Valvular Heart Disease 2
Valvular Heart Disease 2
Download as ppt, pdf, or txt
At a glance
Powered by AI
The document discusses the main types of valvular heart disease including mitral stenosis, aortic stenosis, mitral regurgitation, aortic regurgitation, tricuspid regurgitation, tricuspid stenosis, pulmonary stenosis and pulmonary regurgitation.
The main types of valvular heart disease discussed are mitral stenosis, aortic stenosis, mitral regurgitation, aortic regurgitation, tricuspid regurgitation, tricuspid stenosis, pulmonary stenosis and pulmonary regurgitation.
The main causes of mitral stenosis discussed are rheumatic fever, congenital defects such as Lutembacher syndrome, and mitral valve annular calcification in elderly patients.
You might also like
- Essential Revision Notes For MRCP PDFDocument1,002 pagesEssential Revision Notes For MRCP PDFMontasir Ahmed100% (25)
- Short Cases in Clinical Exams of Internal Medicine (PDFDrive)Document185 pagesShort Cases in Clinical Exams of Internal Medicine (PDFDrive)Nadhirah ZulkifliNo ratings yet
- PANCE Prep Pearls Valvular DiseaseDocument4 pagesPANCE Prep Pearls Valvular Diseasekat100% (2)
- Perfusion BookDocument127 pagesPerfusion Bookreader50% (2)
- Harmony in Disarray: Exploring Atrial Arrhythmias and Advancements in Cardiovascular HealthFrom EverandHarmony in Disarray: Exploring Atrial Arrhythmias and Advancements in Cardiovascular HealthNo ratings yet
- Ebstein Anomaly, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandEbstein Anomaly, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Congenital Heart Diseases, A Simple Guide to these Medical ConditionsFrom EverandCongenital Heart Diseases, A Simple Guide to these Medical ConditionsNo ratings yet
- Abnormal Slow Heart Beats, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandAbnormal Slow Heart Beats, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Assessment of bleeding Shock in a Politraumatized PatientFrom EverandAssessment of bleeding Shock in a Politraumatized PatientNo ratings yet
- A Simple Guide to the Heart beats, Related Diseases And Use in Disease DiagnosisFrom EverandA Simple Guide to the Heart beats, Related Diseases And Use in Disease DiagnosisRating: 5 out of 5 stars5/5 (1)
- Anatomy of The Mitral Valve Understanding The Mitral Valve Complex in Mitral RegurgitationDocument7 pagesAnatomy of The Mitral Valve Understanding The Mitral Valve Complex in Mitral RegurgitationecocardioNo ratings yet
- Aortic RegurgitationDocument14 pagesAortic RegurgitationFahd HatemNo ratings yet
- DR Sandeep - EISENMENGER SYNDROMEDocument81 pagesDR Sandeep - EISENMENGER SYNDROMEAlexandrescuNo ratings yet
- Constrictive PericarditisDocument54 pagesConstrictive PericarditisRazib AlamNo ratings yet
- Mitral RegurgitationDocument6 pagesMitral RegurgitationMelfi Triani SiskaNo ratings yet
- Cardiac MurmursDocument28 pagesCardiac MurmursAlvin BlackwellNo ratings yet
- Aortic Valve DiseaseDocument63 pagesAortic Valve DiseaseFaridOrahaNo ratings yet
- CardiomyopathiesDocument4 pagesCardiomyopathiesyvasparksNo ratings yet
- Approach To Cardiac MurmursDocument11 pagesApproach To Cardiac Murmurstouthang0074085No ratings yet
- Brugada SyndromeDocument1 pageBrugada SyndromecyelzNo ratings yet
- L-R ShuntDocument88 pagesL-R ShuntnanohaniwiekoNo ratings yet
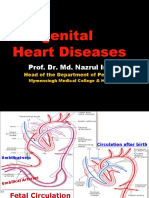
- Congenital Heart Diseases: Prof. Dr. Md. Nazrul IslamDocument23 pagesCongenital Heart Diseases: Prof. Dr. Md. Nazrul IslamprajwalNo ratings yet
- Stenosis MitralDocument11 pagesStenosis MitralRandy PangestuNo ratings yet
- FinalDocument56 pagesFinalvamshidhNo ratings yet
- Peripheral Arteries DiseasesDocument50 pagesPeripheral Arteries DiseasesAzzaiz AlexandrescuNo ratings yet
- Acute Coronary SyndromeDocument9 pagesAcute Coronary SyndromeAnthony Philip Patawaran CalimagNo ratings yet
- Mitral ValveDocument48 pagesMitral Valvestoicea_katalinNo ratings yet
- Focal Atrial Tachycardia I: Clinical Features, DiagnosisDocument10 pagesFocal Atrial Tachycardia I: Clinical Features, Diagnosisapi-26166949No ratings yet
- Valvular Heart DiseaseDocument54 pagesValvular Heart DiseaseKiki RizkyNo ratings yet
- Heart ExaminationDocument75 pagesHeart ExaminationRancesh FamoNo ratings yet
- Aortic Regurgitation CaseDocument38 pagesAortic Regurgitation CaseIka MagfirahNo ratings yet
- Infective EndocarditisDocument68 pagesInfective EndocarditisDr. Rajesh PadhiNo ratings yet
- Mitral ValveDocument48 pagesMitral Valvesinghal296% (23)
- CardiomyopathyDocument8 pagesCardiomyopathyKarisaNo ratings yet
- Ali A Sovari, MD: Author:, Staff Physician, Department of Internal MedicineDocument9 pagesAli A Sovari, MD: Author:, Staff Physician, Department of Internal MedicineMaríaDelPilarAguilarNo ratings yet
- Ngaji Arrythmia Cordis 3Document122 pagesNgaji Arrythmia Cordis 3Dhita Dwi NandaNo ratings yet
- Valvular Heart DiseaseDocument32 pagesValvular Heart DiseasefallenczarNo ratings yet
- Aortic RegurgitationDocument41 pagesAortic RegurgitationMedi PutraNo ratings yet
- 4.3.aortic StenosisDocument61 pages4.3.aortic StenosisMuh BluNo ratings yet
- 1.congenital Heart DiseaseDocument60 pages1.congenital Heart Diseasemerzi farooq ahmadkhanNo ratings yet
- Aortic StenosisDocument3 pagesAortic StenosisMaxine BaraquiaNo ratings yet
- Valvular Heart Disease: Aortic StenosisDocument28 pagesValvular Heart Disease: Aortic StenosisRajiv_Saikia_3577100% (1)
- Cardiac ArrythmiasDocument63 pagesCardiac ArrythmiasSankara SubramanianNo ratings yet
- Cardio-Vascular Disease: Mitral Stenosis & Mitral RegurgitationDocument25 pagesCardio-Vascular Disease: Mitral Stenosis & Mitral Regurgitationyulia silviNo ratings yet
- Sinus Node DysfunctionDocument11 pagesSinus Node DysfunctionVasishta Nadella100% (1)
- Valvular Heart DiseaseDocument10 pagesValvular Heart DiseaseEzyan SyaminNo ratings yet
- Overview On Peripheral Artery Disease - FinalDocument78 pagesOverview On Peripheral Artery Disease - FinalMITHA100% (1)
- Dorv Medscape 12345600Document9 pagesDorv Medscape 12345600ayubahriNo ratings yet
- Pulmonary Arterial Pressure TestingDocument22 pagesPulmonary Arterial Pressure Testingeven24No ratings yet
- Valvular Heart DiseaseDocument32 pagesValvular Heart DiseaseyunielsyaNo ratings yet
- Acute Coronary SyndromeDocument18 pagesAcute Coronary SyndromeKartika RahmawatiNo ratings yet
- Primary and Secondary CV Prevention - Iman EvanDocument104 pagesPrimary and Secondary CV Prevention - Iman EvanFikriYTNo ratings yet
- Heart Failure With Preserved Ejection FractionDocument19 pagesHeart Failure With Preserved Ejection Fractioncosmin balanNo ratings yet
- Cardio My OpathiesDocument61 pagesCardio My OpathiesIrina Cabac-PogoreviciNo ratings yet
- 25 Cardiovascular DiseaseDocument35 pages25 Cardiovascular DiseaseBramantyo NugrosNo ratings yet
- TelemetryDocument3 pagesTelemetryKelly PrattNo ratings yet
- ECG Workout Flashcards: Atrial ArrhythmiasDocument27 pagesECG Workout Flashcards: Atrial ArrhythmiasDima HabanjarNo ratings yet
- Performing A Comprehensive Epicardial Echo ExamDocument11 pagesPerforming A Comprehensive Epicardial Echo ExamPitoAdhiNo ratings yet
- Algoritma Trombosis Katup JantungDocument12 pagesAlgoritma Trombosis Katup JantungEfrison SitumorangNo ratings yet
- Mitral ValveDocument48 pagesMitral Valvestoicea_katalinNo ratings yet
- MURMURS - NotespaediaDocument8 pagesMURMURS - NotespaediaZenithNo ratings yet
- CardioDocument122 pagesCardioAdrian Rosell Carrillo EnriquezNo ratings yet
- Heart Dissection: Year 12 AS BiologyDocument9 pagesHeart Dissection: Year 12 AS BiologyBio SciencesNo ratings yet
- Acute Rheumatic FeverDocument51 pagesAcute Rheumatic FeverFaedil Ichsan CiremaiNo ratings yet
- Presentation On EchocardiogramDocument17 pagesPresentation On EchocardiogramSoniya Nakka100% (1)
- Valvular Heart DiseaseDocument73 pagesValvular Heart Diseaseindia2puppy100% (5)
- MCQ Internal Medicine PDFDocument448 pagesMCQ Internal Medicine PDFAyaa Yousef100% (5)
- Skripta-Engleski IVDocument54 pagesSkripta-Engleski IVEnvera Sivac100% (1)
- Rheumatic Heart Disease Criteria PDFDocument13 pagesRheumatic Heart Disease Criteria PDFLeo Ii S. RomagosNo ratings yet
- Ayurveda Q&A - Detoxification Therapy Cures Fungal Infection - Sify HealthDocument12 pagesAyurveda Q&A - Detoxification Therapy Cures Fungal Infection - Sify Healthsanti_1976No ratings yet
- Chapter 20 Practice TestDocument19 pagesChapter 20 Practice TestCorei'Ana Conrad0% (1)
- Double-Outlet Right Ventricle: J F. K D C. FDocument7 pagesDouble-Outlet Right Ventricle: J F. K D C. FVictor PazNo ratings yet
- PreviewDocument37 pagesPreviewDavid Teoh100% (1)
- Examining The PrecordiumDocument83 pagesExamining The PrecordiumnicolNo ratings yet
- Basinger Abraham - ConsultationDocument80 pagesBasinger Abraham - ConsultationVikas NairNo ratings yet
- Chapter 19 Heart Marie BDocument29 pagesChapter 19 Heart Marie BomarNo ratings yet
- Echocardiographic Assessment of Aortic Valve Stenosis DR RanjitDocument93 pagesEchocardiographic Assessment of Aortic Valve Stenosis DR RanjitNavojit ChowdhuryNo ratings yet
- HandBook of Pathology and PathoPhysiology of CardioVascularDocument321 pagesHandBook of Pathology and PathoPhysiology of CardioVascularNurwahidah Moh WahiNo ratings yet
- Huff - ECG Workout - Exercises in Arrhythmia InterpretationDocument415 pagesHuff - ECG Workout - Exercises in Arrhythmia InterpretationWei Jie Ong93% (15)
- Diastolic DysfunctionDocument9 pagesDiastolic DysfunctiondrsubramanianNo ratings yet
- PANCE Prep Pearls Valvular Disease PDFDocument4 pagesPANCE Prep Pearls Valvular Disease PDFkatNo ratings yet
- LFSC Gr10 p2 Memo Nov 2024 EngDocument12 pagesLFSC Gr10 p2 Memo Nov 2024 Engkgodisojan2No ratings yet
- Cardiovascular SystemDocument3 pagesCardiovascular Systemhz1588No ratings yet