
ACOG On CA Endometrium
ACOG On CA Endometrium
Uploaded by
zoviCopyright:
Available Formats
ACOG On CA Endometrium
ACOG On CA Endometrium
Uploaded by
zoviOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Copyright:
Available Formats
ACOG On CA Endometrium
ACOG On CA Endometrium
Uploaded by
zoviCopyright:
Available Formats
ACOG
PRACTICE
BULLETIN
CLINICAL MANAGEMENT GUIDELINES FOR
OBSTETRICIANGYNECOLOGISTS
NUMBER 65, AUGUST 2005
This Practice Bulletin was
developed by the ACOG Com-
Management of
mittee on Practice Bulletins
Gynecology and the Society of Endometrial Cancer
Gynecologic Oncologists mem- Endometrial carcinoma is the most common gynecologic malignancy that will
ber contributors James Orr Jr,
be encountered by almost every gynecologist. A thorough understanding of the
MD, Donald Chamberlain,
MD, Larry Kilgore, MD, and epidemiology, pathophysiology, and management strategies allows the obste-
Wendal Naumann, MD, and the triciangynecologist to identify women at increased risk, to contribute toward
editorial assistance of Joan risk reduction, and to facilitate early diagnosis of this cancer. The purpose of
Walker, MD, and Jonathan this document is to review the risks and benefits of current treatment options to
Berek, MD. The information is optimize treatment for women with endometrial cancer.
designed to aid practitioners in
making decisions about appro-
priate obstetric and gyneco-
logic care. These guidelines Background
should not be construed as dic-
tating an exclusive course of Epidemiology
treatment or procedure. Varia- Endometrial cancer is the most common female genital tract malignancy, with
tions in practice may be war- more than 40,000 cases estimated to be diagnosed in 2005 in the United States
ranted based on the needs of the (1). Most women (90%) with endometrial cancer develop symptomatic bleed-
individual patient, resources,
ing or discharge, facilitating early diagnosis and resulting in an increased
and limitations unique to the
institution or type of practice. opportunity for cure. Currently, most endometrial cancers (72%) are diagnosed
while in stage I; however, a significant number are in stage II (12%), stage III
Reaffirmed 2013 (13%), or stage IV (3%) (2). Despite this favorable stage distribution, endome-
trial cancer is responsible for 7,310 deaths each year, making it the eighth lead-
ing site of cancer-related death among American women (1).
It is estimated that 2.62% of women in the United States will develop uter-
ine cancer during their lifetime, with a 0.5% lifetime mortality risk (whites
2.8%, 0.48%; blacks 1.7%, 0.73% respectively for risk of disease and death)
(3). The 5-year survival rate for white women older than 65 years is 80.8% and
for black women in the same age group is 53.3%. It is unclear whether the high
mortality in black women is a result of delayed treatment, lack of access to care,
or a higher likelihood of cancers with more serious prognostic characteristics.
It is known that of women with endometrial cancer, only 52% of black women
older than 50 years have disease confined to the uterus at the time of original
surgery, compared with 73% of white women older than endometrium is the most aggressive form of endometrial
50 years. The overall incidence of endometrial cancer cancer, and the classification of this lesion as a sarcoma
likely will increase in the future secondary to increasing or dedifferentiated carcinoma is controversial. Using en-
obesity and the aging of the population. dometrial sampling, carcinosarcoma may be interpreted
preoperatively as adenocarcinoma, thereby making unex-
Etiology pected intraoperative findings more common.
The etiology of most endometrial cancers has been well Obtaining a family history may alert the gynecolo-
described (4). The most common cause is an excess of gist to women at increased risk for genetically linked
endogenous or exogenous estrogen unopposed by pro- cancers (eg, hereditary nonpolyposis colorectal cancer)
gestin leading to endometrial hyperplasia followed by in which young age at presentation of colon cancer is
cancer. This cause allows for prevention and early detec- important. The most common manifestation of hereditary
tion of the most common and most indolent form of nonpolyposis colorectal cancer in women is endometrial
endometrial cancer (type I or estrogen dependent). Type cancer (4060% lifetime risk), followed by colon cancer,
I endometrial cancer typically has lower grade nuclei, then ovarian cancer. It is important to identify women at
endometrioid histologic cell type, phosphatase and tensin risk in order to provide them with appropriate screening,
homologue mutation, and a good prognosis. prophylactic surgery, and counseling (5). In addition,
The more lethal variety of endometrial cancer, type II, women with anovulatory disorders should be counseled
accounts for approximately 10% of cases. It has aggressive about their long-term risk of endometrial cancer and
high-grade nuclei or serous and clear cell histology and modalities available for prevention.
P53 tumor suppression mutation. In contrast to type I, the
background underlying endometrium generally is atrophic Histologic Considerations
or associated with polyps. There is no clear epidemiologic Endometrioid adenocarcinoma is the most common his-
profile for type II cancers (Table 1). Carcinosarcoma of the tologic cell type of endometrial cancer, making up more
than three fourths of the cases. Benign or malignant squa-
mous differentiation can coexist with the adenocarcino-
Table 1. Risk Factors for Uterine Corpus Cancer ma; however, the grade and prognosis are currently deter-
Factors Influencing Risk Estimated Relative Risk mined based only on the glandular component (6, 7). The
ultimate prognosis depends on both the depth of myome-
Older age 23 trial invasion and the grade determined by glandular and
Residency in North America or nuclear cellular differentiation (8).
Northern Europe 318 The precursor lesion of the endometrioid adenocar-
Higher level of education or income 1.52 cinoma is endometrial hyperplasia, which produces a
White race 2 continuum of lesions that are difficult to differentiate by
Nulliparity 3 standard histologic characteristics. The classification of
History of infertility 23 endometrial hyperplasias by the World Health Organi-
zation is shown in the box. An additional classification
Menstrual irregularities 1.5
system is accepted by the International Society of
Late age at natural menopause 23 Gynecologic Pathologists.
Early age at menarche 1.52 Atypical endometrial hyperplasia is commonly
Long-term use of high dosages of found coexisting with undiagnosed cancer in the uterus,
menopausal estrogens 1020
Long-term use of high dosages of
combination oral contraceptives 0.30.5 World Health Organizations
High cumulative doses of tamoxifen 37 Classification of Endometrial Hyperplasia
Obesity 25 1. Simple hyperplasia
Stein-Leventhal disease or estrogen- 2. Complex hyperplasia (adenomatous)
producing tumor >5
3. Simple atypical hyperplasia
History of diabetes, hypertension, gallbladder
disease, or thyroid disease 1.33 4. Complex atypical hyperplasia (adenomatous with
Cigarette smoking 0.5 atypia)
*Relative risks depend on the study and referent group employed. Data from Scully RE, Bonfiglio TA, Kurman RJ, Silverberg SG,
Reprinted from Gynecologic cancer: controversies in management, Gershenson Wilkinson ED, editors. Histological typing of female genital tract
DM, McGuire WP, Gore M, Quinn MA, Thomas G, editors. Copyright 2004, with tumours. 2nd ed. New York (NY): Springer-Verlag; 1994.
permission from Elsevier.
2 ACOG Practice Bulletin No. 65
or if found alone, it may progress to endometrial cancer cal staging in order to adequately evaluate regional
in untreated women (9). A prospective trial was con- lymph nodes and to sample paraaortic and bilateral obtu-
ducted to identify the prevalence of underlying cancer rators and at least one other bilateral pelvic node group
and to define more clearly the diagnostic criteria for (22). These organizations recommend that findings be
atypical endometrial hyperplasia compared with cancer documented in the pathology or operative reports, or
(10). In this study, 306 women had diagnosed atypical both. The AJCC further defined the difference between
endometrial hyperplasia, established by community pathologic staging (p T, p N, p M) and clinical staging
pathologists on preoperative biopsy, followed immedi- (c T, c N, c M).
ately, without medical treatment, by hysterectomy. More Survival data generally are obtained from popula-
than 42% of women were found to have invasive cancer, tion-based registries such as those maintained by the
and some even had high-grade lesions and deep myome- American Cancer Society, the American College of
trial invasion. The results demonstrate the futility of try- Surgeons, and the Surveillance, Epidemiology and End
ing to make a true diagnosis before hysterectomy until Results (SEER) Program of the National Cancer
protein or molecular biomarkers have been established Institute. However, these data are limited by the diversity
(11, 12). of interventions used, including surgical staging. In addi-
Papillary serous histology portends an increased tion, clinical trial research organizationsPostoperative
risk of extrauterine disease and carries a poor prognosis. Radiation Therapy in Endometrial Carcinoma
Although this cell type accounts for only about 10% of (PORTEC) study group in the Netherlands and
all cases, it represents most recurrent endometrial can- Gynecologic Oncology Group in the United States
cers (13). Clear cell histology is rare but also is associat- provide data that are not population based but are quali-
ed with a poor prognosis (14). Carcinosarcoma, also ty controlled for patients treated with a standardized sur-
known as malignant mixed mllerian tumor of the gery as well as prescribed postoperative therapy.
uterus, is another histologic cell type with a poor prog-
nosis and may represent a subset of adenocarcinoma.
This lesion is high grade and spreads intraperitoneally, Clinical Considerations and
through lymphatics and by hematogenous routes.
Recommendations
Prognosis
What elements of preoperative evaluation are
The 1988 International Federation of Gynecology and
useful for women with endometrial cancer?
Obstetrics (FIGO) surgical staging system (Table 2)
incorporates important pathologic risk factors associated Patients with endometrial cancer often have comorbidi-
with prognosis and recurrent disease, including histo- ties, including obesity, hypertension, diabetes, and, fre-
logic (FIGO) grade, nuclear grade, depth of myometrial quently, cardiac and pulmonary dysfunction, making
invasion, cervical glandular or stromal invasion, vaginal them high-risk or poor surgical candidates. Careful
and adnexal metastases, positive cytology, metastatic attention to functional status and medical history will
disease in pelvic or paraaortic lymph nodes, and the assist in optimizing perioperative outcome. Perioperative
presence of intraabdominal or distant metastases risk assessment also serves as the basis for appropriate
(1517). Other prognostic factors not included in this patient counseling of the risks and benefits of available
system are DNA ploidy and the presence of lymphvas- treatment options.
cular space involvement (1820). The latter has been Only a physical examination and a chest radiograph
associated with a worsened prognosis, even in the are required for preoperative staging of the usual (type I
absence of documented lymph node metastasis (21). endometrioid grade 1) histology, clinical stage I patient.
The FIGO system emphasizes the overriding prog- All other preoperative testing should be directed toward
nostic value of surgical staging information as well as its optimizing the surgical outcome. The use of computed
use in postoperative treatment planning. The prognosis tomography or magnetic resonance imaging is not nec-
of women with endometrial cancer is dictated primarily essary because the surgeon should be prepared to resect
by the site of metastatic disease (Fig. 1). When disease metastatic disease commonly found in patients with
has been systematically documented to be confined to endometrial cancer.
the uterine fundus, the prognosis is based on grade, his- A preoperative physical examination provides infor-
tologic cell type, and depth of invasion. The degree of mation that may affect the surgical approach and subse-
lymphvascular space invasion and the patients race and quent risks, and it assists with developing a therapeutic
age are important independent prognostic factors. plan. For example, supraclavicular lymph node metasta-
Recently, the American Joint Committee on Cancer sis may make chemotherapy an appropriate first line of
(AJCC) joined FIGO in recommending the use of surgi- treatment. If the cervix appears to be enlarged (suggest-
ACOG Practice Bulletin No. 65 3
Table 2. International Federation of Gynecology and Obstetrics and TumorNodeMetastases Surgical Staging Systems for
Endometrial Cancer
TNM Categories FIGO Stages* SurgicalPathologic Findings
Primary Tumor (T)
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
Tis 0 Carcinoma in situ
T1 I Tumor confined to corpus uteri
T1a IA Tumor limited to endometrium
T1b IB Tumor invades less than one half of the myometrium
T1c IC Tumor invades one half or more of the myometrium
T2 II Tumor invades cervix but does not extend beyond uterus
T2a IIA Tumor limited to the glandular epithelium of the endocervix;
there is no evidence of connective tissue stromal invasion
T2b IIB Invasion of the stromal connective tissue of the cervix
T3 III Local and/or regional spread
T3a IIIA Tumor involves serosa and/or adnexa (direct extension or
metastasis) and/or cancer cells in ascites or peritoneal washings
T3b IIIB Vaginal involvement (direct extension or metastasis)
T4 IVA Tumor invades bladder mucosa and/or bowel mucosa (bullous
edema is not sufficient to classify a tumor as T4)
Regional Lymph Nodes (N)
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 IIIC Regional lymph node metastasis to pelvic and/or paraaortic
nodes
Distant Metastasis (M)
MX Distant metastasis cannot be assessed
M0 No distant metastasis
M1 IVB Distant metastasis (includes metastasis to abdominal lymph
nodes other than paraaortic, and/or inguinal lymph nodes;
excludes metastasis to vagina, pelvic serosa, or adnexa)
FIGO indicates International Federation of Gynecology and Obstetrics; TNM, tumornodemetastases.
*All cases of FIGO Stage IIVA should be subclassified by histologic grade as follows: GX, grade cannot be assessed; G1, well differentiated; G2, moderately differenti-
ated; G3, poorly differentiated or undifferentiated.
Used with the permission of the American Joint Committee on Cancer (AJCC), Chicago, Illinois. The original source for this material is the AJCC Cancer Staging Manual,
Sixth edition (2002), published by Springer-Verlag New York, www.springeronline.com.
ing possible tumor involvement), the differential diagno- What constitutes appropriate staging for
sis of cervical adenocarcinoma should be considered. If women with endometrial cancer?
cervical involvement is confirmed, treatment options
may include radical hysterectomy or preoperative radia- Most women with endometrial cancer benefit from
tion therapy. The finding of vaginal, parametrial, or systematic surgical staging, including pelvic washings,
adnexal extension of disease also can complicate treat- bilateral pelvic and paraaortic lymphadenectomy, and
ment planning, and special skills may be required for complete resection of all disease. Appropriate surgical
complete surgical resection. staging is prognostic and facilitates targeted therapy to
Preoperative measurement of the CA 125 level may maximize survival and to minimize the effects of under-
be appropriate because it is frequently elevated in women treatment (eg, recurrent disease or increased mortality)
with advanced-stage disease. Elevated levels of CA 125 and potential morbidity (eg, radiation injury) associated
may assist in predicting treatment response or in post- with overtreatment. Exceptions to the need for surgical
treatment surveillance (23, 24). staging include young or perimenopausal women with
4 ACOG Practice Bulletin No. 65
100
I Surgical (n = 5,017)
80
Proportion surviving II Surgical (n = 790)
60
III Surgical (n = 850)
I Clinical (n = 239)
II Clinical (n = 67)
40
III Clinical (n = 64)
20
IV Surgical (n = 207)
IV Clinical (n = 46)
0
0 1 2 3 4 5
Years after diagnosis
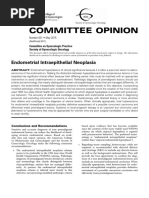
Figure 1. Carcinoma of the corpus uteri, patients treated 19961998. Survival by mode of staging, N =
7,280. (Reprinted from Int J Gynaecol Obstet, Vol. 83 (Suppl 1), Creasman WT, Odicino F, Maisonneuve P,
Beller U, Benedet JL, Heintz AP, et al. Carcinoma of the corpus uteri. p. 79118. Copyright 2003, with per-
mission from the International Federation of Gynecology and Obstetrics.)
grade 1 endometrioid adenocarcinoma associated with In specific situations, hysterectomy, bilateral sal-
atypical endometrial hyperplasia and women at increased pingo-oophorectomy, and bilateral pelvic and paraaortic
risk of mortality secondary to comorbidities. lymphadenectomy can be completed successfully and
Retroperitoneal lymph node assessment is a critical safely with less perioperative morbidity by using a
component of surgical staging and is associated with laparoscopic approach (3335).
improved survival. Women testing negative for disease of
the pelvic and paraaortic lymph nodes and for abnormal
How are women with endometrial cancer
pelvic cytology have better survival rates than women treated postoperatively?
with matched uterine histologic factors and positive
results of testing of nodes or cytology (25). These nega- The use of adjuvant radiation therapy in women with dis-
tive results allow the adjuvant radiotherapy to be with- ease limited to the uterus based on systematic surgical
held and change the survival estimates from that of a staging is controversial. Many practitioners have aban-
clinical stage I patient to a surgical stage I. Palpation of doned teletherapy (whole pelvic radiation therapy) and
the retroperitoneum is an inaccurate measure and cannot replaced it with vaginal brachytherapy for selected
substitute for surgical dissection of nodal tissue for patients (36). One study reported a 5-year survival rate of
histopathology. Sampling of pelvic lymph nodes alone 92% for systematically staged IC patients treated with
ignores the fact that 62% of women with any positive postoperative whole pelvic radiation, compared with
lymph nodes have paraaortic metastasis, and 17% have 90% for those treated with surgery alone (37). The
paraaortic disease alone (16, 2629). authors concluded that radiation should be tailored
The incidence and severity of complications associ- to sites of known metastatic disease or reserved for
ated with extensive surgical staging of women with recurrence.
endometrial cancer frequently are related to the effects of The large, randomized controlled PORTEC trial was
existing medical comorbidities (ie, obesity, diabetes, conducted to determine the value of postoperative whole
coronary artery disease) (30, 31). The average hospital pelvic radiation therapy in women after hysterectomy
stay for abdominal staging is similar to that for benign and bilateral salpingo-oophorectomy without compre-
hysterectomy (32). hensive surgical staging and lymphadenectomy. The
ACOG Practice Bulletin No. 65 5
initial report included women with grade 1 deep myome- cost reduction by avoiding routine brachytherapy and
trial invasion, grade 2 invasion of any depth, and grade 3 treating the high-risk women only when they develop
superficial invasion, and found a 5-year overall survival recurrent disease.
rate of 81% in the radiotherapy group and 85% for the
controls (38). These results confirm the conclusions of What are the recommendations for women
another large randomized prospective study of 540 found to have endometrial cancer after a
patients that there is no benefit to whole pelvic radiation hysterectomy?
therapy, except local control in the vagina and pelvis
(39). Deaths generally result from disease recurrence out- To counsel the patient appropriately on her risk of metas-
side the radiation field. Of patients treated with radiation, tases, recurrence, and death, a multidisciplinary review of
2% have major complications, and 20% have minor com- pathologic material is important (2, 15). In this clinical
plaints that affected quality of life. situation, therapeutic options include no further therapy
The second PORTEC report focused on women with and surveillance only, reoperation to complete the surgi-
grade 3 histology with deep myometrial invasion, all cal staging, or radiotherapy to prevent local recurrence.
women receiving whole pelvic radiotherapy (40). The The acceptable level of risk that determines the need for
5-year survival rate for this group of women without reoperation or radiation varies among individuals. The
comprehensive surgical staging was 58%. In contrast, survival advantages of surgical staging must be weighed
when stage IIIC patients are appropriately staged, against the complications from a new major surgical pro-
metastatic disease in the lymph nodes is removed, and cedure. This risk of additional surgery contrasts with the
treatment is delivered to the known sites of metastatic minimal difference in risk with planned, combined pro-
spread, the overall 5-year survival rate is 7085%, cedures of surgical staging with hysterectomy, bilateral
demonstrating that radiation cannot overcome poor sur- pelvic and paraaortic lymphadenectomy, and peritoneal
gical treatment (29, 41, 42). cytology tests. The advent of laparoscopic surgical
Women who do not receive postoperative radiation restaging has resulted in less morbidity using this
with surgical stage I endometrial cancer may have isolat- approach. One study on the use of laparoscopic restaging
ed recurrent disease in the vagina. Treatment of these for endometrial cancer reported a hospital stay of 1.5
recurrences demonstrated 6075% survival (38). Another days and less than 100 mL estimated blood loss (44).
randomized trial also indicates that radiation does not Treatment decisions with endometrial cancer following
improve survival or reduce distant metastases; it prevents hysterectomy are best made in consultation with a spe-
only vaginal recurrences. These recurrences can be treat- cialist with advanced training and demonstrated compe-
ed subsequently, avoiding the unnecessary exposure of tence, such as a gynecologic oncologist.
radiation toxicity (39). Therefore, for patients with surgi-
cal stage I disease, postoperative radiation therapy can What is the mode of therapy for patients with
reduce the risk of local recurrence. In deciding whether positive pelvic or paraaortic nodes?
to use radiation, the cost and toxicity should be balanced
with the evidence that the therapy does not improve sur- Every patient found to have extrauterine disease (stage
vival or reduce distant metastasis. III, IV) is at significant risk for developing persistent or
Evidence for the treatment of metastatic endometrial recurrent disease and should be considered a candidate
cancer has advanced significantly in the past decade. for additional therapy (45). Factors influencing postoper-
Recognition in multiple reports that most deaths are from ative treatment decisions may include tumor histology,
distant failure secondary to hematogenous spread makes extent of disease, the presence of medical comorbidities,
optimizing chemotherapy, possibly in combination with and the availability of research protocols. Regional or
local brachytherapy, the foundation for future research. systemic therapeutic modalities may be considered.
A cost analysis of treatment options of intermediate- Despite the potential therapeutic role of lym-
risk patients (surgical stage I, grade 23, deep myome- phadenectomy, most women with nodal metastases
trial invasion) who underwent complete staging made the should receive adjuvant therapy. The addition of thera-
following assumptions: 1) lymph node status is the most peutic pelvic radiation for the treatment of women with
important prognostic factor, 2) removal of lymph nodes stage IIIC disease (and testing negative for disease of the
testing negative for disease improves survival, 3) lym- paraaortic nodes) results in disease-free survival rates
phadenectomy has minimal morbidity, 4) lymphadenec- from 57% to 72% (42, 46).
tomy improves the cost effectiveness, and 5) teletherapy Women with paraaortic nodal disease should have
can be eliminated for stage III disease (36). The analy- the tumor completely resected and should have postoper-
sis demonstrated a 12% cost reduction with routine lym- ative imaging studies (eg, chest computed tomography or
phadenectomy by avoiding teletherapy and substituting positron emission tomography scans) to detect or exclude
brachytherapy (43). The same analysts also report a 31% the presence of occult extraabdominal disease (41, 47).
6 ACOG Practice Bulletin No. 65
The addition of paraaortic radiation is associated with versus 79%) and 10 years (94% versus 74%) (61, 62). It
improved survival (median survival, 2743 months) and would appear that grade is more predictive of survival
is of significant benefit, particularly for those with than depth of cervical invasion (63). Optimal treatment
microscopic nodal metastases (4851). of women with stage II disease has resulted in survival
Patterns of failure in women with stage IIIC disease rates approaching or exceeding 80% (6466).
suggest the possible benefit of concomitant or sequential
systemic therapy. Retrospective studies of concomitant Is there a role for radiotherapy as an
chemotherapy also support the benefit of systemic alternative to surgery?
chemotherapy (29, 47, 50). The primary treatment of endometrial cancer typically
involves hysterectomy. In the unusual instance (<3.5%)
What is the mode of therapy for patients with when a patient is deemed an exceptionally poor surgical
intraperitoneal disease? candidate, primary therapeutic radiation may be consid-
The primary mode of therapy for women with intraperi- ered for treating the uterine disease (67). Although pri-
mary therapeutic radiation is suboptimal, the use of
toneal disease includes an attempt at optimal tumor
brachytherapy to control disease offers reasonable
cytoreduction and the addition of systemic chemother-
results in this ultra-high-risk surgical population (68).
apy or radiation therapy or both (52). Optimal cytore-
The additional benefit of teletherapy remains unclear.
duction can be completed with limited morbidity and
Radiation therapy alone does not allow for directed
likely offers a survival benefit (5356). The ability to
therapy and fails to eradicate the uterine cancer in
resect isolated metastases when combined with addi-
1015% of cases. The cancer-specific 5-year survival
tional therapy can result in long-term survival similar to
rates in stage I inoperable patients (80%) are less than
the treatment of women with ovarian cancer (31).
that of stage I operable patients (98%) (67) and are relat-
Postoperatively, progestational agents or systemic
ed to tumor grade (69). Others have reported lower sur-
cytotoxic therapy may be used alone or in combination
vival rates of approximately 50% (69, 70). A significant
with directed radiation. A randomized trial showed the
number of these patients die of intercurrent disease (71).
superiority of the combination of doxorubicin, cisplatin,
These results suggest that a careful preoperative evalua-
and paclitaxel systemic chemotherapy for advanced and
tion and appropriate consultation be undertaken before
recurrent endometrial cancer (57). The use of carboplatin denying any woman the benefits of hysterectomy.
and paclitaxel in combination, similar to use for ovarian
cancer, is favored by some because of the combinations
Is there a role for progestin therapy in the
more favorable toxicity profile. treatment of atypical endometrial hyperplasia
and endometrial cancer?
What is the mode of therapy for patients with
cervical involvement? Atypical endometrial hyperplasia and endometrial can-
cer should be considered part of a continuum. The diag-
In the absence of macroscopic cervical involvement, the nosis remains uncertain as long as the uterus is in situ.
preoperative diagnosis of stage II disease is difficult to For women who do not desire fertility, hysterectomy
establish. Endocervical curettage is notoriously impre- should be recommended for treatment of atypical
cise for such use, with a reported accuracy of 50% (58). endometrial hyperplasia because of the high risk of an
It is challenging to differentiate primary cervical adeno- underlying cancer. Women who desire to maintain
carcinoma from stage II endometrial cancer. Patients fertility, whether they have a diagnosis of atypical
may benefit from HPV testing and immunohistochem- endometrial hyperplasia or grade 1 endometrioid adeno-
istry or cone biopsy for further evaluation. The treatment carcinoma, may be treated with progestins in an attempt
plan for each diagnosis is markedly different. When the to reverse the lesion.
diagnosis is unclear, radical hysterectomy and lym- Progestational agents have been evaluated as a pri-
phadenectomy can be performed, followed by tailored mary treatment modality of early grade 1 disease in
adjuvant therapy based on the pathologic findings. women who wish to maintain their fertility or in those
Treatment of women with cervical involvement may who are extremely poor operative candidates. Oral, par-
include preoperative radiation combined with total hys- enteral, or intrauterine device delivery of progestin (72)
terectomy, or radical hysterectomy with lymphadenecto- has been successful, with response rates ranging from
my followed by the addition of adjuvant chemotherapy 58% to 100% (7375). Although long-term outcomes are
or radiation therapy directed toward known sites of dis- uncertain, the disease will likely recur in most patients.
ease (59, 60). The use of radical hysterectomy has been There is controversy about whether progestin should be
associated with improved local control and survival prescribed continuously or cyclically, and these regi-
when compared with total hysterectomy at 5 years (94% mens are currently under investigation. Other hormonal
ACOG Practice Bulletin No. 65 7
therapies have been reported to be effective but are less remove intact, b) adhesions or obesity impair visualiza-
well studied (76). tion, and c) metastatic disease is encountered, to facilitate
Continued histologic monitoring is vital both to optimal surgical resection. Vaginal hysterectomy usually
assure medication response and to exclude recurrence, can be accomplished in even nulliparous obese patients
which may approach 50% (73). Following therapy, by experienced surgeons (80).
patients should undergo serial complete intrauterine
evaluation approximately every 3 months to document What is the appropriate follow-up for women
response. Progestin therapy may successfully reverse after treatment of endometrial cancer?
atypical endometrial hyperplasia as well as an early
endometrial carcinoma; conception may then be attempt- The pattern of recurrent disease depends on the original
ed (76). A review of the literature found a 76% response sites of metastasis in patients with advanced stage dis-
rate for progestin therapy in 81 patients with a median ease, as well as the treatment received. In women in
age of 30.5 years (77). The median response time was 12 whom the disease is confined to the uterus, the types of
weeks, with a median treatment duration of 24 weeks. Of recurrence depend on histologic cell type, lymphvascu-
the 62 responders, 47 did not experience recurrence. lar invasion, depth of invasion, and the use of radiation
Twenty patients became pregnant, and 12 required therapy. Investigators reported on 379 patients in whom
assisted reproductive technologies for conception. recurrence sites were local in 50%, distant in 29%, and
combined in 21% (81). The median time to detection of
What is the mode of treatment for patients recurrence was 14 months for vaginal disease and 19
with endometrial cancer and morbid obesity months for distant disease. Thirty-four percent of recur-
or other high-risk medical problems? rences were diagnosed in the first year of follow-up,
76% were found within 3 years, and 10% did not recur
Operative intervention should be considered for all until more than 5 years of follow-up. The recurrent dis-
women with uterine cancer; however, many of these ease was found on physical examination in 32% of cases,
women will have significant coexisting conditions that when the patients were asymptomatic. Only 37% report-
place them at higher risk of perioperative morbidity. ed vaginal bleeding. The patients who received postop-
Additionally, the staging procedure may predispose to erative radiotherapy had a decreased risk of vaginal
some specific morbidities (eg, thromboembolism). recurrence (24%). In addition, they have few thera-
Therefore, care for women with coexisting conditions peutic options to treat recurrence and, therefore, would
should be individualized, with appropriate perioperative benefit less from frequent surveillance with cervical
consultation sought. With disease-specific preoperative cytology screening and pelvic examinations for detec-
medical and intraoperative intervention undertaken, tion of recurrent disease.
most of this population can undergo an appropriate sur- The follow-up strategy in the nonirradiated patient
gical procedure. is based on the knowledge that recurrent disease in the
Specialized long instrumentation is available for pelvis, particularly in the vaginal cuff, can be treated
operative procedures in the obese patient; however, addi- successfully with radiotherapy (37, 38, 82). Vaginal or
tional considerations such as incision placement (eg, pelvic recurrence can be detected and treated success-
upper abdomen), thromboembolic prophylaxis, and fully in 6888% of women who have not received radia-
attention to recovery of postoperative pulmonary tion therapy (38, 82). Most studies cited monitored
function are important in reducing morbidity. patients every 34 months for 23 years, then twice
Panniculectomy has been advocated in women with a yearly with a speculum and rectovaginal examination at
specific body habitus (large panniculus adiposus) (78). each visit. The use of cervical cytology testing for detec-
Laparoscopy and vaginal hysterectomy may be of tion of recurrent disease is mostly anecdotal. The identi-
benefit for some patients. In a study of 125 elderly fication of asymptomatic distant recurrence is unlikely
women (average age, 75 years), laparoscopic staging was to have a survival benefit; treatment is primarily pallia-
successfully completed in 77.6% (79). The average hos- tive chemotherapy. The use of periodic chest radio-
pital stay was 3 days, which compares favorably to the graphic evaluation cannot be supported outside a
average 5.6-day hospital stay for total abdominal hys- research setting.
terectomy, bilateral salpingo-oophorectomy, and bilateral
pelvic and paraaortic lymphadenectomy. Thirteen
Which patients may benefit from referral to a
patients underwent only vaginal hysterectomy because of gynecologic oncologist?
medical conditions and were in the hospital an average of
2.1 days (79). In many cases, the ovaries are not removed Physicians with advanced training and expertise in the
to decrease the risk of requiring laparotomy. Conversion treatment of women with endometrial cancer, such as
to laparotomy is advised when a) the uterus is too large to gynecologic oncologists, understand the nuances of uter-
8 ACOG Practice Bulletin No. 65
ine cancer management, including the selection and For those women who have not received radiation
sequencing of treatment modalities likely to benefit the therapy, pelvic examinations every 34 months for
individual patient. When it is practical and feasible, pre- 23 years, then twice yearly following surgical
operative consultation with a physician with advanced treatment of endometrial cancer are recommended
training and demonstrated competence such as a gyneco- for detection and treatment of recurrent disease.
logic oncologist may be recommended. Consultation may
be particularly beneficial in the following situations: The following recommendations are based primar-
ily on consensus and expert opinion (Level C):
The ability to completely and adequately surgically
stage the patient is not readily available at the time
Women who cannot undergo systematic surgical
of her initial procedure. staging because of comorbidities may be candidates
Preoperative histology (grade 3, papillary serous, for vaginal hysterectomy.
clear cell, carcinosarcoma) suggests a high risk for
Only a physical examination and a chest radiograph
extrauterine spread. are required for preoperative staging of the usual
The final pathology test result reveals an unexpect- (type I endometrioid grade 1) histology, clinical
ed endometrial cancer following hysterectomy per- stage I patient. All other preoperative testing should
formed for other indications. be directed toward optimizing the surgical outcome.
There is evidence of cervical or extrauterine disease.
The pelvic washings are positive for malignant cells.
References
Recurrent disease is diagnosed or suspected.
1. Jemal A, Murray T, Ward E, Samuels A, Tiwari RC,
Nonoperative therapy is contemplated. Ghafoor A, et al. Cancer statistics, 2005. CA Cancer J
Clin 2005;55:1030. (Level II-3)
2. Creasman WT, Odicino F, Maisonneuve P, Beller U,
Summary of Benedet JL, Heintz AP, et al. Carcinoma of the corpus
uteri. Int J Gynaecol Obstet 2003;83(Suppl 1):79118.
Recommendations and (Level II-3)
3. Ries LA, Eisner MP, Kosary CL, Hankey BF, Miller BA,
Conclusions Clegg L, et al, editors. SEER Cancer Statistics Review,
19752001, National Cancer Institute. Bethesda (MD):
The following recommendations are based on lim- 2004. Available at: http://seer.cancer.gov/csr/1975_2001/.
ited or inconsistent scientific evidence (Level B): Retrieved November 9, 2004. (Level II-3)
4. Gershenson DM, McGuire WP, Gore M, Quinn MA,
Most women with endometrial cancer should under- Thomas G, editors. Gynecologic cancer: controversies in
go systematic surgical staging, including pelvic management. Philadephia (PA): Elsevier; 2004. (Level III)
washings, bilateral pelvic and paraaortic lympha- 5. Boyd J. Hereditary gynecology cancer syndromes. In:
denectomy, and complete resection of all disease. Gershenson DM, McGuire WP, Gore M, Quinn MA,
Exceptions to this include young or perimenopausal Thomas G, editors. Gynecologic cancer: controversies in
women with grade 1 endometrioid adenocarcinoma management. Philadephia (PA): Elsevier; 2004. p.
83345. (Level III)
associated with atypical endometrial hyperplasia
and those at increased risk of mortality secondary to 6. Alberhasky RC, Connelly PJ, Christopherson WM.
Carcinoma of the endometrium. IV. Mixed adenosqua-
comorbidities. mous carcinoma. A clinical-pathological study of 68 cases
Women with atypical endometrial hyperplasia and with long-term follow-up. Am J Clin Pathol 1982;77:
endometrial cancer who desire to maintain their fer- 65564. (Level III)
tility may be treated with progestin therapy. 7. Pekin T, Yildizhan B, Eren F, Pekin O, Yildizhan R.
Adenocarcinoma, adenoacanthoma, and mixed adeno-
Following therapy they should undergo serial com-
squamous carcinoma of the endometrium. Eur J Gynaecol
plete intrauterine evaluation approximately every 3 Oncol 2001;22:1513. (Level III)
months to document response. Hysterectomy should 8. Zaino RJ, Kurman R, Herbold D, Gliedman J, Bundy BN,
be recommended for women who do not desire Voet R, et al. The significance of squamous differentiation
future fertility. in endometrial carcinoma. Data from a Gynecologic
Oncology Group study. Cancer 1991;68:2293302.
Patients with surgical stage I disease may be coun- (Level II-2)
seled that postoperative radiation therapy can reduce
9. Kurman RJ, Kaminski PF, Norris HJ. The behavior of
the risk of local recurrence, but the cost and toxicity endometrial hyperplasia. A long-term study of untreat-
should be balanced with the evidence that it does not ed hyperplasia in 170 patients. Cancer 1985;56:40312.
improve survival or reduce distant metastasis. (Level III)
ACOG Practice Bulletin No. 65 9
10. Trimble CL. Atypical endometrial hyperplasia: a tough 24. Patsner B, Orr JW Jr, Mann WJ Jr. Use of serum CA 125
call. Int J Gynecol Cancer 2005;15:401. measurement in posttreatment surveillance of early-stage
11. Mutter GL, Lin MC, Fitzgerald JT, Kum JB, Baak JP, endometrial carcinoma. Am J Obstet Gynecol 1990;162:
Lees JA, et al. Altered PTEN expression as a diagnostic 4279. (Level II-2)
marker for the earliest endometrial precancers. J Natl 25. Kilgore LC, Partridge EE, Alvarez RD, Austin JM,
Cancer Inst 2000;92:92430. (Level III) Shingleton HM, Noojin F 3rd, et al. Adenocarcinoma of
12. Maxwell GL, Risinger JI, Gumbs C, Shaw H, Bentley RC, the endometrium: survival comparisons of patients with
Barrett JC, et al. Mutation of the PTEN tumor suppressor and without pelvic node sampling. Gynecol Oncol 1995;
gene in endometrial hyperplasias. Cancer Res 1998;58: 56:2933. (Level II-3)
25003. (Level III) 26. Giradi F, Petru E, Heydarfadai M, Haas J, Winter R.
13. Hendrickson M, Ross J, Eifel P, Martinez A, Kempson R. Pelvic lymphadenectomy in the surgical treatment of
Uterine papillary serous carcinoma: a highly malignant endometrial cancer. Gynecol Oncol 1993;49:17780.
form of endometrial adenocarcinoma. Am J Surg Pathol (Level III)
1982;6:93108. (Level III) 27. Chuang L, Burke TW, Tornos C, Marino BD, Mitchell MF,
14. Christopherson WM, Alberhasky RC, Connelly PJ. Tortolero-Luna G, et al. Staging laparotomy for endome-
Carcinoma of the endometrium: I. A clinicopathologic trial carcinoma: assessment of retroperitoneal lymph
study of clear-cell carcinoma and secretory carcinoma. nodes. Gynecol Oncol 1995;58:18993. (Level II-3)
Cancer 1982;49:151123. (Level III) 28. Arango HA, Hoffman MS, Roberts WS, DeCesare SL,
15. Morrow CP, Bundy BN, Kurman RJ, Creasman WT, Fiorica JV, Drake J. Accuracy of lymph node palpation to
Heller P, Homesley HD, et al. Relationship between sur- determine need for lymphadenectomy in gynecologic
gical-pathological risk factors and outcome in clinical malignancies. Obstet Gynecol 2000;95:5536. (Level
stage I and II carcinoma of the endometrium: a II-3)
Gynecologic Oncology Group study. Gynecol Oncol 29. McMeekin DS, Lashbrook D, Gold M, Johnson G, Walker
1991;40:5565. (Level II-2) JL, Mannel R. Analysis of FIGO Stage III endometrial
16. Creasman WT, Morrow CP, Bundy BN, Homesley HD, cancer patients. Gynecol Oncol 2001;81:2738. (Level
Graham JE, Heller PB. Surgical pathologic spread pat- II-3)
terns of endometrial cancer. A Gynecologic Oncology 30. Geisler JP, Geisler HE, Melton ME, Wiemann MC. What
Group Study. Cancer 1987;60(Suppl 8):203541. (Level
staging surgery should be performed on patients with
II-2)
uterine papillary serous carcinoma? Gynecol Oncol
17. Boronow RC, Morrow CP, Creasman WT, Disaia PJ, 1999;74:4657. (Level II-3)
Silverberg SG, Miller A, et al. Surgical staging in
31. Orr JW Jr, Orr PF, Taylor PT. Surgical staging endometrial
endometrial cancer: clinical-pathologic findings of a
cancer. Clin Obstet Gynecol 1996;39:65668. (Level III)
prospective study. Obstet Gynecol 1984;63:82532.
(Level III) 32. Kennedy AW, Austin JM Jr, Look KY, Munger CB. The
18. Kodama S, Kase H, Tanaka K, Matsui K. Multivariate Society of Gynecologic Oncologists Outcomes Task
analysis of prognostic factors in patients with endometrial Force. Study of endometrial cancer: initial experiences.
cancer. Int J Gynaecol Obstet 1996;53:2330. (Level II-3) Gynecol Oncol 2000;79:37998. (Level III)
19. Baak JP, Snijders WP, Van Diest PJ, Armee-Horvath E, 33. Holub Z, Jabor A, Bartos P, Eim J, Urbanek S,
Kenemans P. Confirmation of the prognostic value of the Pivovarnikova R. Laparoscopic surgery for endometrial
ECPI-1 score (myometrial invasion, DNA-ploidy and cancer: long-term results of a multicentric study. Eur J
mean shortest nuclear axis) in FIGO stage I endometrial Gynaecol Oncol 2002;23:30510. (Level II-2)
cancer patients with long follow-up. Int J Gynecol Cancer 34. Eltabbakh GH, Shamonki MI, Moody JM, Garafano LL.
1995;5:1126. (Level II-2) Laparoscopy as the primary modality for the treatment of
20. Ambros RA, Kurman RJ. Identification of patients with women with endometrial carcinoma. Cancer 2001;91:
stage I uterine endometrioid adenocarcinoma at high risk 37887. (Level II-2)
of recurrence by DNA ploidy, myometrial invasion, and 35. Malur S, Possover M, Michels W, Schneider A.
vascular invasion. Gynecol Oncol 1992;45:2359. (Level Laparoscopic-assisted vaginal versus abdominal surgery
II-3) in patients with endometrial cancera prospective ran-
21. Gal D, Recio FO, Zamurovic D, Tancer ML. domized trial. Gynecol Oncol 2001;80:23944. (Level I)
Lymphvascular space involvementa prognostic indica- 36. Fanning J, Hoffman ML, Andrews SJ, Harrah AW,
tor in endometrial adenocarcinoma. Gynecol Oncol 1991; Feldmeier JJ. Cost-effectiveness analysis of the treatment
42:1425. (Level II-3) for intermediate risk endometrial cancer: postoperative
22. American Joint Committee on Cancer. AJCC cancer stag- brachytherapy vs. observation. Gynecol Oncol 2004;
ing manual. 6th ed. New York (NY): Springer-Verlag; 93:6326. (Level III)
2002. (Level III) 37. Straughn JM, Huh WK, Orr JW Jr, Kelly FJ, Roland PY,
23. Patsner B, Tenhoppen DJ, Mann WJ. Use of serum CA- Gold MA, et al. Stage IC adenocarcinoma of the
125 levels to monitor therapy of patients with advanced or endometrium: survival comparisons of surgically staged
recurrent endometrial carcinoma. Eur J Gynaecol Oncol patients with and without adjuvant radiation therapy.
1989;10:3225. (Level III) Gynecol Oncol 2003;89:295300. (Level II-3)
10 ACOG Practice Bulletin No. 65
38. Creutzberg CL, van Putten WL, Koper PC, Lybeert ML, 51. McMeekin DS, Tillmanns T. Endometrial cancer: treat-
Jobsen JJ, Warlam-Rodenhuis CC, et al. Surgery and post- ment of nodal metastases. Curr Treat Options Oncol
operative radiotherapy versus surgery alone for patients 2003;4:12130. (Level III)
with stage-1 endometrial carcinoma: multicentre ran-
52. Memarzadeh S, Holschneider CH, Bristow RE, Jones NL,
domised trial. PORTEC Study Group. Post Operative
Fu YS, Karlan BY, et al. FIGO stage III and IV uterine
Radiation Therapy in Endometrial Carcinoma. Lancet
papillary serous carcinoma: impact of residual disease on
2000;355:140411. (Level I)
survival. Int J Gynecol Cancer 2002;12:4548. (Level
39. Aalders J, Abeler V, Kolstad P, Onsrud M. Postoperative II-3)
external irradiation and prognostic parameters in stage I
endometrial carcinoma: clinical and histopathologic study 53. Ayhan A, Taskiran C, Celik C, Yuce K, Kucukali T. The
of 540 patients. Obstet Gynecol 1980;56:41927. (Level influence of cytoreductive surgery on survival and mor-
II-2) bidity in stage IVB endometrial cancer. Int J Gynecol
Cancer 2002;12:44853. (Level II-3)
40. Creutzberg CL, van Putten WL, Warlam-Rodenhuis CC,
van den Bergh AC, de Winter KA, Koper PC, et al. 54. Bristow RE, Zerbe MJ, Rosenshein NB, Grumbine FC,
Outcome of high-risk stage IC, grade 3, compared with Montz FJ. Stage IVB endometrial carcinoma: the role of
stage I endometrial carcinoma patients: the Postoperative cytoreductive surgery and determinants of survival.
Radiation Therapy in Endometrial Carcinoma Trial. J Clin Gynecol Oncol 2000;78:8591. (Level II-3)
Oncol 2004;22:123441. (Level II-2) 55. Chi DS, Welshinger M, Venkatraman ES, Barakat RR.
41. Mariani A, Webb MJ, Keeney GL, Aletti G, Podratz KC. The role of surgical cytoreduction in Stage IV endometri-
Predictors of lymphatic failure in endometrial cancer. al carcinoma. Gynecol Oncol 1997;67:5660. (Level II-3)
Gynecol Oncol 2002;84:43742. (Level II-3) 56. Goff BA, Goodman A, Muntz HG, Fuller AF Jr, Nikrui N,
42. Nelson G, Randall M, Sutton G, Moore D, Hurteau J, Rice LW. Surgical stage IV endometrial carcinoma: a
Look K. FIGO stage IIIC endometrial carcinoma with study of 47 cases. Gynecol Oncol 1994;52:237 40.
metastases confined to pelvic lymph nodes: analysis of (Level II-3)
treatment outcomes, prognostic variables, and failure pat-
57. Fleming GF, Brunetto VL, Cella D, Look KY, Reid GC,
terns following adjuvant radiation therapy. Gynecol Oncol
Munkarah AR, et al. Phase III trial of doxorubicin plus cis-
1999;75:2114. (Level II-3)
platin with or without paclitaxel plus filgrastim in advanced
43. Fanning J. Treatment for early endometrial cancer. Cost- endometrial carcinoma: a Gynecologic Oncology Group
effectiveness analysis. J Reprod Med 1999;44:71923. Study. J Clin Oncol 2004;22:215966. (Level I)
(Level III)
58. Leminen A, Forss M, Lehtovirta P. Endometrial adenocar-
44. Childers JM, Spirtos NM, Brainard P, Surwit EA. cinoma with clinical evidence of cervical involvement:
Laparoscopic staging of the patient with incompletely accuracy of diagnostic procedures, clinical course, and
staged early adenocarcinoma of the endometrium. Obstet prognostic factors. Acta Obstet Gynecol Scand 1995;74:
Gynecol 1994;83:597600. (Level III) 616. (Level II-3)
45. Mundt AJ, McBride R, Rotmensch J, Waggoner SE, 59. Boente MP, Orandi YA, Yordan EL, Miller A, Graham JE,
Yamada SD, Connell PP. Significant pelvic recurrence in Kirshner C, et al. Recurrence patterns and complications
high-risk pathologic stage IIV endometrial carcinoma in endometrial adenocarcinoma with cervical involve-
patients after adjuvant chemotherapy alone: implications ment. Ann Surg Oncol 1995;2:13844. (Level II-3)
for adjuvant radiation therapy. Int J Radiat Oncol Biol
Phys 2001;50:114553. (Level II-3) 60. Maggino T, Romagnolo C, Landoni F, Sartori E, Zola P,
Gadducci A. An analysis of approaches to the manage-
46. Ayhan A, Taskiran C, Celik C, Aksu T, Yuce K. Surgical ment of endometrial cancer in North America: a CTF
stage III endometrial cancer: analysis of treatment out-
study. Gynecol Oncol 1998;68:2749. (Level III)
comes, prognostic factors and failure patterns. Eur J
Gynaecol Oncol 2002;23:5536. (Level II-3) 61. Mariani A, Webb MJ, Kenney GL, Calori G, Podratz KC.
47. Bristow RE, Zahurak ML, Alexander CJ, Zellars RC, Role of wide/radical hysterectomy and pelvic lymph node
Montz FJ. FIGO stage IIIC endometrial carcinoma: resec- dissection in endometrial cancer with cervical involve-
tion of macroscopic nodal disease and other determinants of ment. Gynecol Oncol 2001;83:7280. (Level II-3)
survival. Int J Gynecol Cancer 2003;13:66472. (Level II-3) 62. Sartori E, Gadducci A, Landoni F, Lissoni A, Maggino T,
48. Rose PG, Cha SD, Tak WK, Fitzgerald T, Reale F, Hunter Zola P, et al. Clinical behavior of 203 stage II endometri-
RE. Radiation therapy for surgically proven para-arotic al cancer cases: the impact of primary surgical approach
node metastasis in endometrial carcinoma. Int J Radiat and of adjuvant radiation therapy. Int J Gynecol Cancer
Oncol Biol Phys 1992;24:22933. (Level II-3) 2001;11:4307. (Level II-3)
49. Husseinzadeh N, Shrake P, DeEulis T, Rowley K, Aron B. 63. Reisinger SA, Staros EB, Mohiuddin M. Survival and fail-
Chemotherapy and extended-field radiation therapy to ure analysis in stage II endometrial cancer using the
para-aortic area in patients with histologically proven revised 1988 FIGO staging system. Int J Radiat Oncol
metastatic cervical cancer to para-artic nodes: a phase II Biol Phys 1991;21:102732. (Level II-3)
pilot study. Gynecol Oncol 1994;52:32631. (Level I) 64. Maingon P, Horiot JC, Fraisse J, Salas S, Collin F, Bone-
50. Katz LA, Andrews SJ, Fanning J. Survival after multi- Lepinoy MC, et al. Preoperative radiotherapy in stage I/II
modality treatment for stage IIIC endometrial cancer. Am endometrial adenocarcinoma. Radiother Oncol 1996;39:
J Obstet Gynecol 2001;184:10713. (Level II-2) 2018. (Level II-3)
ACOG Practice Bulletin No. 65 11
65. Eltabbakh GH, Moore AD. Survival of women with sur- serve the uterususefulness and limitations. Eur J
gical stage II endometrial cancer. Gynecol Oncol 1999; Gynaecol Oncol 2001;22:21720. (Level III)
74:805. (Level II-3) 75. Kaku T, Yoshikawa H, Tsuda H, Sakamoto A, Fukunaga
66. Calvin DP, Connell PP, Rotmensch J, Waggoner S, Mundt M, Kuwabara Y, et al. Conservative therapy for adenocar-
AJ. Surgery and postoperative radiation therapy in stage II cinoma and atypical endometrial hyperplasia of the
endometrial carcinoma. Am J Clin Oncol 1999;22: endometrium in young women: central pathologic review
33843. (Level II-3) and treatment outcome. Cancer Lett 2001;167:3948.
67. Fishman DA, Roberts KB, Chambers JT, Kohorn EI, (Level III)
Schwartz PE, Chambers SK. Radiation therapy as exclu- 76. Wang CB, Wang CJ, Huang HJ, Hsueh S, Chou HH,
sive treatment for medically inoperable patients with stage Soong YK, et al. Fertility-preserving treatment in young
I and II endometrioid carcinoma with endometrium. patients with endometrial adenocarcinoma. Cancer 2002;
Gynecol Oncol 1996;61:18996. (Level II-2) 94:21928. (Level III)
68. Kucera H, Knocke TH, Kucera E, Potter R. Treatment of 77. Ramirez PT, Frumovitz M, Bodurka DC, Sun CC,
endometrial carcinoma with high-dose-rate brachytherapy Levenback C. Hormonal therapy for the management of
alone in medically inoperable stage I patients. Acta Obstet grade 1 endometrial adenocarcinoma: a literature review.
Gynecol Scand 1998;77:100812. (Level II-3) Gynecol Oncol 2004;95:1338. (Level III)
69. Rouanet P, Dubois JB, Gely S, Pourquier H. Exclusive 78. Tillmanns TD, Kamelle SA, Abudayyeh I, McMeekin SD,
radiation therapy in endometrial carcinoma. Int J Radiat Gold MA, Korkos TG, et al. Panniculectomy with simul-
Oncol Biol Phys 1993;26:2238. (Level II-3) taneous gynecologic oncology surgery. Gynecol Oncol
70. Knocke TH, Kucera H, Weidinger B, Holler W, Potter R. 2001;83:51822. (Level III)
Primary treatment of endometrial carcinoma with high- 79. Scribner DR Jr, Walker JL, Johnson GA, McMeekin SD,
dose rate brachytherapy: results of 12 years of experience Gold MA, Mannel RS. Surgical management of early-
with 280 patients. Int J Radiat Oncol Biol Phys 1997; stage endometrial cancer in the elderly: is laparoscopy
37:35965. (Level II-3) feasible? Gynecol Oncol 2001;83:5638. (Level II-3)
71. Kupelian PA, Eifel PJ, Tornos C, Burke TW, Delclos L, 80. Bloss JD, Berman ML, Bloss LP, Buller RE. Use of vagi-
Oswald MJ. Treatment of endometrial carcinoma with nal hysterectomy for the management of stage I endome-
radiation therapy alone. Int J Radiat Oncol Biol Phys trial cancer in the medically compromised patient.
1993;27:81724. (Level II-3) Gynecol Oncol 1991;40:747. (Level II-3)
72. Montz FJ, Bristow RE, Bovicelli A, Tomacruz R, Kurman 81. Aalders JG, Abeler V, Kolstad P. Recurrent adenocarcino-
RJ. Intrauterine progesterone treatment of early endo- ma of the endometrium: a clinical and histopathological
metrial cancer. Am J Obstet Gynecol 2002;186:6517. study of 379 patients. Gynecol Oncol 1984;17:85103.
(Level III) (Level II-2)
73. Gotlieb WH, Beiner ME, Shalmon B, Korach Y, Segal Y, 82. Keys HM, Roberts JA, Brunetto VL, Zaino RJ, Spirtos
Zmira N, et al. Outcome of fertility-sparing treatment NM, Bloss JD, et al. A phase III trial of surgery with or
with progestins in young patients with endometrial can- without adjunctive external pelvic radiation therapy in
cer. Obstet Gynecol 2003;102:71825. (Level III) intermediate risk endometrial adenocarcinoma: a
74. Imai M, Jobo T, Sato R, Kawaguchi M, Kuramoto H. Gynecologic Oncology Group study [published erratum
Medroxyprogesterone acetate therapy for patients with appears in Gynecol Oncol 2004;94:2412]. Gynecol
adenocarcinoma of the endometrium who wish to pre- Oncol 2004;92:74451. (Level I)
ACOG Practice Bulletin No. 65 12
Copyright August 2005 by the American College of Obste-
The MEDLINE database, the Cochrane Library, and tricians and Gynecologists. All rights reserved. No part of this
ACOGs own internal resources and documents were used publication may be reproduced, stored in a retrieval system, or
to conduct a literature search to locate relevant articles pub- transmitted, in any form or by any means, electronic, mechan-
lished between January 1985 and April 2005. The search ical, photocopying, recording, or otherwise, without prior writ-
was restricted to articles published in the English language. ten permission from the publisher.
Priority was given to articles reporting results of original Requests for authorization to make photocopies should be
research, although review articles and commentaries also directed to Copyright Clearance Center, 222 Rosewood Drive,
were consulted. Abstracts of research presented at sympo- Danvers, MA 01923, (978) 750-8400.
sia and scientific conferences were not considered adequate
for inclusion in this document. Guidelines published by or- ISSN 1099-3630
ganizations or institutions such as the National Institutes of The American College of
Health and the American College of Obstetricians and Gy- Obstetricians and Gynecologists
necologists were reviewed, and additional studies were 409 12th Street, SW
located by reviewing bibliographies of identified articles. PO Box 96920
When reliable research was not available, expert opinions Washington, DC 20090-6920
from obstetriciangynecologists were used. 12345/98765
Studies were reviewed and evaluated for quality according Management of endometrial cancer. ACOG Practice Bulletin No. 65.
to the method outlined by the U.S. Preventive Services Task American College of Obstetricians and Gynecologists. Obstet Gynecol
Force: 2005;106:41325.
I Evidence obtained from at least one properly de-
signed randomized controlled trial.
II-1 Evidence obtained from well-designed controlled
trials without randomization.
II-2 Evidence obtained from well-designed cohort or
casecontrol analytic studies, preferably from more
than one center or research group.
II-3 Evidence obtained from multiple time series with or
without the intervention. Dramatic results in uncon-
trolled experiments also could be regarded as this
type of evidence.
III Opinions of respected authorities, based on clinical
experience, descriptive studies, or reports of expert
committees.
Based on the highest level of evidence found in the data,
recommendations are provided and graded according to the
following categories:
Level ARecommendations are based on good and consis-
tent scientific evidence.
Level BRecommendations are based on limited or incon-
sistent scientific evidence.
Level CRecommendations are based primarily on con-
sensus and expert opinion.
13 ACOG Practice Bulletin No. 65
You might also like
- PDF Urinary Fistula René Sotelo (Editor) downloadNo ratings yetPDF Urinary Fistula René Sotelo (Editor) download60 pages
- Breast Cancer: by Eric Lee & Rikki HabernyNo ratings yetBreast Cancer: by Eric Lee & Rikki Haberny53 pages
- Melanoma: Meku Damtie (M.D.) July 18, 2006No ratings yetMelanoma: Meku Damtie (M.D.) July 18, 200638 pages
- Breast Cancer: Dr. Armando V. Tan AnatomyNo ratings yetBreast Cancer: Dr. Armando V. Tan Anatomy9 pages
- Prof - Amer Eltwati Ben Irhuma Consultant Surgeon Sebha Medical College100% (1)Prof - Amer Eltwati Ben Irhuma Consultant Surgeon Sebha Medical College79 pages
- ACG Guideline Focal Liver Lesions September 2014No ratings yetACG Guideline Focal Liver Lesions September 201420 pages
- (SURG) 5.4b Management of Soft Tissue SarcomaNo ratings yet(SURG) 5.4b Management of Soft Tissue Sarcoma6 pages
- Benign Breast Diseases Epidemiology, Evaluation,.17No ratings yetBenign Breast Diseases Epidemiology, Evaluation,.1715 pages
- Nascimento Et Al. - 2012 - Bloody Nipple Discharge in Infancy - Report of Two CasesNo ratings yetNascimento Et Al. - 2012 - Bloody Nipple Discharge in Infancy - Report of Two Cases3 pages
- Committee Opinion: Endometrial Intraepithelial NeoplasiaNo ratings yetCommittee Opinion: Endometrial Intraepithelial Neoplasia7 pages
- Endometrial Carcinoma - Pretreatment Evaluation, Staging, and Surgical Treatment - UpToDateNo ratings yetEndometrial Carcinoma - Pretreatment Evaluation, Staging, and Surgical Treatment - UpToDate24 pages
- Clinical Surgery in General RCS Course ManualNo ratings yetClinical Surgery in General RCS Course Manual2 pages
- By: Shrijan Timalsina, Samir Ghimire For-Dr - UMSD, DR - RJ Urosurgery Surgery DepartmentNo ratings yetBy: Shrijan Timalsina, Samir Ghimire For-Dr - UMSD, DR - RJ Urosurgery Surgery Department30 pages
- Aagl Practice Guidelines For The Diagnosis and Management of Submucous LeiomyomasNo ratings yetAagl Practice Guidelines For The Diagnosis and Management of Submucous Leiomyomas20 pages
- 17 Plasma Cell Neoplasms - Libre Pathology PDFNo ratings yet17 Plasma Cell Neoplasms - Libre Pathology PDF5 pages
- Breast Surgery - Assessment of A Breast LumpNo ratings yetBreast Surgery - Assessment of A Breast Lump3 pages
- Introduction To History Taking & Physical Examination in SurgeryNo ratings yetIntroduction To History Taking & Physical Examination in Surgery46 pages
- Review On Medicinal Value of Honeybee PR PDFNo ratings yetReview On Medicinal Value of Honeybee PR PDF12 pages
- Anti-Diabetes Sugar Properties of Gamma Oryzanol - ResearchNo ratings yetAnti-Diabetes Sugar Properties of Gamma Oryzanol - Research3 pages
- Hematology Part 1 - Dr. Saud Alhayli (Answers)No ratings yetHematology Part 1 - Dr. Saud Alhayli (Answers)162 pages
- Rahman Institute of Nursing and Paramedical Sciences, Radhanagar, Guwahati Demonstration ON Peritoneal DialysisNo ratings yetRahman Institute of Nursing and Paramedical Sciences, Radhanagar, Guwahati Demonstration ON Peritoneal Dialysis7 pages
- Cagri Karaciklar Fragility Fractures Presentation PDFNo ratings yetCagri Karaciklar Fragility Fractures Presentation PDF15 pages
- B.inggris Laporan Pendahuluan Hipertensi-1-DikonversiNo ratings yetB.inggris Laporan Pendahuluan Hipertensi-1-Dikonversi13 pages
- Localized Multiple Cemental Excrescences HipercementosisNo ratings yetLocalized Multiple Cemental Excrescences Hipercementosis5 pages
- Cabaran Membesarkan Anak-Anak Autisme Daripada Perspektif Ibu (The Challenges of100% (1)Cabaran Membesarkan Anak-Anak Autisme Daripada Perspektif Ibu (The Challenges of14 pages
- Annex E - COVID 19 Monitoring Tools - v3 Final - 09 23 21No ratings yetAnnex E - COVID 19 Monitoring Tools - v3 Final - 09 23 2116 pages
- MODULE 3 Disorders of Primary HemostasisNo ratings yetMODULE 3 Disorders of Primary Hemostasis13 pages

























































































- Ewing Sarcoma: Causes, Tests, and Treatment OptionsFrom EverandEwing Sarcoma: Causes, Tests, and Treatment Options
- Prof - Amer Eltwati Ben Irhuma Consultant Surgeon Sebha Medical CollegeProf - Amer Eltwati Ben Irhuma Consultant Surgeon Sebha Medical College
- Benign Breast Diseases Epidemiology, Evaluation,.17Benign Breast Diseases Epidemiology, Evaluation,.17
- Nascimento Et Al. - 2012 - Bloody Nipple Discharge in Infancy - Report of Two CasesNascimento Et Al. - 2012 - Bloody Nipple Discharge in Infancy - Report of Two Cases
- Committee Opinion: Endometrial Intraepithelial NeoplasiaCommittee Opinion: Endometrial Intraepithelial Neoplasia
- Endometrial Carcinoma - Pretreatment Evaluation, Staging, and Surgical Treatment - UpToDateEndometrial Carcinoma - Pretreatment Evaluation, Staging, and Surgical Treatment - UpToDate
- By: Shrijan Timalsina, Samir Ghimire For-Dr - UMSD, DR - RJ Urosurgery Surgery DepartmentBy: Shrijan Timalsina, Samir Ghimire For-Dr - UMSD, DR - RJ Urosurgery Surgery Department
- Aagl Practice Guidelines For The Diagnosis and Management of Submucous LeiomyomasAagl Practice Guidelines For The Diagnosis and Management of Submucous Leiomyomas
- Introduction To History Taking & Physical Examination in SurgeryIntroduction To History Taking & Physical Examination in Surgery
- Anti-Diabetes Sugar Properties of Gamma Oryzanol - ResearchAnti-Diabetes Sugar Properties of Gamma Oryzanol - Research
- Rahman Institute of Nursing and Paramedical Sciences, Radhanagar, Guwahati Demonstration ON Peritoneal DialysisRahman Institute of Nursing and Paramedical Sciences, Radhanagar, Guwahati Demonstration ON Peritoneal Dialysis
- Cagri Karaciklar Fragility Fractures Presentation PDFCagri Karaciklar Fragility Fractures Presentation PDF
- B.inggris Laporan Pendahuluan Hipertensi-1-DikonversiB.inggris Laporan Pendahuluan Hipertensi-1-Dikonversi
- Localized Multiple Cemental Excrescences HipercementosisLocalized Multiple Cemental Excrescences Hipercementosis
- Cabaran Membesarkan Anak-Anak Autisme Daripada Perspektif Ibu (The Challenges ofCabaran Membesarkan Anak-Anak Autisme Daripada Perspektif Ibu (The Challenges of
- Annex E - COVID 19 Monitoring Tools - v3 Final - 09 23 21Annex E - COVID 19 Monitoring Tools - v3 Final - 09 23 21