpretation, Rhythms & Arrhythmias Including Basic Cardiac DysrhythmiasFrom EverandEKG | ECG: An Ultimate Step-By-Step Guide to 12-Lead EKG | ECG Interpretation, Rhythms & Arrhythmias Including Basic Cardiac DysrhythmiasRating: 3 out of 5 stars3/5 (5)
- Acid-Base WorksheetDocument2 pagesAcid-Base WorksheetMayer Rosenberg100% (19)
- Basic Arrhythmia RulesDocument3 pagesBasic Arrhythmia Rulesgreenflames0997% (30)
- Dysrhythmias ChartDocument6 pagesDysrhythmias Chartjkrix100% (1)
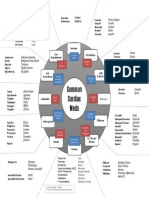
- Common Cardiac MedicationsDocument1 pageCommon Cardiac MedicationsPaige HardekopfNo ratings yet
- Cardiac Drugs Study Guide CourseDocument19 pagesCardiac Drugs Study Guide CourseAmanda Brittain100% (9)
- Critical Care Survival GuideDocument2 pagesCritical Care Survival Guidetringalama100% (5)
- Types of Assisted VentilationDocument1 pageTypes of Assisted VentilationJerry G100% (3)
- Dysrhythmia Recognition Pocket Reference Card PDFDocument14 pagesDysrhythmia Recognition Pocket Reference Card PDFjenn1722100% (3)
- Shoulderless Preliminary DraftDocument29 pagesShoulderless Preliminary Draftvrana23-1100% (2)
- ECG & EKG Interpretation: How to interpret ECG & EKG, including rhythms, arrhythmias, and more!From EverandECG & EKG Interpretation: How to interpret ECG & EKG, including rhythms, arrhythmias, and more!No ratings yet
- EKG and ECG Interpretation: Learn EKG Interpretation, Rhythms, and Arrhythmia Fast!From EverandEKG and ECG Interpretation: Learn EKG Interpretation, Rhythms, and Arrhythmia Fast!No ratings yet
- EKG Interpretation Basics Guide: Electrocardiogram Heart Rate Determination, Arrhythmia, Cardiac Dysrhythmia, Heart Block Causes, Symptoms, Identification and Medical Treatment Nursing HandbookFrom EverandEKG Interpretation Basics Guide: Electrocardiogram Heart Rate Determination, Arrhythmia, Cardiac Dysrhythmia, Heart Block Causes, Symptoms, Identification and Medical Treatment Nursing HandbookNo ratings yet
- Fluid and Electrolytes for Nursing StudentsFrom EverandFluid and Electrolytes for Nursing StudentsRating: 5 out of 5 stars5/5 (12)
- Advance Cardiac Life Support: Short, Sweet and to the PointFrom EverandAdvance Cardiac Life Support: Short, Sweet and to the PointRating: 3 out of 5 stars3/5 (2)
- A Simplified ECG GuideDocument4 pagesA Simplified ECG Guidejalan_z97% (30)
- Electrolyte CompleteDocument6 pagesElectrolyte CompleteTofan Ana100% (3)
- Cardiac DrugsDocument10 pagesCardiac Drugssurviving nursing school100% (4)
- Cardiac DisordersDocument15 pagesCardiac Disordersgold_enriquez100% (3)
- Critical Care NoteDocument10 pagesCritical Care NoteHanis Rozib99% (74)
- Cardiac NursingDocument26 pagesCardiac Nursingjgcriste95% (20)
- CO2 Pocket GuideDocument2 pagesCO2 Pocket GuideDarryl Betts100% (7)
- CCRN CardiacDocument39 pagesCCRN CardiacMike100% (5)
- Adult III Cardiac Study GuideDocument15 pagesAdult III Cardiac Study GuideNursingSchoolNotes100% (6)
- Nursing Mnemonics: The Ultimate Tips and Notes For NursesFrom EverandNursing Mnemonics: The Ultimate Tips and Notes For NursesRating: 5 out of 5 stars5/5 (1)
- EKG/ECG Interpretation Made Easy: A Practical Approach to Passing the ECG/EKG Portion of NCLEXFrom EverandEKG/ECG Interpretation Made Easy: A Practical Approach to Passing the ECG/EKG Portion of NCLEXRating: 5 out of 5 stars5/5 (2)
- Ccrn Certification Examination Practice Questions and Answers with Rationale: First EditionFrom EverandCcrn Certification Examination Practice Questions and Answers with Rationale: First EditionRating: 5 out of 5 stars5/5 (1)
- Bonehead Electrocardiography: The Easiest and Best Way to Learn How to Read Electrocardiograms—No Bones About It!From EverandBonehead Electrocardiography: The Easiest and Best Way to Learn How to Read Electrocardiograms—No Bones About It!Rating: 5 out of 5 stars5/5 (2)
- Hemodynamic Rounds: Interpretation of Cardiac Pathophysiology from Pressure Waveform AnalysisFrom EverandHemodynamic Rounds: Interpretation of Cardiac Pathophysiology from Pressure Waveform AnalysisNo ratings yet
- Objectives of Economic PlanningDocument13 pagesObjectives of Economic PlanningNivriti Seth100% (1)
- NutritionDocument34 pagesNutritionOluwachidiNo ratings yet
- Brinlee Et Al ACL Guidelines Paper - SportsHealth - 2021Document10 pagesBrinlee Et Al ACL Guidelines Paper - SportsHealth - 2021Antoine ClyNo ratings yet
- Attachment 1610172742-1 CompressedDocument114 pagesAttachment 1610172742-1 CompressedSaqib MansuriNo ratings yet
- Weapons of Mass DestructionDocument41 pagesWeapons of Mass DestructionRexchel Nicole P. AlvarezNo ratings yet
- CJLS Hammer On Smoking - Final As ApprovedDocument22 pagesCJLS Hammer On Smoking - Final As ApprovedAgustin MarcoffNo ratings yet
- Newborn ReflexesDocument2 pagesNewborn ReflexesNEil モラレスNo ratings yet
- VetDocument77 pagesVetFeritFazliuNo ratings yet
- Neha Sharma - 31862159 - 9 12 2018 - 18 9 PDFDocument2 pagesNeha Sharma - 31862159 - 9 12 2018 - 18 9 PDFAnonymous ClNzkEwgVJNo ratings yet
- Histology of Pancreas by Dr. RoomiDocument20 pagesHistology of Pancreas by Dr. RoomiMudassar Roomi100% (1)
- Radiologist in GwaliorDocument8 pagesRadiologist in GwaliorshahulNo ratings yet
- High Containment Labs and Other Facilities of The US Bio Defense ProgramDocument1 pageHigh Containment Labs and Other Facilities of The US Bio Defense ProgramHRCNo ratings yet
- A) MarasmusDocument21 pagesA) Marasmusrathai0% (1)
- How Behavior Spreads Centola en 44325Document6 pagesHow Behavior Spreads Centola en 44325ytuncer19No ratings yet
- Laboratory Report - Cow GheeDocument4 pagesLaboratory Report - Cow GheeBalajiDussaNo ratings yet
- Covidien BISDocument5 pagesCovidien BISmunchen88No ratings yet
- Marketing Strategies of Insurance Companies in Us, Uk, India EtcDocument15 pagesMarketing Strategies of Insurance Companies in Us, Uk, India EtclegendarystuffNo ratings yet
- Assay of Ascorbic Acid in Vitamin C SyrupDocument6 pagesAssay of Ascorbic Acid in Vitamin C SyrupOyemomi Samuel AdeyemiNo ratings yet
- IMI Level 2 Assessment CriteriaDocument89 pagesIMI Level 2 Assessment CriteriaTrevorNo ratings yet
- Simple White Bean Hummus - The Simple VeganistaDocument2 pagesSimple White Bean Hummus - The Simple VeganistaAshNo ratings yet
- Foundation of Special Education 1Document26 pagesFoundation of Special Education 1Lyle Padua100% (1)
- RemarkDocument3 pagesRemarkMuhammad tholhah AzamNo ratings yet
- Nail Structure and Conditions Diseases and DisorderDocument6 pagesNail Structure and Conditions Diseases and DisorderCris Cali EspeNo ratings yet
- Cca 2024 Codebook List Updated2-23Document2 pagesCca 2024 Codebook List Updated2-23chaitanya varmaNo ratings yet
- Cube Method SpreadsheetDocument12 pagesCube Method SpreadsheetLujack McIntyre100% (1)
- Aci 440Document5 pagesAci 440Debora AraújoNo ratings yet