Effectiveness of Aloe Vera Gel Compared With 1% Silver Sulphadiazine Cream As Burn Wound Dressing in Second Degree Burns
Effectiveness of Aloe Vera Gel Compared With 1% Silver Sulphadiazine Cream As Burn Wound Dressing in Second Degree Burns
Download as pdf or txt
You might also like
- The Healing Power of SoundDocument7 pagesThe Healing Power of SoundKate Kunkel86% (7)
- Illustrated Guide Percutaneous Collagen InductionDocument29 pagesIllustrated Guide Percutaneous Collagen InductionErik Brooks100% (1)
- Buffy The Vampire Slayer RPG - Slayer's Handbook PDFDocument157 pagesBuffy The Vampire Slayer RPG - Slayer's Handbook PDFSadisticSeraphNo ratings yet
- Efektifitas Tepid Sponge Bath Suhu 32 CDAN37 C Dalam Menurunkan Suhu Tubuh Anak Demam (The Effectiveness of Tepid Sponge Bath With 32Document7 pagesEfektifitas Tepid Sponge Bath Suhu 32 CDAN37 C Dalam Menurunkan Suhu Tubuh Anak Demam (The Effectiveness of Tepid Sponge Bath With 32Jeni TiaraNo ratings yet
- Sonatherapy White Paper For EM 2012Document5 pagesSonatherapy White Paper For EM 2012Gary Robert BuchananNo ratings yet
- Wound Closure ManualDocument127 pagesWound Closure ManualDougyStoffell100% (6)
- Wound Care Management in Indonesia Issues and Challenges in Diabetic Foot Ulceration PDFDocument5 pagesWound Care Management in Indonesia Issues and Challenges in Diabetic Foot Ulceration PDFlinda jurwitaNo ratings yet
- Modern and Classic Wound Dressing Comparison in WoDocument6 pagesModern and Classic Wound Dressing Comparison in WoJuan LuckyNo ratings yet
- 133 167 1 PB PDFDocument11 pages133 167 1 PB PDFratnaummudzakyNo ratings yet
- Makalah GADAR Kel.5 Mekanisme Cedera, Initial Assessment (Primary & Secondary Survey) & AB ManagementDocument43 pagesMakalah GADAR Kel.5 Mekanisme Cedera, Initial Assessment (Primary & Secondary Survey) & AB ManagementInsosNo ratings yet
- Jurnal Paliatif AdhityaDaiskyYanuarDocument5 pagesJurnal Paliatif AdhityaDaiskyYanuarDaisky Rafif MaulanaNo ratings yet
- Hubungan Tingkat StresDocument8 pagesHubungan Tingkat StresAri SuhartantoNo ratings yet
- Daftar Jurnal KeperawatanDocument6 pagesDaftar Jurnal KeperawatanRayuwanda Ayu100% (5)
- Pengaruh Pemberian Jus Belimbing Manis Terhadap Penurunan Tekanan Darah Pada Penderita Hipertensi Di Panti Werdha Bina Bhakti Serpong TAHUN 2018Document17 pagesPengaruh Pemberian Jus Belimbing Manis Terhadap Penurunan Tekanan Darah Pada Penderita Hipertensi Di Panti Werdha Bina Bhakti Serpong TAHUN 2018Siti SugiartiNo ratings yet
- PDF Sap Pkmrs Jiwa Manfaat Kontrol Dan Minum Obat Secara Teratur Dan Peran Keluarga Dalam Mencegah Kekambuhan Pada Pasien Gangguan Jiwa CompressDocument8 pagesPDF Sap Pkmrs Jiwa Manfaat Kontrol Dan Minum Obat Secara Teratur Dan Peran Keluarga Dalam Mencegah Kekambuhan Pada Pasien Gangguan Jiwa CompressErma Cahyani45No ratings yet
- Jurnal Mobilisasi DiniDocument12 pagesJurnal Mobilisasi Diniapriliani nuraisiyahNo ratings yet
- Analisa Jurnal PicotDocument9 pagesAnalisa Jurnal PicotYolly NadhaNo ratings yet
- Peran Perawat Pada Situasi Tanggap DaruratDocument24 pagesPeran Perawat Pada Situasi Tanggap DaruratAddi Mardi HarnantoNo ratings yet
- Makalah Pain Management p&Np-2Document12 pagesMakalah Pain Management p&Np-2damarNo ratings yet
- Anatomi Dan Fisiologi Sistem PersyarafanDocument37 pagesAnatomi Dan Fisiologi Sistem PersyarafanAnonymous xfBKTQfNo ratings yet
- Jurnal Skripsiku PENGARUH ANESTESI SPINAL TERHADAP TEKANAN DARAH PASIEN OPERASI DI RUANG FLAMBOYAN RSUD PANDAN ARANG BOYOLALIDocument13 pagesJurnal Skripsiku PENGARUH ANESTESI SPINAL TERHADAP TEKANAN DARAH PASIEN OPERASI DI RUANG FLAMBOYAN RSUD PANDAN ARANG BOYOLALIratmanNo ratings yet
- Development Theory of Nursing: By. Dr. Joni Haryanto, S.KP., NS., M.SiDocument32 pagesDevelopment Theory of Nursing: By. Dr. Joni Haryanto, S.KP., NS., M.Siratna220693No ratings yet
- Physical Activity and Premenstrual Syndrome in TeenagersDocument23 pagesPhysical Activity and Premenstrual Syndrome in TeenagersFadillah RosyidahNo ratings yet
- Hubungan Komunikasi Terapeutik Perawat Dengan Kepuasan Pasien Di Ruang Rawat Inap Irina A Rsup Prof. Dr. R. D. Kandou ManadoDocument22 pagesHubungan Komunikasi Terapeutik Perawat Dengan Kepuasan Pasien Di Ruang Rawat Inap Irina A Rsup Prof. Dr. R. D. Kandou ManadonartiNo ratings yet
- Judul Hubungan Self Efficacy Dengan Self Care Di Ruang Poli Interna Rsud Labuang Baji MakassarDocument15 pagesJudul Hubungan Self Efficacy Dengan Self Care Di Ruang Poli Interna Rsud Labuang Baji MakassarErina AdrianaNo ratings yet
- Endoscopic Endonasal Transsphenoidal Surgery For Pituitary Macroadenoma As Minimal Invasive Approach: Case ReportDocument6 pagesEndoscopic Endonasal Transsphenoidal Surgery For Pituitary Macroadenoma As Minimal Invasive Approach: Case ReportDokter FebyanNo ratings yet
- Program Studi Profesi Ners Sekolah Tinggi Ilmu Kesehatan Muhammadiyah Samarinda 2017Document49 pagesProgram Studi Profesi Ners Sekolah Tinggi Ilmu Kesehatan Muhammadiyah Samarinda 2017Rhynii HasryyNo ratings yet
- Konsep Dasar FK PDFDocument27 pagesKonsep Dasar FK PDFStefanie Pramudita JayaNo ratings yet
- Jurnal k3 PDFDocument10 pagesJurnal k3 PDFDen's CivilNo ratings yet
- Whoqol Hiv Bref PDFDocument5 pagesWhoqol Hiv Bref PDFIndra DwinataNo ratings yet
- Pengaruh Hipnoterapi Terhadap Nyeri Pada Pasien Dispepsia Di Rsud Dr. R. Goeteng Taruna Dibrata PurbalinggaDocument12 pagesPengaruh Hipnoterapi Terhadap Nyeri Pada Pasien Dispepsia Di Rsud Dr. R. Goeteng Taruna Dibrata PurbalinggaRahmi Eka PutriNo ratings yet
- Non-Pharmacological Methods and Post-Operative Pain Relief: An Observational StudyDocument7 pagesNon-Pharmacological Methods and Post-Operative Pain Relief: An Observational StudyAsti DwiningsihNo ratings yet
- Peran Perawat Dalam Penanggulangan Bencana: Vol 6, No 1 Mei, Pp. 63-70 P-ISSN 2549-4880, E-ISSN 2614-1310 WebsiteDocument8 pagesPeran Perawat Dalam Penanggulangan Bencana: Vol 6, No 1 Mei, Pp. 63-70 P-ISSN 2549-4880, E-ISSN 2614-1310 WebsiteEbato SanaeNo ratings yet
- Henny Dwi Susanti CVDocument4 pagesHenny Dwi Susanti CVIndra GunawanNo ratings yet
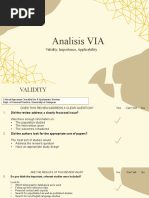
- Analisis VIA: Validity, Importance, ApplicabilityDocument7 pagesAnalisis VIA: Validity, Importance, Applicabilitysukma nugrohoNo ratings yet
- Pengaruh Terapi Relaksasi Autogenik Terhadap Tingkat Kualitas Tidur Pada Lanjut UsiaDocument8 pagesPengaruh Terapi Relaksasi Autogenik Terhadap Tingkat Kualitas Tidur Pada Lanjut UsiaEla NurlaelaNo ratings yet
- Manuskrip Terapi Musik Terhadap IntensitDocument8 pagesManuskrip Terapi Musik Terhadap Intensitagustian trihatmokoNo ratings yet
- Resilience Definitions, Theory, and Challenges: Interdisciplinary PerspectivesDocument15 pagesResilience Definitions, Theory, and Challenges: Interdisciplinary PerspectivesAlex BanicaNo ratings yet
- Jurnal ARDSDocument17 pagesJurnal ARDSwahyuNo ratings yet
- Wound Bed PreparationDocument24 pagesWound Bed PreparationnudiaNo ratings yet
- Dengue Shock Syndrome: Dr. Elsye Souvriyanti, SpaDocument18 pagesDengue Shock Syndrome: Dr. Elsye Souvriyanti, SpaYesi Maulani NovitasariNo ratings yet
- Gilang YA G2A009181 Bab8KTI DafpusDocument23 pagesGilang YA G2A009181 Bab8KTI DafpusNurbaitiNo ratings yet
- Askep Kritis Sistem EndokrinDocument37 pagesAskep Kritis Sistem EndokrinDerfina Bahagia iduNo ratings yet
- Brief COPE ScaleDocument4 pagesBrief COPE ScaleSri Padma SariNo ratings yet
- Gambaran Interaksi Sosial Lansia Di MasyarakatDocument8 pagesGambaran Interaksi Sosial Lansia Di MasyarakatLatuary JosephNo ratings yet
- ATTID Questionnaire Court Interactif enDocument8 pagesATTID Questionnaire Court Interactif enTran PhuocNo ratings yet
- Clinical Use of MEBO in Wound Management in UAE PDFDocument7 pagesClinical Use of MEBO in Wound Management in UAE PDFUus SuparmanNo ratings yet
- Pengambilan Keputusan Klinis Perawat: Jurnal Ilmiah Kesehatan 2020Document11 pagesPengambilan Keputusan Klinis Perawat: Jurnal Ilmiah Kesehatan 2020Dafarasyad DafarasyadNo ratings yet
- Medoroga& Its ManagementDocument6 pagesMedoroga& Its ManagementChintamani VeerrajuNo ratings yet
- Dokumentasi Pre Dan Post Conference Semi MPKP Ruang KulimDocument10 pagesDokumentasi Pre Dan Post Conference Semi MPKP Ruang KulimMarni EllyzaNo ratings yet
- Analisa Teori Wound HailerDocument3 pagesAnalisa Teori Wound HailerAgis TaufikNo ratings yet
- Lisa Mustika Sari, Niche Ardila: Niche - A@yahoo - Co.idDocument6 pagesLisa Mustika Sari, Niche Ardila: Niche - A@yahoo - Co.idirfan wabula100% (1)
- Wound Bed Preparation (Ria Andjarwati, SKP - Etn)Document27 pagesWound Bed Preparation (Ria Andjarwati, SKP - Etn)Gede JuanamastaNo ratings yet
- AnginaDocument59 pagesAnginaVevi InakuNo ratings yet
- Skripsi Full Tanpa Bab PembahasanDocument53 pagesSkripsi Full Tanpa Bab Pembahasanfani akifaazriNo ratings yet
- Role Play Distress SpiritualDocument4 pagesRole Play Distress Spiritualarya7316042No ratings yet
- Terapi Modalitas Terapi LingkunganDocument5 pagesTerapi Modalitas Terapi Lingkunganni luh ade seriasihNo ratings yet
- Uji Validitas Kuesioner Dukungan KeluargaDocument1 pageUji Validitas Kuesioner Dukungan Keluargapitria100% (1)
- Implementasi Evidence Based Nursing Pada Pasien Dengan Stroke Non-Hemoragik: Studi KasusDocument7 pagesImplementasi Evidence Based Nursing Pada Pasien Dengan Stroke Non-Hemoragik: Studi KasusHerman HermanNo ratings yet
- A Herbal Cream Consisting of Aloe Vera, Lavandula Silver Sulfadiazine in Burn ManagementDocument6 pagesA Herbal Cream Consisting of Aloe Vera, Lavandula Silver Sulfadiazine in Burn ManagementWalaa ElleithyNo ratings yet
- Double-Blind, Randomized, Placebo-Controlled Study of Topical 5% Acyclovir-1% Hydrocortisone Cream (ME-609) for Treatment of UV Radiation-Induced Herpes Labialis - Evans 2002Document5 pagesDouble-Blind, Randomized, Placebo-Controlled Study of Topical 5% Acyclovir-1% Hydrocortisone Cream (ME-609) for Treatment of UV Radiation-Induced Herpes Labialis - Evans 2002NataliaNo ratings yet
- Lasers Surg Med - 2021 - Eubanks - Safety and efficacy of fractional radiofrequenion of acneDocument8 pagesLasers Surg Med - 2021 - Eubanks - Safety and efficacy of fractional radiofrequenion of acnemarialinda7755233No ratings yet
- Questionnaire Survey of The Efficacy of Emollients For Adult Patients With Atopic DermatitisDocument5 pagesQuestionnaire Survey of The Efficacy of Emollients For Adult Patients With Atopic DermatitisRemaja IslamNo ratings yet
- 1 s2.0 S0190962224018218 MainDocument1 page1 s2.0 S0190962224018218 MainMohammed AlmnsoobNo ratings yet
- Atopic Dermatitis: New Perspectives on Managing a Chronic Inflammatory DiseaseFrom EverandAtopic Dermatitis: New Perspectives on Managing a Chronic Inflammatory DiseaseRating: 5 out of 5 stars5/5 (1)
- Rekap Absen Briefing Firts TakerDocument2 pagesRekap Absen Briefing Firts TakerBayuNo ratings yet
- Knowledge & Practice of Nursing Ethics and Laws: Riginal RticleDocument4 pagesKnowledge & Practice of Nursing Ethics and Laws: Riginal RticleBayuNo ratings yet
- Vanasco N Clinical Characteristics and Risk...Document4 pagesVanasco N Clinical Characteristics and Risk...BayuNo ratings yet
- Risk Factors For Leptospirosis in Urban Flooding: A Literature ReviewDocument49 pagesRisk Factors For Leptospirosis in Urban Flooding: A Literature ReviewBayuNo ratings yet
- Natures.n1 Healing - SecretDocument29 pagesNatures.n1 Healing - Secretwikorv8497100% (1)
- Wound Healing Concepts in Clinical Practice of OMFDocument23 pagesWound Healing Concepts in Clinical Practice of OMFrozh rasulNo ratings yet
- Introductory Q Bank (Pathology MCQ)Document9 pagesIntroductory Q Bank (Pathology MCQ)EZHIL N100% (2)
- A Comparative Evaluation of Efficacy of Tetracycline HCL, Edta & Hyaluronic Acid Gel As Root Biomodification Agents. - An In-Vitro Sem StudyDocument11 pagesA Comparative Evaluation of Efficacy of Tetracycline HCL, Edta & Hyaluronic Acid Gel As Root Biomodification Agents. - An In-Vitro Sem StudyIJAR JOURNALNo ratings yet
- List of 488 Power Affirmations: Believe in The Creative Power of Your Own MindDocument35 pagesList of 488 Power Affirmations: Believe in The Creative Power of Your Own MindgopinathaskuNo ratings yet
- Surgery Lec 2Document26 pagesSurgery Lec 2Eman NazzalNo ratings yet
- Wound Healing, Tissue Repair, and FibrosisDocument28 pagesWound Healing, Tissue Repair, and FibrosisRibka Theodora100% (1)
- Positive Affirmations For HealthDocument3 pagesPositive Affirmations For HealthAR GNo ratings yet
- MS LAB Week 3Document6 pagesMS LAB Week 3Rouwi DesiatcoNo ratings yet
- Principles of Wound HealingDocument8 pagesPrinciples of Wound HealingTracy100% (6)
- Wound Healing in The Oral Mucosa: Patricio C. Smith and Constanza MartínezDocument14 pagesWound Healing in The Oral Mucosa: Patricio C. Smith and Constanza MartínezNadira NurinNo ratings yet
- Gastrointestinal - Mucosal.repair - And.experimental - Therapeutics Ublog - TKDocument261 pagesGastrointestinal - Mucosal.repair - And.experimental - Therapeutics Ublog - TKpotaiskiNo ratings yet
- Pathomorophology. (Medicine, 3 Course)Document10 pagesPathomorophology. (Medicine, 3 Course)Joy JoyNo ratings yet
- ATI Remediation Template practice B.docxDocument3 pagesATI Remediation Template practice B.docxtkekipinuuanu2020No ratings yet
- Chapter 3 - Protocols For Decellularization of Human Amniotic MembraneDocument11 pagesChapter 3 - Protocols For Decellularization of Human Amniotic MembraneravhcolNo ratings yet
- PRP in DermatologyDocument36 pagesPRP in DermatologySuryakant HayatnagarkarNo ratings yet
- Ethereal Crystals 1 - 9 Revised ManualDocument52 pagesEthereal Crystals 1 - 9 Revised ManualBelanitaAbreu100% (1)
- Advanced Derm AustraliaDocument3 pagesAdvanced Derm AustraliaovieNo ratings yet
- Oral Pathology - Study NotesDocument9 pagesOral Pathology - Study Notesapi-347345383No ratings yet
- MLC InjuryDocument26 pagesMLC Injuryharsh89100% (3)
- Soft Tissue Injuries-2Document11 pagesSoft Tissue Injuries-2api-298014898No ratings yet
- MIT20 441JF09 Lec02b MsDocument61 pagesMIT20 441JF09 Lec02b Mssinsis4254No ratings yet
- Botswana-Agate Properties: Thousand-Layer QuartzDocument2 pagesBotswana-Agate Properties: Thousand-Layer Quartzudemyandroid IITNo ratings yet
- Physiological Roles of MacrophagesDocument10 pagesPhysiological Roles of MacrophagesBasideu ByinajuNo ratings yet
- Why Wounds Fail To HealDocument6 pagesWhy Wounds Fail To HealMsPocketbook HoarderNo ratings yet