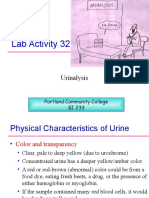
Urinalysis
Urinalysis
Download as doc, pdf, or txt
You might also like
- Eliade, Mircea - Tales of The Sacred and The Supernatural PDFDocument109 pagesEliade, Mircea - Tales of The Sacred and The Supernatural PDFpooka john100% (8)
- Color Atlas of Emergency TraumaDocument314 pagesColor Atlas of Emergency TraumaIacob Razvan78% (9)
- DHA General 03/03/2021: c-90-120 DaysDocument6 pagesDHA General 03/03/2021: c-90-120 DaysMONFOLA100% (1)
- LemarDocument12 pagesLemarViny ManyaNo ratings yet
- Urinalysis Sample Report With Notes - 0Document1 pageUrinalysis Sample Report With Notes - 0sukanto bagchiNo ratings yet
- Exploring Amylase Substrate Specificity: Physioex Exercise 8: Activity 2Document3 pagesExploring Amylase Substrate Specificity: Physioex Exercise 8: Activity 2Linette GuillermoNo ratings yet
- Pediatrics Care Plan Kawasaki Disease Final Draft and CorrectedDocument9 pagesPediatrics Care Plan Kawasaki Disease Final Draft and CorrectedValencia Vickers50% (4)
- Swu Phinma, College of Pharmacy 2020: Wr/Urinalysis - Html#Ixzz6Zxlj RQKH /Product-Manual/3008 - 3B - UrinalysisDocument7 pagesSwu Phinma, College of Pharmacy 2020: Wr/Urinalysis - Html#Ixzz6Zxlj RQKH /Product-Manual/3008 - 3B - UrinalysisTrex MarciiiNo ratings yet
- Routine UrinalysisDocument4 pagesRoutine UrinalysisDanica Joy Christelle L. PilarNo ratings yet
- Chapter Four: Chemical Analysis of UrineDocument211 pagesChapter Four: Chemical Analysis of UrineErenjaeger TitanNo ratings yet
- Clinical Chemistry Lecture KayzardnDocument3 pagesClinical Chemistry Lecture KayzardnHenry QuimbaNo ratings yet
- Lesson 5: Nature of The Clinical LaboratoryDocument8 pagesLesson 5: Nature of The Clinical LaboratoryJohn Daniel AriasNo ratings yet
- Serology Review: M LAB 2361 Clinical IIDocument17 pagesSerology Review: M LAB 2361 Clinical IIkiskawhiteNo ratings yet
- Urinalysis 150313040235 Conversion Gate01Document30 pagesUrinalysis 150313040235 Conversion Gate01AbhishiktaAbhi100% (2)
- Aub F Urine Screening For Metabolic DisordersDocument4 pagesAub F Urine Screening For Metabolic DisordersRomie SolacitoNo ratings yet
- CC - DAY 4 - PRE-TEST RationalizationDocument21 pagesCC - DAY 4 - PRE-TEST RationalizationVincent AmitNo ratings yet
- A. B. C. A. B. C. D.: Clinical Chemistry II - Prelims (Bandala)Document19 pagesA. B. C. A. B. C. D.: Clinical Chemistry II - Prelims (Bandala)IceNo ratings yet
- Laboratory Diagnosis of Parasitic DiseasesDocument57 pagesLaboratory Diagnosis of Parasitic DiseasesAmanuel MaruNo ratings yet
- CC1P S Weier - OsmometryDocument17 pagesCC1P S Weier - OsmometrySaad KhanNo ratings yet
- ConclusionDocument2 pagesConclusionOMMONANo ratings yet
- Micropara Final LabNotesDocument75 pagesMicropara Final LabNotescream oNo ratings yet
- Clearance and GFR: Major DR Arabinda Mohan Bhattarai Lecturer (Biochemistry), NAIHSDocument25 pagesClearance and GFR: Major DR Arabinda Mohan Bhattarai Lecturer (Biochemistry), NAIHSChandan SahNo ratings yet
- Aubf Case Study AbcdefDocument9 pagesAubf Case Study AbcdefChiara Kate CodillaNo ratings yet
- Question Excerpt From Clinical ChemistryDocument3 pagesQuestion Excerpt From Clinical Chemistryeebrej100% (1)
- Giardia PPT M.SC Medical 4th SemDocument16 pagesGiardia PPT M.SC Medical 4th SemRahul ChaudharyNo ratings yet
- 3 Concentration Techniques SedimentationDocument18 pages3 Concentration Techniques SedimentationFatihah JahsmiNo ratings yet
- Alkaline PH Acid PH N Amorphous Phosphate Uric AcidDocument3 pagesAlkaline PH Acid PH N Amorphous Phosphate Uric AcidSurriya NawazNo ratings yet
- Solving The Bacterial UnknownDocument14 pagesSolving The Bacterial UnknownDenisse Watt Cuarteros100% (1)
- Complete Bacteriology 240302 021020Document2,416 pagesComplete Bacteriology 240302 021020Usama HameedNo ratings yet
- Urine and Blood PPT (Handout Print Form) Chua, RDocument10 pagesUrine and Blood PPT (Handout Print Form) Chua, RKirsten Hazel Mejia100% (1)
- Intestinal FlagellatesDocument5 pagesIntestinal Flagellatesdhainey100% (3)
- Lab Activity No. 1 - Hemoglobin DeterminationDocument2 pagesLab Activity No. 1 - Hemoglobin DeterminationChelsea Padilla Delos ReyesNo ratings yet
- MED TECH Clinical ChemistryDocument3 pagesMED TECH Clinical ChemistryJan Martin Mogueis JustoNo ratings yet
- Buenviaje-HEAT AND ACETIC ACID TESTDocument7 pagesBuenviaje-HEAT AND ACETIC ACID TESTrio salvadorNo ratings yet
- Prelims Week 3 - Urinalysis - TransDocument16 pagesPrelims Week 3 - Urinalysis - TransLoro JDNo ratings yet
- Lab 2 - Microscopy and The CellDocument44 pagesLab 2 - Microscopy and The CellNatalie Pemberton100% (1)
- OsmometryDocument6 pagesOsmometryVERMADEEN0% (1)
- ASM StyleDocument3 pagesASM Stylemicroreader100% (1)
- Hematology Exam 2017Document7 pagesHematology Exam 2017Rye CalderonNo ratings yet
- 4 - HemoglobinopathiesDocument19 pages4 - HemoglobinopathiesHamzehNo ratings yet
- Understanding StoolDocument6 pagesUnderstanding StoolJonni Arianto RangkutyNo ratings yet
- Gel TechnologyDocument2 pagesGel TechnologyJai Carungay100% (1)
- ENZYMOLOGYDocument2 pagesENZYMOLOGYCarla Lagar FloresNo ratings yet
- Parasitology PrelimsDocument47 pagesParasitology PrelimsKim Delaney MadridNo ratings yet
- Hematology 1 Lab - The Reticulocyte CountDocument17 pagesHematology 1 Lab - The Reticulocyte CountCIRILO MABBORANGNo ratings yet
- MT LawsDocument8 pagesMT LawsKathleen Javier AngcayaNo ratings yet
- CC Partii&III NotesDocument30 pagesCC Partii&III NotesAnielle Mongaya100% (1)
- Staphylococcus VS, StreptococcusDocument5 pagesStaphylococcus VS, StreptococcuschokasaNo ratings yet
- PopcornDocument41 pagesPopcorntrixia therese00No ratings yet
- AUBF Analysis of Urine and Body FluidsDocument581 pagesAUBF Analysis of Urine and Body FluidsQuetzaL coatL100% (1)
- Clinial MicrosDocument53 pagesClinial MicrosDreyden HaloNo ratings yet
- 3a.6 Aspartate Aminotransferase DeterminationDocument7 pages3a.6 Aspartate Aminotransferase Determinationiridescent brightwinNo ratings yet
- CC Lab 6 TransesDocument6 pagesCC Lab 6 TransesCiara PamonagNo ratings yet
- Cc2 Lec 13 Trace ElementsDocument21 pagesCc2 Lec 13 Trace ElementsJunea See100% (1)
- MLS322L - Module7 - Platelet Estimation - 0958CL - Gundayao - John Bernard EizersonDocument3 pagesMLS322L - Module7 - Platelet Estimation - 0958CL - Gundayao - John Bernard EizersonJB GundayaoNo ratings yet
- Chemical Examination of UrineDocument17 pagesChemical Examination of Urinekaran kambojNo ratings yet
- Post Lab 01-09Document7 pagesPost Lab 01-09Patrick ParconNo ratings yet
- Topic 5. MEDICAL TECHNOLOGY EDUCATIONDocument7 pagesTopic 5. MEDICAL TECHNOLOGY EDUCATIONSophia GarciaNo ratings yet
- CM CoachingDocument24 pagesCM CoachingGwynne Velasquez100% (1)
- Blood BankDocument10 pagesBlood BankMarie LlanesNo ratings yet
- Isolation and Characterization of Egg ProteinsDocument6 pagesIsolation and Characterization of Egg ProteinsJason Raquin Roque100% (4)
- Abo and MN Blood Group SystemDocument54 pagesAbo and MN Blood Group SystemAkram chaudaryNo ratings yet
- Tietz's Applied Laboratory MedicineFrom EverandTietz's Applied Laboratory MedicineMitchell G. ScottRating: 3 out of 5 stars3/5 (1)
- UrinalysisDocument10 pagesUrinalysisMichelle100% (2)
- Soil Diversity: Experiment 6Document19 pagesSoil Diversity: Experiment 6Linette GuillermoNo ratings yet
- PGC Schedule: Section: 4B1 Date Activities Topic Reminders/ Due Submission April 4, MondayDocument6 pagesPGC Schedule: Section: 4B1 Date Activities Topic Reminders/ Due Submission April 4, MondayLinette GuillermoNo ratings yet
- The Philippine Political SystemDocument2 pagesThe Philippine Political SystemLinette Guillermo100% (1)
- Pex 08 02Document4 pagesPex 08 02Linette Guillermo90% (10)
- Presidential EssayDocument10 pagesPresidential EssayLinette GuillermoNo ratings yet
- Pex 08 04Document4 pagesPex 08 04Linette Guillermo64% (11)
- Experiment 5. Soil CharacerizationDocument6 pagesExperiment 5. Soil CharacerizationMatthew SANo ratings yet
- Pex 08 03Document4 pagesPex 08 03Charles Patrice Isaupu Gansang50% (2)
- Pex 08 01Document4 pagesPex 08 01Linette Guillermo92% (12)
- Exercise 4. Terrestrial Sampling TechniquesDocument11 pagesExercise 4. Terrestrial Sampling TechniquesMatthew SANo ratings yet
- Elisa (Enzyme Linked Immunosorbant Assay)Document4 pagesElisa (Enzyme Linked Immunosorbant Assay)Linette GuillermoNo ratings yet
- Experiment 6. Intro ObjDocument3 pagesExperiment 6. Intro ObjLinette GuillermoNo ratings yet
- Experiment 6 - Intro-ObjDocument3 pagesExperiment 6 - Intro-ObjLinette GuillermoNo ratings yet
- Mucic Acid TestDocument5 pagesMucic Acid TestLinette Guillermo75% (4)
- Erase E WasteDocument7 pagesErase E WasteLinette GuillermoNo ratings yet
- CH 600 LC Name: Problem Set Yr. & Sec: Enzymes ANSWER THE FOLLOWING QUESTIONS. Use Yellow Pad For Your AnswersDocument2 pagesCH 600 LC Name: Problem Set Yr. & Sec: Enzymes ANSWER THE FOLLOWING QUESTIONS. Use Yellow Pad For Your AnswersLinette GuillermoNo ratings yet
- EthicsDocument1 pageEthicsLinette GuillermoNo ratings yet
- HND Unit 18 - Voice & Speech For ActorsDocument8 pagesHND Unit 18 - Voice & Speech For Actorsstuart_murray_22No ratings yet
- One Thousand Mcq's ADCDocument84 pagesOne Thousand Mcq's ADCboreddentist83% (6)
- Assignment On Cells and Stem CellsDocument10 pagesAssignment On Cells and Stem CellsMohammad MashhoodNo ratings yet
- Yoga PDFDocument31 pagesYoga PDFAlvin IvanNo ratings yet
- Diazepam CompiledDocument41 pagesDiazepam CompiledyayayanizaNo ratings yet
- 3.4 Process of Absorption and Transportation of Digested Food and DefecationDocument9 pages3.4 Process of Absorption and Transportation of Digested Food and DefecationYu Xuan ChongNo ratings yet
- Museum of Human Anatomy Luigi RolandoDocument2 pagesMuseum of Human Anatomy Luigi RolandoFrankNo ratings yet
- Case Study - SisDocument14 pagesCase Study - Sisclara_wenceslaoNo ratings yet
- DiverticulosisDocument9 pagesDiverticulosisSyafiq Shahbudin100% (1)
- Heart Railway RPF by Radhika MamDocument70 pagesHeart Railway RPF by Radhika Mamyakshat.4141ykNo ratings yet
- Cells: The Basic Units of LifeDocument17 pagesCells: The Basic Units of LifeglezamaeNo ratings yet
- Current Use of Resuscitative Endovascular Balloon Occlusion of The Aorta (REBOA) in Trauma?Document9 pagesCurrent Use of Resuscitative Endovascular Balloon Occlusion of The Aorta (REBOA) in Trauma?Luis-alfredo Perez Bolde HernandezNo ratings yet
- Reviewer in PE 2Document3 pagesReviewer in PE 2Marjorie Jacinto CruzinNo ratings yet
- Uworld: Maria Elizabeth SharmaDocument87 pagesUworld: Maria Elizabeth SharmaElizabeth SharmaNo ratings yet
- Capstone Case Study Final - CHFDocument3 pagesCapstone Case Study Final - CHFapi-351999622No ratings yet
- Prostho IV Slide 3 Impression Making For Complete DenturesDocument82 pagesProstho IV Slide 3 Impression Making For Complete DenturesBoka BokaNo ratings yet
- Common Abbrevia-WPS OfficeDocument8 pagesCommon Abbrevia-WPS OfficeChristian Nicolas RabagoNo ratings yet
- DLP Gen - BiologyDocument4 pagesDLP Gen - BiologyGina Ano IsidroNo ratings yet
- Intestinal Colonisation, Microbiota and Future Probiotics?: Original ArticleDocument5 pagesIntestinal Colonisation, Microbiota and Future Probiotics?: Original ArticleSherif Abou BakrNo ratings yet
- Curriculum Vitae Richard L. Doty: WWW - Med.upenn - Edu/stcDocument60 pagesCurriculum Vitae Richard L. Doty: WWW - Med.upenn - Edu/stcSri KarthickNo ratings yet
- Franks Houston 2017Document29 pagesFranks Houston 2017Donnell FrancisNo ratings yet
- Anaphy QuizzesDocument5 pagesAnaphy QuizzesElvira MirajulNo ratings yet
- Notes by María Penado From UNED PsychobiologyDocument37 pagesNotes by María Penado From UNED PsychobiologyScribdTranslationsNo ratings yet
- Cardiac MonitorDocument3 pagesCardiac MonitorShameera M. KamlianNo ratings yet
- Female Reproductive SystemDocument40 pagesFemale Reproductive SystemSAYMABANUNo ratings yet
- June 2023 (v3) QP - Paper 4 CAIE Biology IGCSEDocument20 pagesJune 2023 (v3) QP - Paper 4 CAIE Biology IGCSEceline.the988No ratings yet
- Moxa PaperDocument20 pagesMoxa PaperG.100% (1)