This document provides information on mitral stenosis (MS) and mitral regurgitation (MR). It begins by describing the etiology of MS, which is primarily rheumatic fever resulting in scarring and fusion of the mitral valve. It then discusses the pathophysiology of MS, leading to right heart failure and pulmonary hypertension. Symptoms, physical exam findings, and treatments including medical management, balloon valvuloplasty, and surgical options are summarized. For MR, common causes include myxomatous disease, rheumatic fever, and ischemic or congenital etiologies. The pathophysiology of chronic MR is described. Methods for assessing MR severity including echocardiography are provided, along with recommendations
This document provides information on mitral stenosis (MS) and mitral regurgitation (MR). It begins by describing the etiology of MS, which is primarily rheumatic fever resulting in scarring and fusion of the mitral valve. It then discusses the pathophysiology of MS, leading to right heart failure and pulmonary hypertension. Symptoms, physical exam findings, and treatments including medical management, balloon valvuloplasty, and surgical options are summarized. For MR, common causes include myxomatous disease, rheumatic fever, and ischemic or congenital etiologies. The pathophysiology of chronic MR is described. Methods for assessing MR severity including echocardiography are provided, along with recommendations
This document provides information on mitral stenosis (MS) and mitral regurgitation (MR). It begins by describing the etiology of MS, which is primarily rheumatic fever resulting in scarring and fusion of the mitral valve. It then discusses the pathophysiology of MS, leading to right heart failure and pulmonary hypertension. Symptoms, physical exam findings, and treatments including medical management, balloon valvuloplasty, and surgical options are summarized. For MR, common causes include myxomatous disease, rheumatic fever, and ischemic or congenital etiologies. The pathophysiology of chronic MR is described. Methods for assessing MR severity including echocardiography are provided, along with recommendations
This document provides information on mitral stenosis (MS) and mitral regurgitation (MR). It begins by describing the etiology of MS, which is primarily rheumatic fever resulting in scarring and fusion of the mitral valve. It then discusses the pathophysiology of MS, leading to right heart failure and pulmonary hypertension. Symptoms, physical exam findings, and treatments including medical management, balloon valvuloplasty, and surgical options are summarized. For MR, common causes include myxomatous disease, rheumatic fever, and ischemic or congenital etiologies. The pathophysiology of chronic MR is described. Methods for assessing MR severity including echocardiography are provided, along with recommendations
Download as DOCX, PDF, TXT or read online from Scribd
Download as docx, pdf, or txt
You are on page 1/ 10
Valvular heart disease
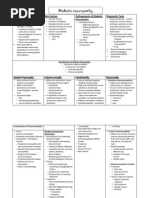
Mitral Stenosis Etiology Primarily a result of rheumatic fever (~ 99% of MVs @ surgery show rheumatic damage ) Scarring & fusion of valve apparatus Rarely congenital Pure or predominant MS occurs in approximately 40% of all patients with rheumatic heart disease Two-thirds of all patients with MS are female.
Right Right Heart Heart Failure: Failure: Hepatic Hepatic Congestion Congestion JVD JVD Tricuspid Tricuspid Regurgitation Regurgitation RA RA Enlargement Enlargement
Pulmonary Pulmonary HTN HTN Pulmonary Pulmonary Congestion Congestion LA LA Enlargement Enlargement Atrial Fib Atrial Fib LA LA Thrombi Thrombi LA Pressure LA Pressure
LV Filling LV Filling
Symptoms Fatigue Palpitations Cough SOB Left sided failure o Orthopnea o PND Palpitation Systemic embolism Pulmonary infection Hemoptysis Right sided failure o Hepatic Congestion o Edema Worsened by conditions that cardiac output. o Exertion,fever, anemia, tachycardia, , pregnancy, thyrotoxicosis
Complications Atrial dysrrhythmias Loud S1- as loud as Systemic embolization (10-25%) S2 in aortic area o Risk of embolization is related to, age, presence of atrial fibrillation, A2 to OS interval previous embolic events inversely proportional Congestive heart failure to severity Diastolic rumble: Pulmonary infarcts (result of severe CHF) length proportional Hemoptysis to severity 0 In severe MS with low o Massive: 2 to ruptured bronchial veins (pulm HTN) flow- S1, OS & rumble o Streaking/pink froth: pulmonary edema, or infection may be inaudible
Endocarditis Pulmonary infections
Physical Exam
First heart sound (S1) is accentuated
and snapping Opening snap (OS) after aortic valve closure Low pitch diastolic rumble at the apex Pre-systolic accentuation (esp. if in sinus rhythm)
EKG
LAE RVH Premature contractions Atrial flutter and/or fibrillation o freq. in pts with mod-severe MS for several years o A fib develops in 30% to 40% of pts w/symptoms
Common Murmurs Systolic Murmurs
Aortic stenosis
Mitral insufficiency
Mitral valve prolapse
Tricuspid insufficiency
Auscultation-Timing of A2 to OS Interval Diastolic Width of A2-OS inversely correlates Murmurs with severity Aortic The more severe the MS the higher insufficiency the LAP the earlirthe LV pressure Mitral stenosis falls below LAP and the MV opens
Role of Echocardiography
Diagnosis of Diagnosis and Mitral Stenosis assessment of concomitant
Assessment of valvular lesions hemodynamic Reevaluation of severity o mean gradient, patients with known MS with mitral valve changing area, pulmonary symptoms or artery pressure
Recommendations for Mitral Valve
Repair for Mitral Stenosis ACC/AHA Class I Patients with NYHA functional Class III-IV symptoms, moderate or severe MS (mitral valve area <1.5 cm 2 ),*and valve morphology favorable for repair if percutaneous mitral balloon valvotomy is not available Patients with NYHA functional Class III-IV symptoms, moderate or severe MS (mitral valve area <1.5 cm 2 ),*and valve morphology favorable for repair if a left atrial thrombus is present despite anticoagulation Patients with NYHA functional Class III-IV symptoms, moderate or severe MS (mitral valve area <1.5 cm 2 ),* and a non-pliable or calcified valve with the decision to proceed with either repair or replacement made at the time of the operation.
signs. Assessment of F/U of asymptomatic right ventricular size and function. patients with mod-severe MS Assessment of valve morphology to determine
Therapy
Medical o Diuretics for LHF/RHF percutaneous o Digitalis/Beta blockers/CCB: Rate mitral balloon control in A Fib valvuloplasty o Anticoagulation: In A Fib ACC/AHA Class IIB o Endocarditis prophylaxis Patients in NYHA functional Class I, moderate or severe MS (mitral valve area Balloon valvuloplasty o Effective long term improvement <1.5 cm 2 ),* and valve morphology favorable for repair who have had Surgical recurrent episodes of embolic events on o Mitral commissurotomy adequate anticoagulation. ACC/AHA Class III o Mitral Valve Replacement Patients with NYHA functional Class I-IV Mechanical symptoms and mild MS. Bioprosthetic
Regurgitation Measure the Impact on the LV: Apical displacement and size Palpable S3 Longer/louder MR murmer (chronic MR) S3 intensity/ length of diastolic flow rumble
Wider split S2 (earlier A2) unless HPT
narrows the split
Pulse:
brisk, low volume
Apex: hype rdynamic later ally displaced palp able S3 +/- thrill late parasternal lift 2 to LA filling S 1 soft or normal S 2 wide split (early A2) unless LBBB
Murmer-Fixed MR: pansystolic loudest apex to axilla no post extrasystolic accentuation Murmer-Dynamic MR(MVP) mid systolic +/- click upright S 3 / flow rumble if severe
Acute Severe Mitral Regurgitation
Acute severe dyspnea, CHF & hypotension LV size normal LV may/may not be hyperdynamic Loud S1 Systolic murmur may/may not be pan-systolic Inflow/rumble S3 present-may be only abnormality
Recognizing Mitral Regurgitation
ECG: LA enlargement Afib LVH (50% pts. With severe MR) RVH (15%) Combined hypertrophy (5%)
CXR: LV LA pulmonary vascularity CHF Ca++ MV/MAC
MR Stages LV size and function defined by echo Stage 1-compensated:
End-diastolic dimension less 63mm, ESD less 42mm
EF more than 60 Stage 2-transitional
EDD 65-68mm, ESD 44-45mm, EF 53-57
Stage 3-decompensated
EDD more than 70mm, ESD more than 45mm, EF less than 50
RV lift TTE/TEE for diagnosis Chordal or papilllary muscle rupture/tear Infarction with papillary muscle ischaemia or tear Infectious endocarditis with leaflet perforation or disruption or chordal tear Flail MV segment
Echocardiography
Etiology: flail leaflets (chord/pap rupture)
thick (RHD) post mvt of leaflets (MVP) vegetations(IE) Severity: regurgitant volume/fraction/orifice area LV systolic function increased LV/LA size, EF
Echo Indicators for Valve Replacement in
Asymptomatic Aortic & Mitral Regurgitation Type of Regurgi tation Aortic Mitral
LVESD mm
EF %
FS
> 55 > 45
< 55 < 60
< 0.27 < 0.32
RECOMMENDED FREQUENCY OF ECHOCARDIOGRAPHY IN PATIENTS WITH
CHRONIC MITRAL REGURGITATION AND PRIMARY MITRAL-VALVE DISEASE.
SEVERITY OF MITRAL REGURGITATION
LEFT VENTRICULAR FUNCTION*
FREQUENCY OF ECHOCARDIOGR A-PHIC FOLLOW-UP
Mild
Normal ESD and
EF
Every 5 yr
Moderate
Normal ESD and
EF
Every 1 2 yr
Moderate
ESD >40 mm or EF <0.65
Annually
Severe
Normal ESD and
EF
Annually
Severe
ESD >40 mm or EF <0.65
Every 6 mo
Ejection Fraction (LVEF)
Strongest predictor of outcome following
surgery Should be assessed quantitatively Surgery indicated if LVEF is below normal (60%) If EF normal, follow every 6 to 12 months If EF <30%, medical management (valve repair experimental in this setting)
Mitral Regurgitation ACC/AHA
recommendations Surgery Recommended in patients who are Symptomatic Asymptomatic with
Any LV dysfunction
Atrial fibrillation
Pulmonary hypertension
Reparable valves
Recurrent VT
MV Repair vs. Replacement
Lower operative mortality
Better late outcome Curative Avoids anticoagulation unless atrial fibrillation
Open Afib ablation
Mitral Valve Surgery
Only effective treatment is valve repair/replacement Optimal timing determined: Presence/absence of symptoms Functional state of ventricle Feasability of valve repair Presence of Afib/PHTN Preference/expectations of patient
Surgical Therapy Timing
Surgery reduces morbidity and
mortality from severe MR but exposes patient to risk of surgery and prosthetic valve Surgery should be performed before onset of severe symptoms or development of LV contractile dysfunction
Valve replacement: o Mortality 2-7% o Anti-coagulation o Decreased LVEF Tissue prosthetic valve degeneration Mechanical prosthetic valve dysfunction/ thrombosis
Valve repair o Mortality 2-3% o No anticoagulation (unless Afib) o Preservation of LVEF Valve repair always preferable o Feasible in 70-90% of patients
Aortic stenosis Etiology Young
patient think
congenital
Bicuspid
2% population
3:1 male:female distribution Co-existing coarctation 6% of patients
Symptoms
Asymptomatic Common in asymptomatic adults Characterized by Grade I II @ LSB Systolic ejection pattern
Rarely Unicus pid valve Subaortic stenosis o Discrete o Diffuse (Tunnel) Middle aged patient(4&5th decades) think bicuspid or rheumatic disease Old patient think degenerative (6,7,8th decades)
Normal Ao V
bicuspid
S1
Normal intensity & splitting of second sound (S2)
No other abnormal sounds or murmurs
No evidence of LVH, and no with Valsalva
normal greatric calcific valve
Physical Findings
S2
Recognizing Aortic Stenosis
Cardinal Symptoms Chest pain (angina) o Reduced coronary flow reserve o Increased demand-high afterload Syncope/Dizziness (exertional presyncope) o Fixed cardiac output o Vasodepressor response Dyspnea on exertion & rest Impaired exercise tolerance Other signs of LV failure Diastolic & systolic dysfunction
Severity of Stenosis
Normal aortic valve area 2.5-3.5
cm2 Mild stenosis 1.5-2.5 cm2 Moderate stenosis 1.0-1.5 cm2 Severe stenosis < 1.0 cm2 Onset of symptoms ~ 0.9 cm2 with CAD ~ 0.7 cm2 without CAD
Intensity DOES NOT predict severity
Presence of thrill DOES NOT predict severity Diamond shaped, harsh, systolic crescendodecrescendo Decreased, delay & prolongation of pulse amplitude Paradoxical S2 S3 (with left ventricular failure)
severe aortic stenosis Operative mortality (elderly) ~ 424%/Morbidity ~ 3-11% Event rate in asymptomatic severe AS ~ 1%/year
Etiology Valve gradient and area LVH Systolic LV function Diastolic LV function LA size Concomitant regional wall motion abnormalities Coarctation associated with bicuspid AV
Natural History Heart failure reduces life expectancy to less than 2 years Angina and syncope reduce life expectancy between 2 and 5 years Rate of progression @ 0.1 cm2/year
sign JVP-prominent A wave Carotiddelayed,anacrotc A2 audible over carotid
Correlation wi severity No Yes If A2 transmitted to carotids mean AV gradient <50mmHg Yes
Replacement in Asymptomatic AR & MR Type of Regurg itation Aortic mitral
LVESD (mm)
EF (%)
FS
> 55 > 45
< 55 < 60
< 0.27 < 0.32
as Aortic DP=LVEDP in acute AR mitral pre-closure
Physical Exam Widened pulse pressure
Systolic diastolic = pulse
pressure High pitched, blowing, decrescendo diastolic murmur at LSB Best heard at end-expiration & leaning forward Hands & Knee position
S1 S1
S2
Natural History Asymptomatic %/Y Normal LV function (~good prognosis) Progression to symptoms or LV dysfunction <6 Progression to asymptomatic LV dysfunction < 3.5 75% 5-year survival Sudden death < 0.2 Abnormal LV function Progression to cardiac symptoms 25
Symptomatic (Poor prognosis)
Mortality > 10 TX: Medical Surgery BEFORE LV dysfunction
Indication for Valve Replacement in Aortic Regurgitation
ACC/AHA Class I ACC/AHA Class II b Symptomatic patients with preserved LVF Patients with severe LV dysfunction (EF < (LVEF >50%) 25%) Asymptomatic patients with mild to Asymptomatic patients with normal systolic moderate LV dysfunction (EF 25-49%) func-tion at rest (EF >0.50) and progressi ve Patients undergoing CABG, aortic or other LV dilata-tion when the degree of dilatation valvular surgery is moderatelysevere (EDD 70 to 75 mm, ACC/AHA Class II a ESD 50 to 55 mm). ACC/AHA Class III Asymptomatic patients with preserved LVEF but severe LV dilatation (EDD>75 mm or Asymptomatic patients with normal systolicf ESD > 55mm) unction at rest (EF >0.50) and LV dilatation when the degree of dilatation is not severe (EDD <70 mm, ESD <50 mm).