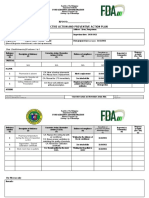
Toll Manufacturing Fda Requirements: Checklists and Forms
Toll Manufacturing Fda Requirements: Checklists and Forms
Download as docx, pdf, or txt
You might also like
- Sample Motion To Quash Service For California Unlawful Detainer (Eviction)Document4 pagesSample Motion To Quash Service For California Unlawful Detainer (Eviction)Stan Burman85% (13)
- Performer AgreementDocument3 pagesPerformer AgreementGeanina PanaitNo ratings yet
- CPR List - FDA PhilippinesDocument2 pagesCPR List - FDA PhilippinesMiguel Pillas100% (6)
- Ascentia ProposalDocument5 pagesAscentia ProposalVeegee CabugaoNo ratings yet
- Job Description PharmacistDocument4 pagesJob Description PharmacistAbdiNo ratings yet
- BIR ICC and BCCDocument1 pageBIR ICC and BCCDarlyn EtangNo ratings yet
- Denr CNC Ulingan PDFDocument1 pageDenr CNC Ulingan PDFReyjel PanaliganNo ratings yet
- RDO No. 43A - East Pasig Zonal ValuesDocument161 pagesRDO No. 43A - East Pasig Zonal ValuesMiguel Pillas79% (14)
- Director's Certificate TEMPLATEDocument1 pageDirector's Certificate TEMPLATEMiguel PillasNo ratings yet
- CPR List - FDA PhilippinesDocument2 pagesCPR List - FDA PhilippinesMiguel Pillas100% (6)
- APUSH Exam 1996Document15 pagesAPUSH Exam 1996gophillies4000No ratings yet
- Integrated ApplicationForm (BLANK)Document42 pagesIntegrated ApplicationForm (BLANK)Reggie Theresa MarquezNo ratings yet
- The FDA PhilippinesDocument5 pagesThe FDA PhilippinesJose Mari Angelo DionioNo ratings yet
- FDA Philippines Letter of UndertakingDocument2 pagesFDA Philippines Letter of UndertakingOmar AsodisenNo ratings yet
- Declaration of Assumption of LiabilityDocument1 pageDeclaration of Assumption of LiabilityJsyazonNo ratings yet
- 2017treasurers AffidavitDocument1 page2017treasurers AffidavitIMEENo ratings yet
- Labor Cases FinalsDocument53 pagesLabor Cases FinalsDenise Michaela YapNo ratings yet
- Employee Benefits Survey TemplateDocument3 pagesEmployee Benefits Survey TemplateepicnexinfraNo ratings yet
- ManifestationDocument1 pageManifestationYoko GNo ratings yet
- Sop-2022 1st RevisionDocument35 pagesSop-2022 1st RevisionMariper SantosNo ratings yet
- Sample Form of Notice To Change Nominee/ Alternate Nominee of The One Person CorporationDocument2 pagesSample Form of Notice To Change Nominee/ Alternate Nominee of The One Person CorporationCarl SoriaNo ratings yet
- Revised Establishment Report Form v3 1Document5 pagesRevised Establishment Report Form v3 1Sai GuyoNo ratings yet
- UNO Presentation FinalDocument35 pagesUNO Presentation FinalcyddjayNo ratings yet
- INTEGRATED APPLICATION FORM - BIO PROCARE With DataDocument4 pagesINTEGRATED APPLICATION FORM - BIO PROCARE With Datakim roqueNo ratings yet
- Employee Evaluation FormDocument1 pageEmployee Evaluation Formfelius21811No ratings yet
- Release WaiverDocument2 pagesRelease WaiverElli Jane ValdezNo ratings yet
- Consent, Assumption of Risk, and Waiver of LiabilityDocument1 pageConsent, Assumption of Risk, and Waiver of LiabilityDonnabell DayudayNo ratings yet
- O10053-2006 (Requiring Car Wash Station To Construct Settling Catch Basin)Document3 pagesO10053-2006 (Requiring Car Wash Station To Construct Settling Catch Basin)CdeoCityCouncil100% (1)
- Fda Lto 2022Document2 pagesFda Lto 2022clarisse salvadorNo ratings yet
- Copyright Reg ReqDocument1 pageCopyright Reg ReqjeffdelacruzNo ratings yet
- PROCESS FLOW OF APPLICATION OF PNP LICENSES AND PERMITS - UPLB Oct 5 2016Document33 pagesPROCESS FLOW OF APPLICATION OF PNP LICENSES AND PERMITS - UPLB Oct 5 2016Trish AustriaNo ratings yet
- FDA Drugs Clearing Account FDA Drugs Clearing Account: Cashierposting@fda - Gov.ph Cashierposting@fda - Gov.phDocument6 pagesFDA Drugs Clearing Account FDA Drugs Clearing Account: Cashierposting@fda - Gov.ph Cashierposting@fda - Gov.phRFO REGION 5No ratings yet
- ALI FY 2018 Audited Financial Statements 2019 03 01 PDFDocument195 pagesALI FY 2018 Audited Financial Statements 2019 03 01 PDFGillian mae GarciaNo ratings yet
- 9-2 Directors Resolution Adopting AmendmentDocument1 page9-2 Directors Resolution Adopting AmendmentDaniel100% (2)
- Business Closure-Letter IntentDocument1 pageBusiness Closure-Letter IntentAlexis DawnNo ratings yet
- Letter of Retrenchment - Fazri - 2Document1 pageLetter of Retrenchment - Fazri - 2Khalid ZebNo ratings yet
- Explanation LetterDocument3 pagesExplanation LetterA M MngldNo ratings yet
- Annex B-3 RR 11-2018Document1 pageAnnex B-3 RR 11-2018Rheneir MoraNo ratings yet
- Itinerary For VisaDocument3 pagesItinerary For VisaUst LegMa SocNo ratings yet
- Increase of Authorized Capital Stock: Additional Requirements Depending On The Kind of Payment On SubscriptionDocument3 pagesIncrease of Authorized Capital Stock: Additional Requirements Depending On The Kind of Payment On SubscriptionsejinmaNo ratings yet
- General Employee NdaDocument1 pageGeneral Employee NdaMahendra Kumar SoniNo ratings yet
- Coversheet: Company Registration and Monitoring DepartmentDocument15 pagesCoversheet: Company Registration and Monitoring DepartmentMichael ViolandaNo ratings yet
- Response To Warning Letter DDocument4 pagesResponse To Warning Letter DVivian LeighNo ratings yet
- Pharmaceutical SOP ExampleDocument4 pagesPharmaceutical SOP ExampleFaysal AhmedNo ratings yet
- Board Resolution Approving LeaseDocument1 pageBoard Resolution Approving LeaseStephen HaldenNo ratings yet
- Sop RXDocument12 pagesSop RXGloria RamosNo ratings yet
- Amended Aoi - IcornerDocument5 pagesAmended Aoi - IcornerNhez LacsamanaNo ratings yet
- UCU - Ymana - MAJ - Capa PlanDocument3 pagesUCU - Ymana - MAJ - Capa PlanMajesty YmanaNo ratings yet
- Cebu City BarangaysDocument2 pagesCebu City BarangaysEgdar GigBitsNo ratings yet
- Visa Application Japan1 PDFDocument2 pagesVisa Application Japan1 PDFKean PagnaNo ratings yet
- Stock Replenishment FormDocument3 pagesStock Replenishment FormLiecel ValdezNo ratings yet
- Legal Medicine Digested Cases From PRC V de Guzman Up To Custodio V SandiganbayanDocument13 pagesLegal Medicine Digested Cases From PRC V de Guzman Up To Custodio V SandiganbayanJernel JanzNo ratings yet
- Supplier Information SheetDocument1 pageSupplier Information Sheetmind lastNo ratings yet
- DTI, SEC, BSP and BOI RequirementsDocument22 pagesDTI, SEC, BSP and BOI Requirementsni_kai2001No ratings yet
- Application of Article 2180 To Criminal Acts. - : Vicarious LiabilityDocument2 pagesApplication of Article 2180 To Criminal Acts. - : Vicarious LiabilityDon CorleoneNo ratings yet
- Affidavit of Loss Drivers LicenseDocument2 pagesAffidavit of Loss Drivers Licensegretchlegaspi_449102No ratings yet
- Carpool Services Contract PGPC PDFDocument76 pagesCarpool Services Contract PGPC PDFreneleponio1784100% (1)
- TR-Pharmacy Services NC IIIDocument149 pagesTR-Pharmacy Services NC IIILOLONo ratings yet
- Intimation Letter To Pay PremiumDocument1 pageIntimation Letter To Pay PremiumJSKlakshmiNo ratings yet
- CD Cover 2316 RR 2-2015 Annex BDocument1 pageCD Cover 2316 RR 2-2015 Annex BAndriana ArtiagaNo ratings yet
- Secretary's Certificate of MinutesDocument4 pagesSecretary's Certificate of MinutesSuzanne Pagaduan CruzNo ratings yet
- Job Offer - Goldtech HR Manager - Jennifer VacaroDocument3 pagesJob Offer - Goldtech HR Manager - Jennifer VacaroJeniffer VacaroNo ratings yet
- Procedures PurchasingDocument13 pagesProcedures PurchasingLeo Lopez100% (2)
- Checklist of Requirements For Lto Importer - WholesalerDocument1 pageChecklist of Requirements For Lto Importer - WholesalerJan Kevin GaliciaNo ratings yet
- Checklist FDADocument8 pagesChecklist FDAMargarita Mendoza-CadacioNo ratings yet
- Checklist of Requirements For Cosmetic EstablishmentsDocument7 pagesChecklist of Requirements For Cosmetic EstablishmentsKenneth James100% (1)
- CIR v. Mitsubishi FactsDocument2 pagesCIR v. Mitsubishi FactsMiguel PillasNo ratings yet
- DENR Pollution Control Officer - List of RequirementsDocument3 pagesDENR Pollution Control Officer - List of RequirementsMiguel Pillas0% (1)
- PCO Accreditation Application Form 2017Document3 pagesPCO Accreditation Application Form 2017Miguel Pillas100% (4)
- CrimPro CasesDocument2 pagesCrimPro CasesMiguel PillasNo ratings yet
- Pi DP Membership FormDocument2 pagesPi DP Membership FormMiguel PillasNo ratings yet
- Legal OpinionDocument7 pagesLegal OpinionMiguel PillasNo ratings yet
- CV Bangladesh DebnathDocument1 pageCV Bangladesh DebnathEd CanelaNo ratings yet
- Simple Employment Contract TemplateDocument4 pagesSimple Employment Contract TemplateFrancia CadizNo ratings yet
- Punjab Blood Safety Act 2015 VER 19 (22326)Document15 pagesPunjab Blood Safety Act 2015 VER 19 (22326)M Asif NaveedNo ratings yet
- Law On Secrecy of Bank DepositsDocument2 pagesLaw On Secrecy of Bank DepositsSofronio Padogdog100% (1)
- Rediff Moneywiz - My Portfolio(s)Document3 pagesRediff Moneywiz - My Portfolio(s)Vikramjit ਮਿਨਹਾਸNo ratings yet
- Open Letter To Governor Dayton From Leigh Turner December 20 2013Document2 pagesOpen Letter To Governor Dayton From Leigh Turner December 20 2013MarkingsonCaseNo ratings yet
- Certificate of Appearance Joebell G. ParagguaDocument2 pagesCertificate of Appearance Joebell G. ParagguajoebzNo ratings yet
- Tenant Design Manual PDFDocument373 pagesTenant Design Manual PDFAnousack Kittilath100% (1)
- List of Branches Visayas Balance TransferDocument4 pagesList of Branches Visayas Balance TransferMae Ann GonzalesNo ratings yet
- Applied PhysicsDocument5 pagesApplied Physicsahmad irtisamNo ratings yet
- Case BriefDocument2 pagesCase BriefGowri RNo ratings yet
- Data Domain InstructionsDocument2 pagesData Domain InstructionsD_23_desNo ratings yet
- Rudy J. Ramirez v. California, 476 U.S. 1152 (1986)Document2 pagesRudy J. Ramirez v. California, 476 U.S. 1152 (1986)Scribd Government DocsNo ratings yet
- UNDERTAKINGDocument4 pagesUNDERTAKINGvebhsrNo ratings yet
- Secrecy of Bank DepositDocument5 pagesSecrecy of Bank DepositAngelica RoblesNo ratings yet
- M Com Strategic Management Project TopicsDocument4 pagesM Com Strategic Management Project TopicsAdelle Moldovan60% (5)
- Ch. 2 Managerial Accounting: Prepared by Joseph R. Mendoza CPA, MBADocument1 pageCh. 2 Managerial Accounting: Prepared by Joseph R. Mendoza CPA, MBAMarlouieV.BatallaNo ratings yet
- Short Note On Question TagsDocument2 pagesShort Note On Question TagsDebaleena DuttaNo ratings yet
- 2005 Past GCE Questions A LEVELDocument7 pages2005 Past GCE Questions A LEVELteufackwambaNo ratings yet
- Perfection of The Contract of InsuranceDocument18 pagesPerfection of The Contract of InsuranceRacheal SantosNo ratings yet
- Chapter 11-Authority of Attorney: Power To Bind ClientDocument4 pagesChapter 11-Authority of Attorney: Power To Bind ClientRommel P. AbasNo ratings yet
- Sembang Santai Berisi Sabar Itu IndahDocument5 pagesSembang Santai Berisi Sabar Itu IndahAIMANNo ratings yet
- International Environmnet Law in IndiaDocument17 pagesInternational Environmnet Law in IndiaAnushka TRivediNo ratings yet
- Theories of Baptist OriginsDocument22 pagesTheories of Baptist OriginsDaniel Petre Ursu Slavu100% (1)
- Windeatt V Windeatt 91 1981 DMC BJ IIDocument8 pagesWindeatt V Windeatt 91 1981 DMC BJ IIPooshan UpadhyayNo ratings yet
- Lalwani V Lalwani - GD Final 24 4 17 PDFDocument39 pagesLalwani V Lalwani - GD Final 24 4 17 PDFEnoch LowNo ratings yet
- The Philippines in The 19th Century As Rizal's Context Economic, Social & Political AspectsDocument9 pagesThe Philippines in The 19th Century As Rizal's Context Economic, Social & Political AspectsBeaumont Serene Del ReigoNo ratings yet