Prematurely Ruptured of Membranes - PROM
Prematurely Ruptured of Membranes - PROM
Download as pdf or txt
You might also like
- Www. Bobcat-: Service Manual T190 Compact Track LoaderDocument888 pagesWww. Bobcat-: Service Manual T190 Compact Track LoaderRene CuencaNo ratings yet
- ENG TECH 4MA3 Assignment 2020 FallDocument6 pagesENG TECH 4MA3 Assignment 2020 FallRyan TorresNo ratings yet
- Fireground HydraulicsDocument114 pagesFireground HydraulicsNaeem IqbalNo ratings yet
- 2022 Mathematics Atp Grade 7Document7 pages2022 Mathematics Atp Grade 7Themba NyoniNo ratings yet
- Induction and Augmentation of LaborDocument22 pagesInduction and Augmentation of LaborDagnachew kasaye100% (2)
- Supreme Magus Volume 3Document5 pagesSupreme Magus Volume 3eliasNo ratings yet
- Prematurely Ruptured of Membranes (PROM)Document23 pagesPrematurely Ruptured of Membranes (PROM)NiNie Sie MbakayuNeNo ratings yet
- Premature Rupture of MembranesDocument29 pagesPremature Rupture of MembranesIda YosopaNo ratings yet
- Premature Rupture of Membranes (PROM)Document22 pagesPremature Rupture of Membranes (PROM)vishnu mugilNo ratings yet
- PromDocument28 pagesPromSemon YohannesNo ratings yet
- Premature Rupture of MembranesDocument33 pagesPremature Rupture of MembranesSarang Lee100% (1)
- Prom 1Document48 pagesProm 1Tesfahun TekleNo ratings yet
- 24 Intrauterine Fetal Growth Restriction and Amniotic Fluid DisordersDocument23 pages24 Intrauterine Fetal Growth Restriction and Amniotic Fluid DisordersÕbsëqúiœus Menam MikreNo ratings yet
- Induction and AugmentationDocument50 pagesInduction and AugmentationchabsidarbiNo ratings yet
- Premature Rupture of The MembranesDocument6 pagesPremature Rupture of The MembranesMaria Donabella OngueNo ratings yet
- 18 PromDocument8 pages18 PromRyubusa HayabusaNo ratings yet
- Management of PPROM Edit 1Document45 pagesManagement of PPROM Edit 1lohujiherNo ratings yet
- Premature Rupture of MembranesDocument38 pagesPremature Rupture of MembranesArwa QishtaNo ratings yet
- Obgy-Wln Late Pregnancy Complications: Kabwe Central HospitalDocument15 pagesObgy-Wln Late Pregnancy Complications: Kabwe Central HospitalEmmanuel MukukaNo ratings yet
- Preterm Labour: Introduction and Causes by Humna AnisDocument19 pagesPreterm Labour: Introduction and Causes by Humna AnisManjunath VankadariNo ratings yet
- KPSW Dan Sepsis Kemayoran 160719Document54 pagesKPSW Dan Sepsis Kemayoran 160719budiNo ratings yet
- Preterm LaborDocument29 pagesPreterm LaborBer AnneNo ratings yet
- Preterm Pre-Labour Rupture of MembranesDocument48 pagesPreterm Pre-Labour Rupture of Membranesnyiramahirwe theodetteNo ratings yet
- Premature Rupture of MembranesDocument39 pagesPremature Rupture of MembranesROLEX JUMANo ratings yet
- PROM (Prelabor Rupture of Membranes)Document20 pagesPROM (Prelabor Rupture of Membranes)lohujiherNo ratings yet
- Complications of 3rd TrimesterDocument49 pagesComplications of 3rd TrimesterMA. JYRELL BONITONo ratings yet
- Pprom 1 1Document20 pagesPprom 1 1Tehreem Azhar100% (1)
- Management of Abortion,Unsafe Abortion, Post Abortal CareDocument33 pagesManagement of Abortion,Unsafe Abortion, Post Abortal Carebentley.wes78No ratings yet
- Premature RuptureDocument30 pagesPremature RuptureSanthosh.S.U100% (1)
- Preterm Labour and PROMDocument25 pagesPreterm Labour and PROMNinaNo ratings yet
- Ob EmergenciesDocument58 pagesOb Emergenciessanthiyasandy100% (2)
- Gyno... PTL & PRODocument30 pagesGyno... PTL & PROhailemichael chekolNo ratings yet
- Preterm Labour: Pembimbing: Dr. Andriana Kumala Dewi, SP - OGDocument33 pagesPreterm Labour: Pembimbing: Dr. Andriana Kumala Dewi, SP - OGJovian LutfiNo ratings yet
- Premature Rupture of The MembranesDocument21 pagesPremature Rupture of The MembranesMeta SariNo ratings yet
- Preterm Labor-1Document28 pagesPreterm Labor-1tajfaiz779No ratings yet
- Induction Obstructed PrecipitateDocument38 pagesInduction Obstructed PrecipitateRose NyamburaNo ratings yet
- Preterm LaborDocument62 pagesPreterm LaborAstri Sri Widiastuty100% (1)
- Induction of LabourDocument59 pagesInduction of LabourFadiaislamiNo ratings yet
- PRETERM DELIVERY With NARRATIONDocument23 pagesPRETERM DELIVERY With NARRATIONamanda deonananNo ratings yet
- Fetal Dev, AbortionDocument128 pagesFetal Dev, AbortionAr JayNo ratings yet
- Premature Rapture of Membrane.Document13 pagesPremature Rapture of Membrane.Sadia SiddikiNo ratings yet
- Amniotic Fluid DisordersDocument22 pagesAmniotic Fluid Disordersvictor onapaNo ratings yet
- PROM SANJIDA FInal 2Document32 pagesPROM SANJIDA FInal 2Saiful islam RonyNo ratings yet
- Abortion, Ectopic PregnancyDocument139 pagesAbortion, Ectopic PregnancyINFORMASI MENARIK100% (1)
- Premature Rupture of MembraneDocument17 pagesPremature Rupture of MembraneShimaa Abdel hameedNo ratings yet
- Mummification Maceration PyometraDocument16 pagesMummification Maceration PyometrafeyisaNo ratings yet
- Prelabor Rupture of Membranes (Prom) : By-Aditi Grover Roll No. - 3Document12 pagesPrelabor Rupture of Membranes (Prom) : By-Aditi Grover Roll No. - 3San SiddzNo ratings yet
- Maternal HealthDocument90 pagesMaternal HealthShaafieNo ratings yet
- PhimosisDocument36 pagesPhimosisNamrata Karki100% (2)
- Management of Pregnancy With Premature Rupture of Membranes (Prom)Document6 pagesManagement of Pregnancy With Premature Rupture of Membranes (Prom)Ryzka Izza MayFanyNo ratings yet
- PromDocument45 pagesPromgaredewasnakeayeleNo ratings yet
- Recurrent Miscarriage - Pregnancy LossDocument34 pagesRecurrent Miscarriage - Pregnancy Losszianab aliNo ratings yet
- PPROMDocument12 pagesPPROMBright KumwendaNo ratings yet
- Nursing Care of Clients With Reproductive Health ProblemsDocument100 pagesNursing Care of Clients With Reproductive Health ProblemsHassen ZabalaNo ratings yet
- 14 Postterm Pregnancy and Intrauterine Fetal DeathDocument25 pages14 Postterm Pregnancy and Intrauterine Fetal DeathÕbsëqúiœus Menam MikreNo ratings yet
- MultigravidaDocument25 pagesMultigravidaMukund ChauhanNo ratings yet
- Female Sub FertilityDocument75 pagesFemale Sub FertilityIshaThapa100% (1)
- 05b KPSW Dan SepsisDocument34 pages05b KPSW Dan SepsisIsmi RatnasariNo ratings yet
- Multiple Pregnancy: Nirav Hitesh Kumar ValandDocument28 pagesMultiple Pregnancy: Nirav Hitesh Kumar ValandNirav SharmaNo ratings yet
- University of Saint Louis Tuguegarao City, Philippines: Maternal and Child Health NursingDocument94 pagesUniversity of Saint Louis Tuguegarao City, Philippines: Maternal and Child Health NursingErica Veluz LuyunNo ratings yet
- Google 4Document5 pagesGoogle 4sintaraNo ratings yet
- Bleeding in Early PregnancyDocument34 pagesBleeding in Early PregnancyAdenike OLAOGUNNo ratings yet
- Preterm Labour - PgDocument43 pagesPreterm Labour - PglakshyaavuppalaNo ratings yet
- Lecture 11 Bovine and Bubaline Infertility-Non-specific Genital AffectionsDocument54 pagesLecture 11 Bovine and Bubaline Infertility-Non-specific Genital AffectionsgnpobsNo ratings yet
- List of MaterialDocument3 pagesList of MaterialAchmed Farrin OthmanNo ratings yet
- Module Lesson 3 Equipments in BadmintonDocument8 pagesModule Lesson 3 Equipments in BadmintonJerald CañeteNo ratings yet
- SondagaandeDocument5 pagesSondagaandedh8phkyjdtNo ratings yet
- DGS 700 ManualDocument28 pagesDGS 700 Manualcarla monic dialinoNo ratings yet
- Beige Brown Playful Cute Illustration October Monthly Planner Journal Agenda PresentationDocument20 pagesBeige Brown Playful Cute Illustration October Monthly Planner Journal Agenda Presentation2w2tkd2ptbNo ratings yet
- Packaging Present. FinalDocument34 pagesPackaging Present. FinalJitendra Yadav0% (1)
- Food Waste in Rst. Pakistan PDFDocument21 pagesFood Waste in Rst. Pakistan PDFKaruna DhuttiNo ratings yet
- Unit Test 4BDocument6 pagesUnit Test 4BTania CorreiaNo ratings yet
- Care of Spinal Injury Patient With Paraplegia and QuadriplegiaDocument54 pagesCare of Spinal Injury Patient With Paraplegia and Quadriplegia21.FARHANI100% (1)
- Risk Assessment in Livestock Supply Chain Using The MCDM Method: A Case of Emerging EconomyDocument16 pagesRisk Assessment in Livestock Supply Chain Using The MCDM Method: A Case of Emerging EconomyAsrullah AsNo ratings yet
- IO Manual E4Document48 pagesIO Manual E4V.A. Elvien Kristian PrasetyoNo ratings yet
- Animals Everywhere Grammar Drills Picture Description Exercises Readi 98317Document2 pagesAnimals Everywhere Grammar Drills Picture Description Exercises Readi 98317anagalac2344No ratings yet
- TRL2604 Study NotesDocument46 pagesTRL2604 Study Notesabdessamadlotfi02No ratings yet
- Zxtec Tension ControllerDocument16 pagesZxtec Tension ControllerNisar AhmedNo ratings yet
- NCS001 (E) SugarDocument38 pagesNCS001 (E) Sugarrudy_423522658No ratings yet
- Civil Enforcement Handbook V 2Document56 pagesCivil Enforcement Handbook V 2Olaf RazzoliNo ratings yet
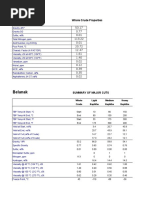
- Belanak: Whole Crude PropertiesDocument6 pagesBelanak: Whole Crude PropertiesHeron SurbaktiNo ratings yet
- The ColorDisk 1.5Document1 pageThe ColorDisk 1.5ad cruzNo ratings yet
- The Quality of Life in Post - Mucormycosis PatientDocument4 pagesThe Quality of Life in Post - Mucormycosis PatientInternational Journal of Innovative Science and Research Technology100% (1)
- Amp & Cab Model List - Help CenterDocument1 pageAmp & Cab Model List - Help CenterGAMES TORRENTNo ratings yet
- NavEdit ManualDocument52 pagesNavEdit ManualDaeng KulleNo ratings yet
- Corrosion Science: L.Y. Xu, Y.F. ChengDocument7 pagesCorrosion Science: L.Y. Xu, Y.F. ChengHaniel FcNo ratings yet
- Procter & Gamble: Using Agent Based Modeling and RFID: Supply Chain ManagementDocument18 pagesProcter & Gamble: Using Agent Based Modeling and RFID: Supply Chain ManagementJames KudrowNo ratings yet
- Mechanics of Materials Lab Fall 2018Document52 pagesMechanics of Materials Lab Fall 2018Hammad RazaNo ratings yet
- How To Save Power by Induction MotorDocument3 pagesHow To Save Power by Induction Motorshamim islamNo ratings yet