
Blue Protocol
Uploaded by
oana florianaBlue Protocol
Uploaded by
oana florianaRelevance of Lung Ultrasound in the
Diagnosis of Acute Respiratory Failure * :
The BLUE Protocol
Daniel A. Lichtenstein and Gilbert A. Mezière
Chest 2008;134;117-125; Prepublished online April 10, 2008;
DOI 10.1378/chest.07-2800
The online version of this article, along with updated information and
services can be found online on the World Wide Web at:
http://chestjournal.chestpubs.org/content/134/1/117.full.html
Supplemental material related to this article is available at:
http://chestjournal.chestpubs.org/content/suppl/2009/03/19/chest.07-280
0.DC1.html
Chest is the official journal of the American College of Chest
Physicians. It has been published monthly since 1935.
Copyright2008by the American College of Chest Physicians, 3300
Dundee Road, Northbrook, IL 60062. All rights reserved. No part of
this article or PDF may be reproduced or distributed without the prior
written permission of the copyright holder.
(http://chestjournal.chestpubs.org/site/misc/reprints.xhtml)
ISSN:0012-3692
Downloaded from chestjournal.chestpubs.org at Borland Medical Library on June 28, 2012
© 2008 American College of Chest Physicians
Original Research
CRITICAL CARE MEDICINE
Relevance of Lung Ultrasound in the
Diagnosis of Acute Respiratory Failure*
The BLUE Protocol
Daniel A. Lichtenstein, MD, FCCP; and Gilbert A. Mezière, MD
Background: This study assesses the potential of lung ultrasonography to diagnose acute respiratory
failure.
Methods: This observational study was conducted in university-affiliated teaching-hospital ICUs. We
performed ultrasonography on consecutive patients admitted to the ICU with acute respiratory failure,
comparing lung ultrasonography results on initial presentation with the final diagnosis by the ICU team.
Uncertain diagnoses and rare causes (frequency < 2%) were excluded. We included 260 dyspneic patients
with a definite diagnosis. Three items were assessed: artifacts (horizontal A lines or vertical B lines
indicating interstitial syndrome), lung sliding, and alveolar consolidation and/or pleural effusion. Com-
bined with venous analysis, these items were grouped to assess ultrasound profiles.
Results: Predominant A lines plus lung sliding indicated asthma (n ⴝ 34) or COPD (n ⴝ 49) with 89%
sensitivity and 97% specificity. Multiple anterior diffuse B lines with lung sliding indicated pulmonary
edema (n ⴝ 64) with 97% sensitivity and 95% specificity. A normal anterior profile plus deep venous
thrombosis indicated pulmonary embolism (n ⴝ 21) with 81% sensitivity and 99% specificity. Anterior
absent lung sliding plus A lines plus lung point indicated pneumothorax (n ⴝ 9) with 81% sensitivity
and 100% specificity. Anterior alveolar consolidations, anterior diffuse B lines with abolished lung
sliding, anterior asymmetric interstitial patterns, posterior consolidations or effusions without
anterior diffuse B lines indicated pneumonia (n ⴝ 83) with 89% sensitivity and 94% specificity. The
use of these profiles would have provided correct diagnoses in 90.5% of cases.
Conclusions: Lung ultrasound can help the clinician make a rapid diagnosis in patients with acute
respiratory failure, thus meeting the priority objective of saving time.
(CHEST 2008; 134:117–125)
Key words: chest ultrasonography; COPD; ICU; interstitial syndrome; lung, ultrasound diagnosis; pneumothorax; pulmonary
edema; respiratory failure
Abbreviations: BLUE ⫽ Bedside Lung Ultrasound in Emergency; PLAPS ⫽ posterolateral alveolar and/or pleural syndrome
A ing
cute respiratory failure is one of the most distress-
situations for the patient. Emergency cases do
immediate diagnosis, which sometimes compromises
outcome.1–3 Physical examination and bedside radiog-
not always present in conditions that are ideal for raphy are imperfect,4,5 resulting in a need for sophisti-
cated test results that delay management.
*From the Service de Réanimation Médicale (Dr. Lichtenstein), Ultrasound has long shown its utility for plain
Hôpital Ambroise-Paré, F-92 Boulogne, Paris-Ouest; and Service
de Réanimation Polyvalente (Dr. Mezière), Centre Hospitalier, organs.6 Although the lung has traditionally been
F-92 Saint-Cloud, Paris-Ouest, France. excluded from its repertoire,7 studies have proven
This work was presented partly at the twenty-third ISICEM, that this belief was unfounded.8 Since 1989 in our
Brussels, March 30, 2003.
The authors have no conflicts of interest to disclose. ICU, using devoted logistics,9 the concept of whole-
Manuscript received November 17, 2007; revision accepted body ultrasound was developed and extended to the
February 16, 2008. lungs for managing critical situations.10,11 Lung ul-
Reproduction of this article is prohibited without written permission
from the American College of Chest Physicians (www.chestjournal. trasonography is becoming a standard tool in critical
org/misc/reprints.shtml). care. Accurate bedside detection of thoracic disor-
Correspondence to: Daniel A. Lichtenstein, MD, FCCP, Service ders should help diagnose acute respiratory failure.12
de Réanimation Médicale, Hôpital Ambroise-Paré, F-92100 Bou-
logne, Faculté Paris-Ouest, France; e-mail: dlicht@free.fr This study examines this potential, as discussed
DOI: 10.1378/chest.07-2800 previously.13
www.chestjournal.org CHEST / 134 / 1 / JULY, 2008 117
Downloaded from chestjournal.chestpubs.org at Borland Medical Library on June 28, 2012
© 2008 American College of Chest Physicians
Table 1—Final Diagnoses and Methods of Diagnosis
Diagnoses Methods
For all patients History, clinical examination, radiography read by radiologists, CT when available (n ⫽ 38),
favorable clinical progression under treatment, and:
Cardiogenic pulmonary edema Evaluation of cardiac function using echocardiography, functional tests, and American Heart
(referred to as pulmonary Association recommendations
edema) 关n ⫽ 64兴
Pneumonia (n ⫽ 83) Infectious profile, radiologic asymmetry, microorganism isolated (blood, invasive tests), recovery with
antibiotics. Included were infectious, aspiration, community, or hospital-acquired pneumonia.
Pneumonia complicating chronic respiratory disease was classified as pneumonia. Beginning ARDS (n ⫽ 7)
and massive atelectasis (n ⫽ 1) were included in this group
Decompensated chronic respiratory Condition defined as exacerbation of chronic respiratory disease without pneumonia, pneumothorax,
disease (referred to as COPD) pulmonary edema, pleurisy, or pulmonary embolism. COPD was confirmed by functional tests.
关n ⫽ 49兴 Patients with simple bronchial superinfection were classified in this case. COPD patients with
pneumonia, pneumothorax, etc, were first considered as pneumonia, pneumothorax, etc
Acute asthma (n ⫽ 34) History, responds to bronchodilator treatment
Pulmonary embolism (n ⫽ 21) Helical CT
Pneumothorax (n ⫽ 9) Radiography (CT if necessary)
Excluded patients
Rare (⬍ 2%) causes (n ⫽ 9) Chronic diffuse interstitial disease (n ⫽ 4), massive pleural effusion (n ⫽ 3), fat embolism (n ⫽ 1),
tracheal stenosis (n ⫽ 1). Note: no dyspnea due to pericardial effusion in this consecutive series
No final diagnosis (n ⫽ 16) Unknown diagnosis at the end of hospitalization, progression preventing conclusions
Several final diagnoses (n ⫽ 16) Pulmonary edema plus pneumonia (n ⫽ 10), pulmonary edema plus COPD (n ⫽ 3), others (n ⫽ 3)
Materials and Methods (Table 1). Acute respiratory failure was defined based on the
classical clinical and biological criteria for requiring admission
This was an observational study conducted in university-affiliated to the ICU. All patients had an ultrasound test by investigators
hospitals over 4 years investigating 301 consecutive adult patients (D.L., G.M.) who did not participate in the patient’s manage-
with acute respiratory failure. The official diagnosis was established ment, which was undertaken by other ICU members blinded
in the hospitalization report using standardized tests by the ICU staff to the ultrasound results. The ultrasound test was performed
and not including lung ultrasound data (Table 1). Sixteen patients without interrupting management at the time of ICU admis-
never received a definite diagnosis, 16 patients had several official sion (ie, within 20 min) and lasted ⬍ 3 min. The internal
diagnoses, and 9 patients had rare (ie, frequency ⬍ 2%) diagnoses. review board of the hospital approved this study and waived
To simplify this study, these patients were subsequently excluded the requirement for informed consent.
Table 2—Comprehensive Results*
Predominant A Lines
on One Side, and
Bilateral-Predominant Bilateral-Predominant Alveolar Predominant B ⫹
Anterior Pattern A Lines B ⫹ Lines Consolidation Lines on Other Side A Lines
Lung sliding ⫹ ⫺ ⫹ ⫺ ⫹ ⫹ ⫺ ⫺ ⫹ ⫹ ⫺ ⫺ ⫹ ⫹ ⫺ ⫺ ⫺ plus lung point
PLAPS Yes Yes No No Yes No Yes No Yes No Yes No Yes No Yes No Any
Pulmonary edema 2 0 0 0 541 8 0 0 0 0 0 0 0 0 0 0 0
COPD 2 1 38 4 2 1 0 0 1 0 0 0 0 0 0 0 0
Asthma 1 0 331 0 0 0 0 0 0 0 0 0 0 0 0 0 0
Pulmonary embolism 108 0 109 0 0 0 0 0 0 0 10 0 0 0 0 0 0
Pneumothorax 0 0 0 1 0 0 0 0 0 0 0 0 0 0 0 0 8
Pneumonia 34 1 3 0 4 2 9 0 7 2 9 0 7 1 4 0 0
A and A⬘ Normal B profile B⬘ profile C profile A/B profile Pneumothorax
profile profile, profile
plus and A⬘
PLAPS profile
without
PLAPS
*Exponent indicates No. of cases with venous thrombosis (datum without exponent means negative venous exploration).
118 Original Research
Downloaded from chestjournal.chestpubs.org at Borland Medical Library on June 28, 2012
© 2008 American College of Chest Physicians
parietal pleura,15 and A lines (Fig 2), these repetitive horizontal
artifacts arising from the pleural line generated by subpleural air,
which, either intraalveolar or pure (pneumothorax), blocks ultra-
sound waves. Normal interlobular septa are not detected. Three
signs with dual answers were assessed, as follow.
Artifact Analysis: A or B Lines: The B line is the name given to
an artifact with seven features: a hydroaeric comet-tail artifact;
arising from the pleural line; hyperechoic; well defined; spread-
ing up indefinitely; erasing A lines; and moving with lung sliding
when lung sliding is present (Fig 3). It reflects the coexistence of
elements with a major acoustic impedance gradient, such as fluid
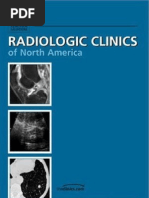
Figure 1. Ultrasound areas. Stage 1 defines the investigation of the and air. Fluid at the subpleural interlobular septum surrounded
anterior chest wall (zone 1) in a supine patient (1⬘ in this semire- by air-filled alveoli (ie, septal edema) fulfills this condition. Three
cumbent patient). Stage 2 adds the lateral wall (zone 2) [left panel]. or more B lines in a single view are called B ⫹ lines. B ⫹ lines
Stage 3 adds the posterolateral chest wall using a short probe, indicate the subpleural part of interstitial syndrome.16 Other
moving the patient only minimally (zone 3) [right panel]. Each wall comet-tail artifacts can be seen; none has B line characteristics.14
is divided into upper and lower halves, resulting in six areas of
investigation. Note the shape of the microconvex probe, which Lung Sliding: Present or Abolished: Abolition (Fig 4) occurs
allows satisfactory analysis of the intercostal space, and satisfactorily when the visceral pleura does not slide against parietal pleura
controlled compression maneuvers at the veins investigated in this (inflammatory adherences, loss of lung expansion, atelectasis,
study: internal jugular, subclavian, iliofemoropopliteal veins, and as apnea, chronic symphysis) or is separated (pneumothorax, pneu-
far as possible, inferior vena cava and calf veins. monectomy). If abolished lung sliding is associated with A lines,
the search for pneumothorax is mandatory. The lung point is a
specific sign of pneumothorax, alternating lung sliding and
abolished lung sliding plus A lines at the same location.17
Ultrasound Approach Alveolar Consolidation and/or Pleural Effusion: Absent or
Present: Pleural effusion classically yields an anechoic-dependent
Ultrasound was performed (Hitachi-405; Hitachi Medical; Tokyo,
pattern (Fig 5),18 an inconstant criterion. The roughly quadran-
Japan) with a 5-MHz microconvex probe (Fig 1). Patients were
gular shape with a regular lower border (the visceral pleura,
investigated in a semirecumbent position, or were supine if intu-
called the lung line) was required for the diagnosis. The inspira-
bated (n ⫽ 35). Scans were longitudinal. The pleural line, sought
tory shift of the lung line toward the pleural line is called the
between two rib shadows, indicates the pleural layers. The normal
sinusoid sign. The sensitivity of these signs is 92%, and specificity
lung14 displays lung sliding, a movement in rhythm with respiration
is 97%.5,19 Alveolar consolidation20 results in fluid-filled alveoli.
at the pleural line, indicating sliding of the visceral pleura against the
The alveolar-interstitial interfaces generate reflections yielding a
tissular pattern, absence of the lung line, absence of the sinusoid
sign. Ultrasound sensitivity is 90%, and specificity is 98%.21
Figure 2. Normal lung surface. Longitudinal scan of an inter-
costal space. Left panel: Pleural line and A line (real-time). The
pleural line is located 0.5 cm below the rib line in the adult. Its
visible length between two ribs in the longitudinal scan is
approximately 2 cm. The upper rib, pleural line, and lower rib
(vertical arrows) outline a characteristic pattern called the bat Figure 3. Interstitial syndrome. These vertical comet-tail arti-
sign. The horizontal lines arising from the pleural line (horizontal facts arise strictly from the pleural line, are well defined (laser-
arrows) are separated by regular intervals that are equal to the like), hyperechoic, move with lung sliding, spread to the edge of
distance between the skin and the pleural line. These were called the screen without fading, and erase A lines (dotted arrows
A lines. A lines are usually large (see upper line) but can be indicate their theoretical location). This pattern defines B lines.
shorter (lower line), which has no clinical significance. Right Several B lines in a single view, reminiscent of a rocket at lift-off,
panel: M mode. An obvious difference appears on either side of are called lung rockets, or B ⫹ lines (featuring here, B3 lines).
the pleural line (arrow). The motionless superficial layers gener- Diffuse lung rockets indicate interstitial syndrome. One or two B
ate horizontal lines. Lung dynamics generate lung sliding (sandy lines in a single view, referred to as the b line, have no pathologic
pattern). This pattern is called the seashore sign. significance. This patient had cardiogenic pulmonary edema.
www.chestjournal.org CHEST / 134 / 1 / JULY, 2008 119
Downloaded from chestjournal.chestpubs.org at Borland Medical Library on June 28, 2012
© 2008 American College of Chest Physicians
Study Design
The signs observed in each disease were methodically col-
lected; then the ultrasound data were compared with the diag-
nosis established by the ICU team.
Results
This study included 260 patients with a definite
diagnosis: 140 men and 120 women (mean age, 68
years; range, 22 to 91 years; SD, 16 years).
Signs Observed
Pulmonary Edema: Pulmonary edema was ob-
served in 64 patients. Anterior-predominant bilateral
B ⫹ lines were observed in 62 cases (diffuse in 59,
Figure 4. Pneumothorax. Left panel (real-time): one significant
item is the complete absence of the B line. Lower arrows: A lines;
predominant involvement of lower halves in 3).
upper arrow: pleural line. Right panel (M mode): this succession Anterior-predominant bilateral A lines were seen in
of horizontal lines indicates complete absence of dynamics at, and two cases. Anterior lung sliding was always pre-
below, the pleural line (arrowheads). This pattern is called the
stratosphere sign. The lung point (not featured here) confidently
served. In 56 cases, PLAPS was detectable. One
rules in the diagnosis. patient (with B ⫹ lines) had internal jugular vein
thrombosis.
Deep venous thrombosis was sought using the same probe.22 COPD: COPD was observed in 49 patients. In 38
Visualization of anatomic echoic intraluminal thrombosis or cases, anterior-predominant bilateral A lines with
absence of compressibility was considered as a positive finding lung sliding and no PLAPS were observed. In five
(Fig 1). An examination combined an anterior approach (analyz- cases, the same pattern with abolished lung sliding
ing artifacts, lung sliding, alveolar consolidation), a lateral sub-
posterior search for posterolateral alveolar and/or pleural syn-
(without lung point) was seen. Anterior-predominant
drome (PLAPS), and venous analysis. bilateral B lines were present in three cases, anterior
consolidation in one. PLAPS was seen in six cases.
Status Asthmaticus: Status asthmaticus was observed
in 34 patients. Asthma gave anterior-predominant A
lines with lung sliding in all cases, posterior consolida-
tion in one, and calf thrombosis in another.
Pulmonary Embolism: Pulmonary edema was ob-
served in 21 patients. Twenty patients had anterior-
predominant A lines with lung sliding. One had
anterior consolidation with absent lung sliding.
PLAPS was found in 11 patients. Seventeen patients
had venous thrombosis.
Pneumothorax: Pneumothorax was observed in
Figure 5. Pleural effusion and alveolar consolidation; typical
example of PLAPS. Left panel: real-time, stage 2. The quad sign:
nine patients. Abolished anterior lung sliding was
a pleural effusion on expiration (E) is delineated between the associated with anterior-predominant A lines in all
pleural line (upper white arrows) and the lung line, always cases. Lateroposterior lung point was present in
regular, which indicates the visceral pleura (lower white arrows).
The shred sign: a lower-lobe alveolar consolidation (LL) yields a
eight cases. PLAPS was found in five cases.
tissular pattern, characteristically limited by the lung line (or the
pleural line when there is no effusion) and in depth by an Pneumonia: Pneumonia was observed in 83 pa-
irregular border (black arrows), the shred line, as in connection
with aerated lung. Below, air artifacts are displayed. Between tients. In 75 cases, PLAPS was present. In six cases,
consolidation and spleen (S) is the diaphragm, a basic landmark an anterior-predominant bilateral B ⫹ pattern was
in stage 2. Right panel: time-motion demonstrates the sinusoid associated with lung sliding (with PLAPS in four
sign, a basic dynamic sign of pleural effusion. The sign will not be
generated by alveolar consolidation, which behaves like a solid cases). In nine cases, anterior-predominant bilateral
lesion. B ⫹ lines were associated with abolished lung sliding;
120 Original Research
Downloaded from chestjournal.chestpubs.org at Borland Medical Library on June 28, 2012
© 2008 American College of Chest Physicians
Table 3—Combined Results*
Normal Profile, and A’
Diagnoses A Profile Plus PLAPS Profile Without PLAPS B Profile B’ Profile C Profile A/B Profile Lung Point
1
Pulmonary edema 2 0 62 0 0 0 0
COPD or asthma 4 751 3 0 1 0 0
Pulmonary embolism 108 109 0 0 10 0 0
Pneumothorax 0 1 0 0 0 0 8
Pneumonia 35 3 6 9 18 12 0
*Exponents indicate No. of cases with venous thrombosis (datum without exponent means negative venous exploration). To simplify this Table,
COPD and asthma are considered together; three columns in Table 2 were combined because analysis showed no loss in performance. One
patient with pneumonia and the A’ profile plus PLAPS was inserted in the A profile plus PLAPS column. The term lung point implies abolished
anterior sliding associated with anterior A lines.
PLAPS was always associated. In 12 cases, anterior- The A’ profile is an A profile with abolished lung
predominant B ⫹ lines in one lung coexisted with sliding and without lung point. The B profile desig-
predominant A lines in the contralateral lung; nates anterior-predominant bilateral B ⫹ lines asso-
PLAPS was seen in 11 cases. In 18 cases, anterior ciated with lung sliding (with possible focalized A
consolidations were observed; lung sliding was abol- lines). The B’ profile is a B profile with abolished
ished in 9 of them; PLAPS was associated in 16 lung sliding. The A/B profile designates anterior-
cases. In 34 cases, an anterior-predominant A pat- predominant B ⫹ lines on one side, predominant A
tern with lung sliding was associated with PLAPS. lines on the other. The C profile designates anterior
Lung sliding was abolished in 28 cases. Three pa- alveolar consolidation(s). PLAPS profile is described
tients had a normal examination. in the Appendix. The normal profile associates the A
profile without PLAPS (regardless of posterior A or
Ultrasound Accuracy B lines) [online document 1].
We retained characteristic combinations of signs
Ultrasound Accuracy Rates
that produced specificities ⬎ 90% (Tables 3, 4). We
suggest a practical nomenclature that avoids repeti- For pulmonary edema, the B profile had 95%
tive descriptions (Fig 6). The A profile designates specificity and 97% sensitivity. For COPD and
anterior predominant bilateral A lines associated asthma (considered together for purposes of simplic-
with lung sliding (with possible focalized B lines). ity), the normal profile had a 97% specificity and a
Table 4 —Accuracy of the Ultrasound Profiles*
Positive Predictive Negative Predictive
Disease Ultrasound Signs Used Sensitivity, % Specificity, % Value, % Value, %
Cardiogenic pulmonary Diffuse bilateral anterior B⫹ lines 97 (62/64) 95 (187/196) 87 (62/71) 99 (187/189)
edema associated with lung sliding (B profile)
COPD or asthma Predominant anterior A lines without 89 (74/83) 97 (172/177) 93 (74/79) 95 (172/181)
PLAPS and with lung sliding (normal
profile), or with absent lung sliding
without lung point
Pulmonary embolism Predominant anterior bilateral A lines 81 (17/21) 99 (238/239) 94 (17/18) 98 (238/242)
plus venous thrombosis
Pneumothorax Absent anterior lung sliding, absent 88 (8/9) 100 (251/251) 100 (8/8) 99 (251/252)
anterior B lines and present lung point
Pneumonia Diffuse bilateral anterior B⫹ lines 11 (9/83) 100 (177/177) 100 (9/9) 70 (177/251)
associated with abolished lung sliding
(B’ profile)
Predominant anterior B⫹ lines on one 14.5 (12/83) 100 (177/177) 100 (12/12) 71.5 (177/248)
side, predominant anterior A lines on
the other (A/B profile)
Anterior alveolar consolidation (C profile) 21.5 (18/83) 99 (175/177) 90 (18/20) 73 (175/240)
A profile plus PLAPS 42 (35/83) 96 (170/177) 83 (35/42) 78 (170/218)
A profile plus PLAPS, B’, A/B or C profile 89 (74/83) 94 (167/177) 88 (74/84) 95 (167/176)
*Data in parenthesis indicate No. of patients (total).
www.chestjournal.org CHEST / 134 / 1 / JULY, 2008 121
Downloaded from chestjournal.chestpubs.org at Borland Medical Library on June 28, 2012
© 2008 American College of Chest Physicians
Figure 6. Ultrasound profiles. Left panel: The A profile is defined as predominant A lines plus lung
sliding at the anterior surface in supine or half-sitting patients (stage 1/1⬘). This profile suggests COPD,
embolism, and some posterior pneumonia. Pulmonary edema is nearly ruled out. Middle: The B profile
is defined as predominant B ⫹ lines in stage 1. This profile suggests cardiogenic pulmonary edema, and
nearly rules out COPD, pulmonary embolism, and pneumothorax. Right panel: an A/B ⫹ profile,
massive B lines at the left lung, A lines at the right lung. This profile is usually associated with
pneumonia.
89% sensitivity. For pulmonary embolism, the A and normal lungs25; roughly 0.95 in interstitial syn-
profile plus venous thrombosis showed 99% speci- drome24; near zero in alveolar consolidation; and
ficity and 81% sensitivity. For pneumothorax, absent zero in pleural effusion (online document 2).
anterior lung sliding, anterior A lines, and a positive COPD and asthma are bronchial diseases assumed
search for lung point yielded 100% specificity and to yield a normal lung surface. This explains the
88% sensitivity. For pneumonia, specificity and sen- ability of ultrasound to distinguish these entities
sitivity were, respectively, 100% and 11% for the B’ from pulmonary edema.26
profile, 100% and 14% for the A/B profile, 99% and In pulmonary edema, the transudate under pressure
11% for the C profile, and 96% and 42% for the A is pushed along interlobular septa against gravity, up to
profile plus PLAPS. These four profiles indicated the anterior wall, explaining the quasiconstant ante-
pneumonia with 94% specificity and 89% sensitivity. rior, symmetric interstitial patterns (indicating an-
For all patients, lung ultrasound yielded correct terior Kerley lines). Edema of interlobular septa is
diagnoses in 90.5% of cases. constant and early.27,28 The B profile (with or with-
out PLAPS due to gravitational filling of dependent
Discussion alveoli) characterizes pulmonary edema with high
accuracy. Posterior interstitial syndrome was not
Briefly, the B profile (anterior interstitial syndrome sought, since gravitational interstitial changes are phys-
with lung sliding) indicated pulmonary edema. The B’ iologic.24 Pulmonary edema produces transsudate,
profile (lung sliding abolished) indicated pneumonia. which is not supposed to generate inflammatory adher-
The A/B profile (asymmetric anterior interstitial syn- ences (a factor that may hinder lung sliding, see below).
drome) and the C profile (anterior consolidation) indi- Pulmonary embolism does not yield interstitial
cated pneumonia, as did the A profile plus PLAPS. The change. A normal anterior lung surface was usually
A profile plus venous thrombosis indicated pulmonary seen, as previously reported.29 None of 92 patients
embolism. A normal profile indicated COPD/asthma. with anterior interstitial patterns had pulmonary
These results correspond to physiopathologic pat- embolism. The positive predictive value of deep
terns, particularly echoed by ultrasound artifacts, venous thrombosis was 89%, but 94% if associated
that have been in clinical use since 1994.23 The with the A profile, suggesting that the search for
pleural line is superficial. Most acute disorders reach venous thrombosis should be associated with lung
it: acute interstitial changes involve deep as well as analysis (Table 2). Pneumothorax features have been
subpleural areas16,24; most (98.5%) cases of acute extensively described.14,15,30
alveolar consolidation abut the pleura21; pneumotho- Pneumonia yields numerous signs. The frequent
rax and pleural effusions always abut the wall.14 The abolition of lung sliding (B’ profile) is explainable by
high acoustic impedance gradient between air and inflammatory adherences due to exudate.31 Abol-
fluid generates artifacts. Air stops ultrasounds, and ished lung sliding again shows low specificity for
fluid facilitates their transmission. The air-fluid ratio pneumothorax (22% positive predictive value here).
is 1 in pneumothorax; roughly 0.98 in asthma, COPD, Pneumonia can be found in a wide variety of loca-
122 Original Research
Downloaded from chestjournal.chestpubs.org at Borland Medical Library on June 28, 2012
© 2008 American College of Chest Physicians
tions, which explains the asymmetric patterns (AB Clinical Implications
profile), anterior consolidations (C profile), or lack of
anterior interstitial patterns (A profile). Note that Using lung ultrasound saves time and decreases
among seven patients initiating ARDS from pneu- the need for CT, whose drawbacks include delayed-
monia, only one had the B profile. Briefly, ultra- care implementation, irradiation,32–34 cost (therefore
sound highlighted distinctions between pneumonia available only in resource-rich countries), and the re-
and pulmonary edema. If confirmed by further data, quired supine position. Lung ultrasound is nearly
this may provide a potential means of differentiating equivalent to CT in detecting most disorders,5 can be
hemodynamic from permeability-related pulmonary repeated at will, and provides additional information.35
edema. Online document 1 shows the number of erroneous
initial diagnoses using conventional tools. One fourth of
the patients in the first 2 h had erroneous or uncertain
Suggested Algorithm
initial diagnoses. Many more received inappropriate
Anterior lung sliding is checked first. Its presence therapy.
discounts pneumothorax. Anterior B lines are sought. Lung ultrasound generates standardized, repro-
The B profile suggests pulmonary edema. The B’, A/B, ducible patterns, explaining the high interobserver
and C profiles suggest pneumonia. The A profile agreement.5,11,21 Feasibility is high. Lung ultrasound
prompts a search for venous thrombosis. If present, may appear complex at first sight but simply requires
pulmonary embolism is considered. If absent, PLAPS is a change in thinking.36 Once the process has been
sought. Its presence (A profile plus PLAPS) suggests learned, a step-by-step use will make it routine.37– 44
pneumonia; its absence (normal profile) suggests
Limitations
COPD/asthma (Fig 7).
This algorithm, using ultrasound alone, would have The operators in this study have several years of
retrospectively given an accurate diagnosis in 90.5% of experience. They were not blinded to the patient’s
cases. Its routine integration into the clinical approach clinical presentation, yet ultrasound profiles were
would give even better results. This algorithm was established based on objective signs.
called Bedside Lung Ultrasound in Emergency—the Among the erroneous results (9.5%), some re-
BLUE protocol. When your patient is blue, promptly sulted from limitations of this simplified ultrasound
perform a BLUE protocol. The absence of echocardi- approach: problems distinguishing pulmonary edema
ography in this algorithm stems from the fact that, even and interstitial pneumonia, or embolism without
if yielding data of primary importance, it gives indirect thrombosis. Others can be explained by possible
arguments, whereas lung ultrasound provides a direct flaws in the reference tests: “decompensated COPD”
approach to acute respiratory failure. In practice, a associated with the B profile or PLAPS, or “pulmo-
cardiac analysis completes our approach. nary edema” without the B profile.
Figure 7. A decision tree utilizing lung ultrasonography to guide diagnosis of severe dyspnea.
www.chestjournal.org CHEST / 134 / 1 / JULY, 2008 123
Downloaded from chestjournal.chestpubs.org at Borland Medical Library on June 28, 2012
© 2008 American College of Chest Physicians
As regards the excluded patients, among rare A/B profile represents anterior-predominant B ⫹ lines at one side
causes of dyspnea, massive pleural effusion was not a and predominant A lines at the other. C profile represents
anterior alveolar consolidation(s). PLAPS represents posterior
diagnostic problem. Chronic interstitial diseases pro-
and/or lateral alveolar and/or pleural syndrome. All these defini-
duce B lines; the solution deserves a subtle approach tions are based on the patient being supine or semirecumbent.
that cannot be discussed herein. Among undefined
official diagnosis, note that all patients had one ACKNOWLEDGMENT: So many people surrounded and helped
characteristic ultrasound profile. Among patients this project, directly or not, that only a collective but warm thanks
will be made in this space. Special thanks to François Jardin, who
with several official diagnoses, their inclusion made this work possible.
would require an accurate way to determine the
respective role of each mechanism involved in
respiratory distress.
References
The choice of the material can be decisive. Cumber-
some echocardiographic units with cardiac probes usu- 1 Wasserman K. Dyspnea on exertion: is it the heart or the
lungs? J Am Med Assoc 1982; 248:2039 –2043
ally have insufficient resolution for the lung. Recent 2 Aronchick J, Epstein D, Gefter WB, et al. Evaluation of the
ultracompact technologies (not a mandatory require- chest radiograph in the emergency department patient.
ment in hospital settings), if technologically designed Emerg Med Clin N Am 1985; 3:491–501
for cardiac investigations, with no consideration for 3 Ray P, Birolleau S, Lefort Y, et al. Acute respiratory failure in
the lung, will not solve this problem. Both systems the elderly: etiology, emergency diagnosis and prognosis. Crit
Care 2006; 10:R82
usually present additional drawbacks: cost, switch-on 4 Greenbaum DM, Marschall KE. The value of routine daily
time, keyboard design that prevents rapid disinfec- chest X-rays in intubated patients in the medical intensive
tion, and modes that seek to remove artifacts. The care unit. Crit Care Med 1982; 10:29 –30
choice of the probe is critical. Vascular probes 5 Lichtenstein D, Goldstein G, Mourgeon E, et al. Compara-
usually prevent deep analysis and artifact recogni- tive diagnostic performances of auscultation, chest radiogra-
phy and lung ultrasonography in acute respiratory distress
tion. Abdominal probes have inappropriate ergo- syndrome. Anesthesiology 2004; 100:9 –15
nomics but are perhaps the least problematic in 6 Dénier A. Les ultrasons, leur application au diagnostic. Presse
terms of resolution. The authors use a low-cost, 31-cm Méd 1946; 22:307–308
large, hybrid machine with a compact design and flat 7 Weinberger SE, Drazen JM. Diagnostic procedures in respi-
keyboard, available since 1992 and still being manufac- ratory diseases. In: Harrison’s principles of internal medicine.
15th ed. New York, NY: McGraw-Hill, 2005; 1505–1508
tured, without Doppler.45,46 Their microconvex probe, 8 Lichtenstein D. Lung ultrasound in the critically ill. In: 2004
the optimal type of probe for the lungs, is also ideal for yearbook of intensive care and emergency medicine. Berlin,
emergency whole-body analysis.22 Germany: Springer-Verlag, 2004; 625– 644
9 Jardin F, Dubourg O. L’exploration échocardiographique en
médecine d’urgence. Paris, France: Masson, 1986
10 Lichtenstein D, Axler O. Intensive use of general ultrasound
Conclusions in the intensive care unit: a prospective study of 150 consec-
utive patients. Intensive Care Med 1993; 19:353–355
Lung ultrasound immediately provided diagnosis of 11 Lichtenstein D, Mezière G. Training in general ultrasound by
acute respiratory failure in 90.5% of cases. It can there- the intensivist [abstract]. Réan Urg 1998; 7(suppl):108s
fore be added to the armamentarium of critical care.47 12 Irwin RS, Rippe JM. Intensive care medicine, 6th ed. Phila-
The additional value of saving time should provide delphia, PA: Lippincott Williams & Wilkins, 2008; 491– 496
13 Lichtenstein D, Mezière G. Ultrasound diagnosis of an acute
prompter relief for these severely dyspneic patients. dyspnea [abstract]. Crit Care 2003; 7(suppl):S93
14 Lichtenstein D, Mezière G, Lascols N, et al. Ultrasound
diagnosis of occult pneumothorax. Crit Care Med 2005;
Appendix 33:1231–1238
15 Lichtenstein D, Menu Y. A bedside ultrasound sign ruling out
pneumothorax in the critically ill: lung sliding. Chest 1995;
Lung Artifacts Nomenclature 108:1345–1348
16 Lichtenstein D, Mezière G, Biderman P, et al. The comet-tail
A lines indicate horizontal repetitive artifacts originating from the artifact, an ultrasound sign of alveolar-interstitial syndrome.
pleural line. B lines indicate vertical, comet-tail artifacts originat- Am J Respir Crit Care Med 1997; 156:1640 –1646
ing from the pleural line, long, hyperechoic, well-defined, dy- 17 Lichtenstein D, Mezière G, Biderman P, et al. The lung
namic, erasing A lines. point: an ultrasound sign specific to pneumothorax. Intensive
Care Med 2000; 26:1434 –1440
Ultrasound Profiles 18 Joyner CR, Herman RJ, Reid JM. Reflected ultrasound in the
detection and localisation of pleural effusion. J Am Med
A profile represents anterior-predominant bilateral A lines asso- Assoc 1967; 200:399 – 402
ciated with lung sliding. A’ profile represents A profile with 19 Lichtenstein D, Hulot JS, Rabiller A, et al. Feasibility and
abolished lung sliding and without lung point. B profile repre- safety of ultrasound-aided thoracentesis in mechanically ven-
sents anterior-predominant bilateral B lines associated with lung tilated patients. Intensive Care Med 1999; 25:955–958
sliding. B’ profile represents B profile with abolished lung sliding. 20 Weinberg B, Diakoumakis EE, Kass EG, et al. The air
124 Original Research
Downloaded from chestjournal.chestpubs.org at Borland Medical Library on June 28, 2012
© 2008 American College of Chest Physicians
bronchogram: sonographic demonstration. AJR Am J Roent- 34 Brenner DJ, Hall EJ. Computed tomography: an increasing
genol 1986; 147:593–595 source of radiation exposure. N Engl J Med 2007; 357:2277–
21 Lichtenstein D, Lascols N, Mezière G, et al. Ultrasound 2284
diagnosis of alveolar consolidation in the critically ill. Inten- 35 Lichtenstein D, Peyrouset O. Lung ultrasound superior to
sive Care Med 2004; 30:276 –281 CT? The example of a CT-occult necrotizing pneumonia.
22 Lichtenstein D. General ultrasound in the critically ill, 2nd Intensive Care Med 2006; 32:334 –335
ed. Heidelberg, Germany: Springer-Verlag, 2005; 70 –95 36 Neri L, Storti E, Lichtenstein D. Toward an ultrasound
23 Lichtenstein D. Ultrasound diagnosis of pulmonary edema. curriculum for critical care medicine. Crit Care Med 2007;
Rev Im Med 1994; 6:561–562 35(suppl):S290 –S304
24 Rémy-Jardin M, Rémy J. Dème interstitiel. In: Rémy-Jardin 37 Bitschnau R, Mathis G. Chest ultrasound in the diagnosis of
M, Rémy J, eds. Imagerie nouvelle de la pathologie thora- acute pulmonary embolism. Radiology 1999; 211:290
cique quotidienne. Paris, France: Springer-Verlag, 1995; 38 Maury E, Guglielminotti J, Alzieu M, et al. Ultrasonic
137–143 examination: an alternative to chest radiography after central
25 Kurt H, Albertine, Williams MC, et al. Anatomy and devel- venous catheter insertion? Am J Respir Crit Care Med 2001;
opment of the respiratory tract. In: Murray JF, Nadel JA, eds. 164:403– 405
Textbook of respiratory medicine, 4th ed. Philadelphia, PA: 39 Rowan KR, Kirkpatrick AW, Liu D, et al. Traumatic pneu-
Elsevier Saunders, 2005; 4 –5 mothorax: detection with thoracic US; correlation with chest
26 Lichtenstein D, Mezière G. A lung ultrasound sign allowing radiography and CT. Radiology 2002; 225:210 –214
bedside distinction between pulmonary edema and COPD: the 40 Reissig A, Kroegel C. Transthoracic sonography of diffuse
comet-tail artifact. Intensive Care Med 1998; 24:1331–1334 parenchymal lung disease: the role of comet tail artifacts.
27 Staub NC. Pulmonary edema. Physiol Rev 1974; 54:678 – 811 J Ultrasound Med 2003; 22:173–180
28 Safran D, Journois D. Circulation pulmonaire. In: Samii K, 41 Mayo PH, Goltz HR, Tafreshi M, et al. Safety of ultrasound-
ed. Anesthésie réanimation chirurgicale, 2nd ed. Paris, guided thoracentesis in patients receiving mechanical venti-
France: Flammarion, 1995; 31–38 lation. Chest 2004; 125:1059 –1062
29 Lichtenstein D, Loubières Y. Lung ultrasonography in pul- 42 Soldati G, Testa A, Silva FR, et al. Chest ultrasonography in
monary embolism [letter]. Chest 2003; 123:2154 lung contusion. Chest 2006; 130:533–538
30 Lichtenstein D, Mezière G, Biderman P, et al. The comet-tail 43 Volpicelli G, Mussa A, Garofalo G, et al. Bedside lung
artifact, an ultrasound sign ruling out pneumothorax. Inten- ultrasound in the assessment of alveolar-interstitial syndrome.
sive Care Med 1999; 25:383–388 Am J Emerg Med 2006; 24:689 – 696
31 Laënnec RTH. Traité de l’auscultation médiate, ou traité du 44 Fagenholz PJ, Gutman JA, Murray AF, et al. Chest ultra-
diagnostic des maladies des poumons et du coeur. Paris, sonography for the diagnosis and monitoring of high-altitude
France: J.A. Brosson & J.S. Chaudé, 1819; New York, NY: pulmonary edema. Chest 2007; 131:1013–1018
Hafner, 1962; 455– 456 45 Cronan JJ. Venous thromboembolic disease: the role of
32 Brenner DJ, Elliston CD, Hall EJ, et al. Estimated risks of ultrasound, state of the art. Radiology 1993; 186:619 – 630
radiation-induced fatal cancer from pediatric CT. AJR Am J 46 Lichtenstein D, Jardin F. Diagnosis of internal jugular vein
Roentgenol 2001; 176:289 –296 thrombosis. Intensive Care Med 1997; 23:1188 –1189
33 Berrington de Gonzales A, Darby S. Risk of cancer from 47 van der Werf TS, Zijlstra JG. Ultrasound of the lung: just
diagnostic X-rays. Lancet 2004; 363:345–351 imagine. Intensive Care Med 2004; 30:183–184
www.chestjournal.org CHEST / 134 / 1 / JULY, 2008 125
Downloaded from chestjournal.chestpubs.org at Borland Medical Library on June 28, 2012
© 2008 American College of Chest Physicians
Relevance of Lung Ultrasound in the Diagnosis of Acute Respiratory
Failure * : The BLUE Protocol
Daniel A. Lichtenstein and Gilbert A. Mezière
Chest 2008;134; 117-125; Prepublished online April 10, 2008;
DOI 10.1378/chest.07-2800
This information is current as of June 28, 2012
Supplementary Material
View e-supplements related to this article at:
http://chestjournal.chestpubs.org/content/suppl/2009/03/19/chest.07-2800.DC1.html
Updated Information & Services
Updated Information and services can be found at:
http://chestjournal.chestpubs.org/content/134/1/117.full.html
References
This article cites 38 articles, 14 of which can be accessed free at:
http://chestjournal.chestpubs.org/content/134/1/117.full.html#ref-list-1
Cited Bys
This article has been cited by 19 HighWire-hosted articles:
http://chestjournal.chestpubs.org/content/134/1/117.full.html#related-urls
Permissions & Licensing
Information about reproducing this article in parts (figures, tables) or in its entirety can be
found online at:
http://www.chestpubs.org/site/misc/reprints.xhtml
Reprints
Information about ordering reprints can be found online:
http://www.chestpubs.org/site/misc/reprints.xhtml
Citation Alerts
Receive free e-mail alerts when new articles cite this article. To sign up, select the
"Services" link to the right of the online article.
Images in PowerPoint format
Figures that appear in CHEST articles can be downloaded for teaching purposes in
PowerPoint slide format. See any online figure for directions.
Downloaded from chestjournal.chestpubs.org at Borland Medical Library on June 28, 2012
© 2008 American College of Chest Physicians
You might also like
- Full download Drugs in anaesthesia and intensive care 5th Edition Scarth pdf docx100% (1)Full download Drugs in anaesthesia and intensive care 5th Edition Scarth pdf docx65 pages
- Ebooks File ExpertDDx: Chest 2nd Edition. Edition Brett W. Carter All Chapters100% (4)Ebooks File ExpertDDx: Chest 2nd Edition. Edition Brett W. Carter All Chapters29 pages
- Breath Sounds - From Basic Science To Clinical Practice 2018100% (3)Breath Sounds - From Basic Science To Clinical Practice 2018314 pages
- Lebanon Exams Mrcs Part A Sample QuestionsNo ratings yetLebanon Exams Mrcs Part A Sample Questions6 pages
- Evolution in Screening For Down Syndrome: Reviews100% (1)Evolution in Screening For Down Syndrome: Reviews7 pages
- @MBS MedicalBooksStore 2020 Flexible Bronchoscopy 4th Edition100% (2)@MBS MedicalBooksStore 2020 Flexible Bronchoscopy 4th Edition479 pages
- RLE Module 2M - Chest Physiotherapy, Postural Drainage, Nebulization, Chest Tube Drainage Systems, Blood TransfusionNo ratings yetRLE Module 2M - Chest Physiotherapy, Postural Drainage, Nebulization, Chest Tube Drainage Systems, Blood Transfusion57 pages
- NCLEX Exam: Respiratory System Disorders (60 Questions) : Correct100% (3)NCLEX Exam: Respiratory System Disorders (60 Questions) : Correct41 pages
- Diagnostic Medical Sonography - Abdomen and Superficial Structures (Diagnostic Medical Sonography Series), 3E (2012) (PDF) (UnitedVRG)No ratings yetDiagnostic Medical Sonography - Abdomen and Superficial Structures (Diagnostic Medical Sonography Series), 3E (2012) (PDF) (UnitedVRG)859 pages
- Lung Ultrasound in The Critically Ill - The BLUE Protocol, Lichtenstein, 2016No ratings yetLung Ultrasound in The Critically Ill - The BLUE Protocol, Lichtenstein, 2016394 pages
- Computed Tomography of The Lung: Johny A. Verschakelen Walter de WeverNo ratings yetComputed Tomography of The Lung: Johny A. Verschakelen Walter de Wever229 pages
- Foundations of Respiratory Medicine (2018) PDFNo ratings yetFoundations of Respiratory Medicine (2018) PDF375 pages
- Anesthesia for Congenital Heart DiseaseFrom EverandAnesthesia for Congenital Heart DiseaseStephen A. StayerNo ratings yet
- Emergency Point-of-Care UltrasoundFrom EverandEmergency Point-of-Care UltrasoundJames A. ConnollyNo ratings yet
- Handbook of Thoracic Malignancies and Esophageal Related CancerFrom EverandHandbook of Thoracic Malignancies and Esophageal Related CancerNo ratings yet
- The RUSH Exam - Rapid Ultrasound in SHock in The Evaluation of The Critically LLLNo ratings yetThe RUSH Exam - Rapid Ultrasound in SHock in The Evaluation of The Critically LLL28 pages
- Clinical Guide To Sonography: Exercises For Critical Thinking. ISBN 9780323091640, 978-0323091640No ratings yetClinical Guide To Sonography: Exercises For Critical Thinking. ISBN 9780323091640, 978-032309164023 pages
- Applied Technologies in Pulmonary Medicine (PDFDrive)No ratings yetApplied Technologies in Pulmonary Medicine (PDFDrive)271 pages
- Gebhard Mathis - Chest Sonography-Springer (2022)No ratings yetGebhard Mathis - Chest Sonography-Springer (2022)248 pages
- Blue Protocol. Lung Ultrasound in The Critically IllNo ratings yetBlue Protocol. Lung Ultrasound in The Critically Ill12 pages
- Craig Sims, Dana Weber, Chris Johnson - A Guide To Pediatric Anesthesia (2020, Springer International Publishing)No ratings yetCraig Sims, Dana Weber, Chris Johnson - A Guide To Pediatric Anesthesia (2020, Springer International Publishing)535 pages
- Lung Ultrasound Made Easy Step-By-Step Guide100% (2)Lung Ultrasound Made Easy Step-By-Step Guide40 pages
- Pulmonary Sarcoidosis Presenting With Cannonball Pattern Mimicking Lung MetastasesNo ratings yetPulmonary Sarcoidosis Presenting With Cannonball Pattern Mimicking Lung Metastases5 pages
- BLUE-Protocol and FALLS-Protocol: Two Applications of Lung Ultrasound in The Critically IllNo ratings yetBLUE-Protocol and FALLS-Protocol: Two Applications of Lung Ultrasound in The Critically Ill12 pages
- European Society of Cardiology-Esc Guidelines Desk Reference 2011 - Compendi PDFNo ratings yetEuropean Society of Cardiology-Esc Guidelines Desk Reference 2011 - Compendi PDF379 pages
- An Approach To Interpreting Spirometry (Finals) PDFNo ratings yetAn Approach To Interpreting Spirometry (Finals) PDF25 pages
- Novel Approaches To Ultrasonography of The Lung and Pleural Space: Where Are We Now?100% (1)Novel Approaches To Ultrasonography of The Lung and Pleural Space: Where Are We Now?12 pages
- Evidence-Based Obstetric AnesthesiaFrom EverandEvidence-Based Obstetric AnesthesiaStephen H. HalpernNo ratings yet
- 2009, Vol.47, Issues 2, Imaging of Airway Diseases100% (2)2009, Vol.47, Issues 2, Imaging of Airway Diseases154 pages
- Cario Manual de Enfermedad Cardiaca Valvular 2018No ratings yetCario Manual de Enfermedad Cardiaca Valvular 2018653 pages
- Edic Part 2: Thomas Kurian MD, DNB (Respiratory Medicine) Idccm, EdicNo ratings yetEdic Part 2: Thomas Kurian MD, DNB (Respiratory Medicine) Idccm, Edic25 pages
- Thrombectomy Procedures - Percutaneous Mechanical, Vascular Surgical, PharmaceuticalFrom EverandThrombectomy Procedures - Percutaneous Mechanical, Vascular Surgical, PharmaceuticalNo ratings yet
- Lung Ultrasound in Critical Care and Emergency MedicineNo ratings yetLung Ultrasound in Critical Care and Emergency Medicine21 pages
- Full Textbook of Peripheral Vascular Interventions Second Edition Richard R. Heuser Ebook All Chapters100% (18)Full Textbook of Peripheral Vascular Interventions Second Edition Richard R. Heuser Ebook All Chapters84 pages
- Practice Management Guidelines For Management of Hemothorax and Occult PneumothoraxNo ratings yetPractice Management Guidelines For Management of Hemothorax and Occult Pneumothorax9 pages
- (2008) Azfar H Et Al - Spontaneous HemothoraxNo ratings yet(2008) Azfar H Et Al - Spontaneous Hemothorax10 pages
- 10346E Diver Medical Participant Questionnaire 2022-01-17No ratings yet10346E Diver Medical Participant Questionnaire 2022-01-173 pages
- Interpreting Chest X Rays Illustrated with 100 Cases 1st Edition Philip Eng all chapter instant download100% (2)Interpreting Chest X Rays Illustrated with 100 Cases 1st Edition Philip Eng all chapter instant download34 pages
- Maxilofacial Trauma: Presenter: - Wisnu Adiputra (07120080072) - Nofilia Citra Candra (07120090066)No ratings yetMaxilofacial Trauma: Presenter: - Wisnu Adiputra (07120080072) - Nofilia Citra Candra (07120090066)97 pages
- [Ebooks PDF] download ERS Handbook Self Assessment in Respiratory Medicine Sep 1 2012 _ 1849840296 _ European Respiratory Society pdf 1st Edition Konrad E Bloch full chapters100% (14)[Ebooks PDF] download ERS Handbook Self Assessment in Respiratory Medicine Sep 1 2012 _ 1849840296 _ European Respiratory Society pdf 1st Edition Konrad E Bloch full chapters85 pages
- Chapter 9 - Thoracic Injuries Questions: Dr. Achmad Faisal, SPBTKV, Fects, Fiha0% (1)Chapter 9 - Thoracic Injuries Questions: Dr. Achmad Faisal, SPBTKV, Fects, Fiha12 pages
- Remedi KA6 Slides - Client PPT - Remedi IndiaNo ratings yetRemedi KA6 Slides - Client PPT - Remedi India34 pages
- PASSMED MRCP MCQs-RESPIRATORY MEDICINE PDF PDFNo ratings yetPASSMED MRCP MCQs-RESPIRATORY MEDICINE PDF PDF6 pages
- Interventional Radiology: A Manual For Surgeons and RadiologistsNo ratings yetInterventional Radiology: A Manual For Surgeons and Radiologists24 pages
- Craven & Hirnle's Nursing Procedures and Fundamentals OnlineNo ratings yetCraven & Hirnle's Nursing Procedures and Fundamentals Online4 pages
- Pulmonology: The Cells of The Bronchial Epithelium, Leucocytes100% (1)Pulmonology: The Cells of The Bronchial Epithelium, Leucocytes64 pages























































































- Full download Drugs in anaesthesia and intensive care 5th Edition Scarth pdf docxFull download Drugs in anaesthesia and intensive care 5th Edition Scarth pdf docx
- Ebooks File ExpertDDx: Chest 2nd Edition. Edition Brett W. Carter All ChaptersEbooks File ExpertDDx: Chest 2nd Edition. Edition Brett W. Carter All Chapters
- Bedside Ultrasound: Level 1 - Second EditionFrom EverandBedside Ultrasound: Level 1 - Second Edition
- Breath Sounds - From Basic Science To Clinical Practice 2018Breath Sounds - From Basic Science To Clinical Practice 2018
- @MBS MedicalBooksStore 2020 Flexible Bronchoscopy 4th Edition@MBS MedicalBooksStore 2020 Flexible Bronchoscopy 4th Edition
- RLE Module 2M - Chest Physiotherapy, Postural Drainage, Nebulization, Chest Tube Drainage Systems, Blood TransfusionRLE Module 2M - Chest Physiotherapy, Postural Drainage, Nebulization, Chest Tube Drainage Systems, Blood Transfusion
- NCLEX Exam: Respiratory System Disorders (60 Questions) : CorrectNCLEX Exam: Respiratory System Disorders (60 Questions) : Correct
- Diagnostic Medical Sonography - Abdomen and Superficial Structures (Diagnostic Medical Sonography Series), 3E (2012) (PDF) (UnitedVRG)Diagnostic Medical Sonography - Abdomen and Superficial Structures (Diagnostic Medical Sonography Series), 3E (2012) (PDF) (UnitedVRG)
- Lung Ultrasound in The Critically Ill - The BLUE Protocol, Lichtenstein, 2016Lung Ultrasound in The Critically Ill - The BLUE Protocol, Lichtenstein, 2016
- Computed Tomography of The Lung: Johny A. Verschakelen Walter de WeverComputed Tomography of The Lung: Johny A. Verschakelen Walter de Wever
- Handbook of Thoracic Malignancies and Esophageal Related CancerFrom EverandHandbook of Thoracic Malignancies and Esophageal Related Cancer
- The RUSH Exam - Rapid Ultrasound in SHock in The Evaluation of The Critically LLLThe RUSH Exam - Rapid Ultrasound in SHock in The Evaluation of The Critically LLL
- Clinical Guide To Sonography: Exercises For Critical Thinking. ISBN 9780323091640, 978-0323091640Clinical Guide To Sonography: Exercises For Critical Thinking. ISBN 9780323091640, 978-0323091640
- Applied Technologies in Pulmonary Medicine (PDFDrive)Applied Technologies in Pulmonary Medicine (PDFDrive)
- Blue Protocol. Lung Ultrasound in The Critically IllBlue Protocol. Lung Ultrasound in The Critically Ill
- Craig Sims, Dana Weber, Chris Johnson - A Guide To Pediatric Anesthesia (2020, Springer International Publishing)Craig Sims, Dana Weber, Chris Johnson - A Guide To Pediatric Anesthesia (2020, Springer International Publishing)
- Pulmonary Sarcoidosis Presenting With Cannonball Pattern Mimicking Lung MetastasesPulmonary Sarcoidosis Presenting With Cannonball Pattern Mimicking Lung Metastases
- BLUE-Protocol and FALLS-Protocol: Two Applications of Lung Ultrasound in The Critically IllBLUE-Protocol and FALLS-Protocol: Two Applications of Lung Ultrasound in The Critically Ill
- European Society of Cardiology-Esc Guidelines Desk Reference 2011 - Compendi PDFEuropean Society of Cardiology-Esc Guidelines Desk Reference 2011 - Compendi PDF
- An Approach To Interpreting Spirometry (Finals) PDFAn Approach To Interpreting Spirometry (Finals) PDF
- Novel Approaches To Ultrasonography of The Lung and Pleural Space: Where Are We Now?Novel Approaches To Ultrasonography of The Lung and Pleural Space: Where Are We Now?
- 2009, Vol.47, Issues 2, Imaging of Airway Diseases2009, Vol.47, Issues 2, Imaging of Airway Diseases
- Edic Part 2: Thomas Kurian MD, DNB (Respiratory Medicine) Idccm, EdicEdic Part 2: Thomas Kurian MD, DNB (Respiratory Medicine) Idccm, Edic
- Thrombectomy Procedures - Percutaneous Mechanical, Vascular Surgical, PharmaceuticalFrom EverandThrombectomy Procedures - Percutaneous Mechanical, Vascular Surgical, Pharmaceutical
- Lung Ultrasound in Critical Care and Emergency MedicineLung Ultrasound in Critical Care and Emergency Medicine
- Radiological Anatomy Dictionary: Grow Your VocabularyFrom EverandRadiological Anatomy Dictionary: Grow Your Vocabulary
- Full Textbook of Peripheral Vascular Interventions Second Edition Richard R. Heuser Ebook All ChaptersFull Textbook of Peripheral Vascular Interventions Second Edition Richard R. Heuser Ebook All Chapters
- Practice Management Guidelines For Management of Hemothorax and Occult PneumothoraxPractice Management Guidelines For Management of Hemothorax and Occult Pneumothorax
- 10346E Diver Medical Participant Questionnaire 2022-01-1710346E Diver Medical Participant Questionnaire 2022-01-17
- Interpreting Chest X Rays Illustrated with 100 Cases 1st Edition Philip Eng all chapter instant downloadInterpreting Chest X Rays Illustrated with 100 Cases 1st Edition Philip Eng all chapter instant download
- Maxilofacial Trauma: Presenter: - Wisnu Adiputra (07120080072) - Nofilia Citra Candra (07120090066)Maxilofacial Trauma: Presenter: - Wisnu Adiputra (07120080072) - Nofilia Citra Candra (07120090066)
- [Ebooks PDF] download ERS Handbook Self Assessment in Respiratory Medicine Sep 1 2012 _ 1849840296 _ European Respiratory Society pdf 1st Edition Konrad E Bloch full chapters[Ebooks PDF] download ERS Handbook Self Assessment in Respiratory Medicine Sep 1 2012 _ 1849840296 _ European Respiratory Society pdf 1st Edition Konrad E Bloch full chapters
- Chapter 9 - Thoracic Injuries Questions: Dr. Achmad Faisal, SPBTKV, Fects, FihaChapter 9 - Thoracic Injuries Questions: Dr. Achmad Faisal, SPBTKV, Fects, Fiha
- Interventional Radiology: A Manual For Surgeons and RadiologistsInterventional Radiology: A Manual For Surgeons and Radiologists
- Craven & Hirnle's Nursing Procedures and Fundamentals OnlineCraven & Hirnle's Nursing Procedures and Fundamentals Online
- Pulmonology: The Cells of The Bronchial Epithelium, LeucocytesPulmonology: The Cells of The Bronchial Epithelium, Leucocytes