
Hematology 2016
Hematology 2016
Uploaded by
marinaCopyright:
Available Formats
Hematology 2016
Hematology 2016
Uploaded by
marinaOriginal Description:
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Copyright:
Available Formats
Hematology 2016
Hematology 2016
Uploaded by
marinaCopyright:
Available Formats
| WHEN ANTIBODY RESPONSE GOES AWRY |
Warm antibody autoimmune hemolytic anemia
Theodosia A. Kalfa
Division of Hematology, Cancer and Blood Diseases Institute, Cincinnati Children’s Hospital Medical Center,
University of Cincinnati College of Medicine, Cincinnati, OH
Autoimmune hemolytic anemia (AIHA) is a rare and heterogeneous disease that affects 1 to 3/100 000 patients per year.
AIHA caused by warm autoantibodies (w-AIHA), ie, antibodies that react with their antigens on the red blood cell optimally
at 37°C, is the most common type, comprising ~70% to 80% of all adult cases and ~50% of pediatric cases. About half of the
w-AIHA cases are called primary because no specific etiology can be found, whereas the rest are secondary to other
recognizable underlying disorders. This review will focus on the postulated immunopathogenetic mechanisms in idiopathic
and secondary w-AIHA and report on the rare cases of direct antiglobulin test–negative AIHA, which are even more likely to
be fatal because of inherent characteristics of the causative antibodies, as well as because of delays in diagnosis and
initiation of appropriate treatment. Then, the characteristics of w-AIHA associated with genetically defined immune
dysregulation disorders and special considerations on its management will be discussed. Finally, the standard treatment
options and newer therapeutic approaches for this chronic autoimmune blood disorder will be reviewed.
complement fragments are detected on the RBC surface using the
Learning Objectives direct antiglobulin test (DAT). DAT, or direct Coombs test, is typically
• Discuss the immunopathogenesis of autoantibody produc- performed in 2 steps. First, the polyspecific reagent containing both
tion and the mechanisms of antibody-sensitized red blood anti-immunoglobulin G (IgG) and anticomplement is used to agglu-
cell destruction in warm autoimmune hemolytic anemia tinate antibody-coated cells, and then the monospecific reagents anti-
(w-AIHA) IgG and anti-C3d (anti-C3b, anti-C4b, and anti-C4d reagents also
• Understand the reasons DAT may be negative in some cases available) are used individually to detect IgG and complement, re-
of w-AIHA and the implications in diagnosis and management spectively. Binding of anti-C3d alone often indicates bound IgM.4,5
of these cases AIHA is classified into 3 major types based on the optimal temperature
• Recognize the association of w-AIHA with autoimmune in which the autoantibodies bind on the patient’s RBCs in vivo: warm
lymphoproliferative syndrome (ALPS) and other primary immuno- antibody AIHA (w-AIHA), cold agglutinin syndrome (CAS), and
deficiency (PID) syndromes paroxysmal cold hemoglobinuria (PCH). In some unusual cases,
• Review the standard treatment options and newer therapeutic considered as “mixed AIHA,” the laboratory data satisfy the serologic
approaches for w-AIHA criteria of both w-AIHA and CAS.6 The 2 clinical entities of AIHA
that are due to cold-reacting autoantibodies are defined by the im-
Normal red blood cells (RBCs) have an average life span of 115 days.1 munoglobulin isotype against the RBCs: IgM in CAS and IgG in PCH.
Hemolysis is defined as decreased RBC survival and can be caused IgM autoantibodies, typically directed against the I/i system of RBC
because of an inherent abnormality of the cell (intrinsic or intra- antigens, are maximally reactive in the cold (4°C), although they may
corpuscular defect), by extrinsic factors, or by a combination of both. keep a reactivity up to $30°C (wide “thermal amplitude”). The IgM
When hemolysis occurs at a rate that cannot be compensated by in- pentamers fix complement much more readily than IgG, causing
creased RBC production, then the patient presents with hemolytic intravascular hemolysis and to a lesser extent extravascular lysis
anemia. The premature RBC destruction can happen intravascularly or mainly in the liver by macrophages with C3d receptors. Rouleaux
extravascularly in the reticuloendothelial system (mainly adjacent to formation indicating RBC agglutination is frequently noted on the
the macrophages of spleen and liver) and can be episodic/acute or blood smear. PCH is caused by the Donath-Landsteiner IgG antibodies
chronic. Clinical presentation includes pallor, fatigue, jaundice, dark which are usually directed against the P antigen of RBCs. Donath-
urine, splenomegaly, and, in chronic cases, gallstones and cholecystitis. Landsteiner antibodies are biphasic hemolysins: they bind to RBCs
Common laboratory findings are anemia, ie, decreased hemoglobin and fix complement (C1) at cold temperatures, but the complement is
(Hb), reticulocytosis, elevated unconjugated bilirubin and lactate de- then activated at the core temperature of 37°C causing intravascular
hydrogenase, serum aspartate aminotransferase disproportionately RBC lysis. PCH is frequently postinfectious and typically has a good
higher than serum alanine aminotransferase, and decreased haptoglobin. prognosis after remission; however, it can be life threatening on
presentation due to severe and rapidly progressive anemia.3,7
Autoimmune hemolytic anemia (AIHA) is caused by increased RBC
destruction triggered by autoantibodies reacting against RBC antigens AIHA is a rare disease with an incidence of 1 to 3 per 100 000 people
with or without complement activation.2,3 The autoantibodies and/or per year.8,9 w-AIHA is the most common type of autoimmune
Conflict-of-interest disclosure: The author declares no competing financial interests.
Off-label drug use: None disclosed.
690 American Society of Hematology
bound to the erythrocytes, complement (C1q) is bound and gets
activated toward C3b. C3b-opsonized RBCs are next phagocytosed
by liver macrophages that carry C3b receptors (Figure 2).3,12,14
This review will describe the postulated pathogenetic mechanisms
in idiopathic and secondary w-AIHA, report on the rare cases of
DAT-negative AIHA and on cases associated with genetically de-
fined immune dysregulation, and discuss standard treatments and
new therapeutic approaches.
Pathogenetic mechanisms in idiopathic and
secondary w-AIHA
Autoantibodies, the complement system, phagocytes, cytotoxic
CD81 T cells and NK cells performing ADCC, B and T lymphocytes
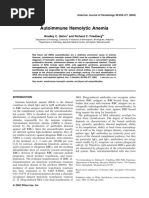
Figure 1. Blood smear of a patient with w-AIHA on presentation. including the CD41 T regulatory (Treg) cells, and cytokines are all
Polychromasia reflecting reticulocytosis, many microspherocytes (few key players in the pathogenesis of w-AIHA. Several mechanisms
pointed by arrowheads), and a nucleated red blood cell (arrow), indicating leading to breach of normal interactions between these immune
stress erythropoiesis, are noted (Wright-Giemsa stain). Bar represents 14 mm. system components have been proposed and are being actively
investigated as responsible for the breakdown of immunologic
tolerance that allows development of w-AIHA.3,6 An excellent recent
hemolytic anemia, comprising ~70% to 80% of all adult cases and review by Barcellini3 describes in detail the working hypotheses and
~50% of the pediatric cases.9 About half of the w-AIHA cases are relevant data on these mechanisms.
called primary because no specific etiology can be found, whereas the
rest are recognized as secondary to lymphoproliferative syndromes; Molecular mimicry of foreign antigens from viruses or other ex-
malignant diseases including chronic lymphoblastic leukemia (CLL), ogenous infectious and noninfectious agents, eg, drugs, that cross-
non-Hodgkin’s lymphoma, and solid tumors; rheumatologic diseases, react with RBC self-antigens, most frequently Rh proteins, and
especially systemic lupus erythematosus; infections (mostly viral)10,11; occasionally glycophorins and band 3, may overcome self-
drugs; frequent cephalosporins and piperacillin; or a previous trans- tolerance and trigger AIHA. Additionally, polyclonal activation
fusion or transplantation.3 The category of primary or idiopathic (ie, of B lymphocytes by viruses may trigger the emergence of “for-
of unknown cause) w-AIHA is likely to keep shrinking in the near bidden clones,” occasionally along with a congenital or acquired
future as we increasingly recognize more monogenic and polygenic dis- lymphoproliferative disorder.
orders of immune dysregulation, which frequently have an autoimmune
cytopenia as their first manifestation. The CD41 T-helper cell subsets, Th1, Th2, Th17, and the Tregs
control the humoral immune system and have a critical role in
In w-AIHA, the autoantibodies react optimally with the RBCs at maintaining or losing self-tolerance. Elevated frequency of Th17
37°C. Typically, no autoantibody specificity can be identified; the cells producing increased interleukin-17 (IL-17) were found to
autoantibodies are polyclonal and react with all RBCs tested (pan- correlate with disease activity in patients with AIHA.15 CD41
reactive), even when w-AIHA complicates a clonal B-cell lym- CD251 Treg cells express high levels of the IL-2 receptor CD25 and
phoproliferative disorder like CLL. Microspherocytes are frequently secrete transforming growth factor-b and IL-10. Naturally occurring
noted on the blood smear (Figure 1). Polychromasia, indicating Tregs contribute to immunologic self-tolerance by suppressing
reticulocytosis, is typical, although the reticulocyte count may not potentially autoreactive T cells. Treg cells were indeed found re-
be elevated early in the course, and occasionally relative retic- duced in patients with AIHA.16 Imbalance between Th1 and Th2
ulocytopenia may be continuously observed as a result of autoan- cells and the cytokines they secrete may also play a role. Th1
tibody sensitization and destruction of late erythroid precursors. secrete IL-2, IL-12, interferon-g, and tumor necrosis factor-b and
Complement activation on the RBC surface may lead to the for- promote cell-mediated immunity, whereas Th2 cells secrete IL-4,
mation of membrane attack complex (C5b9), causing RBC lysis in IL-5, IL-6, IL-10, and IL-13 and promote humoral responses.
the circulation, although this is more typical for antibodies that avidly Although the data on increased and decreased cytokine levels in
bind complement like the IgM pentamers in CAS. Intravascular patients with AIHA may be somewhat conflicting, they favor that
complement-mediated cell lysis does not play a significant role a reduced Th1 and a prominent Th2 profile promote the patho-
in most patients with w-AIHA, implicating that terminal comple- genesis of AIHA.3,6
ment inhibitors would be clinically irrelevant,12 except maybe for
those atypical cases with significant warm antibody-complement– Regarding unique mechanisms in secondary w-AIHA, a decrease
mediated intravascular hemolysis.13 Erythrocytes coated by warm- of the CR1 complement receptor (CD35) and CD55 (decay-
reacting IgG are bound by spleen macrophages, which carry Fcg accelerating factor) or CD59 was found on RBCs and CD31
receptors for the IgG heavy chain, and they are either phagocytosed lymphocytes in systemic lupus erythematosus–associated AIHA,
or have part of their membrane removed, in which case they form whereas after bone marrow transplantation, an activation of host
microsperocytes subject to further destruction during their next self-reactive B cells by allo-reactive donor T cells was seen in
passage through the spleen. Antibody-dependent cell-mediated cy- chronic graft-versus-host disease.6
totoxicity (ADCC), mediated by cytotoxic CD81 T cells and natural
killer (NK) cells also with Fc receptors in the spleen, also contributes Further investigation and understanding of the immunopathogenetic
to RBC destruction/extravascular hemolysis. When either a high mechanisms that lead to AIHA will provide insights for development
concentration of IgG or IgG with high affinity to complement is of more effective and less toxic, targeted therapeutic options.
Hematology 2016 691
Figure 2. Mechanisms of antibody-sensitized RBC destruction in w-AIHA. Erythrocytes coated by warm-reacting IgG are bound by spleen macrophages
carrying Fcg receptors for the IgG heavy chain, and they are either phagocytosed or have part of their membrane removed, in which case
they form microspherocytes subject to further destruction during their next passage through the spleen. ADCC, mediated by cytotoxic CD81
T cells (Tc) and NK cells, is also contributing to extravascular hemolysis preferentially in the spleen and lymphoid organs. When either a high
concentration of IgG or IgG with high affinity to complement is bound to the erythrocytes, complement (C1q) is bound and gets activated toward
C3b. C3b-opsonized RBCs are next phagocytosed by liver macrophages that carry C3b receptors.
DAT-negative AIHA have been now developed and used by reference laboratories; they are
In 1957, Evans and Weiser reported on the serology of immune he- calibrated so that the fluorescently labeled anti-human IgG on red cells is
molytic disease, describing 41 cases of autoimmune hemolytic anemia, detected at a sensitivity greater than that of the commercial DAT reagent,
4 of which had negative direct and indirect Coombs.17 In 1 case, RBC decreasing the frequency of a false-negative antiglobulin test.18,22,23
agglutination in the DAT was achieved only after preparing the anti-
globulin serum by injecting the patient’s own serum into rabbits. In the RBC autoantibodies may have low affinity and therefore are re-
other 3 cases, the 2 associated with infectious mononucleosis, auto- moved easily from the red cell surface during preparative washings
antibodies or isoantibodies, could not be demonstrated but transfused of the cells at room temperature, to perform direct Coombs. Cold
RBCs in these patients had a severely decreased survival, indicating that washing with isotonic or with low ionic strength saline at 4°C using
a factor extrinsic to the patients’ red cells was responsible for their refrigerated centrifuges can prevent the antibody loss from the RBC
destruction. Since then, numerous case series have studied anemia with surface, improving the sensitivity of the commercial DAT assay.18,24
clinical characteristics of w-AIHA but with negative DAT. Based on
such publications, the incidence of DAT-negative w-AIHA has been w-AIHA may be rarely due to sensitization of RBCs with IgA25,26 or
estimated at 3% to 11% of all cases, depending, at least in part, on the a warm-reacting, monomeric IgM alone instead of IgG, without
potency of the direct antiglobulin reagent used for the DAT.18 complement fixation,27 in which cases most commercial DAT re-
agents, containing only anti-IgG against the g heavy chain portion of
There are several inherent characteristics of the RBC autoantibodies the IgG molecule and anti-C3, are not detecting the antibodies.5
causing DAT-negative w-AIHA, and thankfully there are now al-
ternative methods to prove their existence, which are easier and faster Reference laboratories are offering enhanced DAT assays (orderable
than immunizing a rabbit with the patient’s serum. frequently as super-Coombs or micro-Coombs), using an extensive
list of methods reviewed in detail by Segel and Lichtman,18 to
Anti-RBC IgG may bind to the erythrocytes at relatively low levels confirm the immune basis of a hemolytic anemia with history and
causing hemolysis but being below the threshold of detection for the clinical and hematologic findings compatible with w-AIHA but with
commonly used DAT reagents. Kamesaki et al studied samples from negative routine DAT. Of note, in keeping with the observations that
154 patients with DAT-negative AIHA and from 62 patients with DAT- the intensity of DAT reaction does not correlate with the degree of
positive disease by immunoradiometric assay and determined that the hemolysis and severity of the disease, DAT-negative w-AIHA can be
first group had a mean red cell IgG density approximately an order of mild or severe and life threatening. Similarly to the DAT-positive
magnitude less (179 IgG molecules/red cell) than in DAT-positive disease, DAT-negative w-AIHA can also be primary or secondary,
patients (1397 IgG molecules/red cell).19 Normal RBCs from healthy may respond to steroids or splenectomy or may not, and requires the
control subjects had been previously determined to have a low level of same management approach.28-30
IgG adsorbed on their membrane, calculated at 33 6 13 molecules/cell
as detected by immunoradiometric assay20 or ,35 molecules/cell as AIHA associated with genetically defined immune
detected by complement-fixing, antibody consumption test.21 At the dysregulation
same time, the commercial DAT reagent and assay could not identify wAIHA presenting either simultaneously or sequentially with
positivity below ~500 molecules of IgG/cell.21 Flow cytometry assays thrombocytopenia is known as Evans syndrome.31 In fact, when
692 American Society of Hematology
Robert Evans and his colleagues described in 1951 the combination by a known gene mutation or one yet to be determined.35,36,39 It is
of primary thrombocytopenic purpura (of unknown origin at the time important to note that splenectomy should be a last resort in the
pathogenesis) with acquired hemolytic anemia (which was known to management of cytopenias in ALPS because overwhelming sepsis
be due to red cell sensitization with antibodies) gave, for the first following splenectomy is the most frequent cause of death in these
time, evidence that the primary (or idiopathic) thrombocytopenic patients, even more frequent than malignancies.36,40 The defective
purpura is of autoimmune etiology similar to the concurrent he- B-cell function in ALPS was found to be associated with poor anti-
molytic anemia.31 This combination came later to be known as Evans polysacharide IgM antibody production,41 predisposing the patients
syndrome. Over time, the definition of the syndrome has expanded to a higher risk of life-threatening pneumococcal sepsis after sple-
to cover the combination of any 2 or 3 autoimmune cytopenias and nectomy, up to 41% in a cohort of splenectomized ALPS patients.36
is increasingly recognized to be a manifestation of common variable Rituximab also demonstrated increased toxicity in ALPS patients
immunodeficiency with autoantibody formation due to defective causing prolonged and severe hypogammaglobulinemia up to life-
B-cell selection and maturation, or of autoimmune lymphoproli- long IVIG dependency.35,36 Mycophenolate mofetil (MMF) and
ferative syndrome (ALPS), a classic primary immunodeficiency sirolimus are currently the agents of choice for second-line treatment
(PID), or of other novel immune dysregulation syndromes.32-34 of ALPS-related cytopenias, with sirolimus having a beneficial effect
Therefore, the diagnosis of Evans syndrome should trigger a ba- even to the spleen and lymph node size.36,39
sic immunologic workup including screening for common variable
immunodeficiency and ALPS. In fact, childhood AIHA is frequently Standard treatment options and new therapeutic
secondary to an immunologic disease. In a series of 265 children approaches
with AIHA (French National Observational Study), the diagnosis The rarity and heterogeneity of w-AIHA essentially preclude ran-
of AIHA followed a diagnosis of another autoimmune disease, in- domized prospective phase 3 trials to provide evidence-based rec-
cluding immune thrombocytopenic purpura (ITP), or a PID in 15% ommendations. The treatment algorithms are based on data from
of the cases (41 of 265), whereas an additional 38% of the cases (100 of retrospective reviews, case series, and from a few phase 2 pro-
265) was recognized later to be of immunological origin with an spective trials, as well as on expert experience and recommenda-
additional autoimmune disease or PID diagnosis in follow-up. tions.42 There are certainly enough data and experience to conclude
Moreover, 47% (23 of 49) of the children who were thought to that w-AIHA can be a fatal disease, either because of the acuity of
have a postinfectious AIHA at the time of diagnosis, with a well- the presentation or because of being refractory to treatment with
documented history of infection, turned out to have immunologic acute relapses requiring multiple lines of therapy with frequently
conditions.10 Therefore, any pediatric autoimmune cytopenia should life threatening complications. A mortality rate of 11% in adults and
elicit investigation for family history of autoimmunity (it is always 4% in children has been reported.10,43
revealing when a parent on questioning reports history of autoim-
mune cytopenia or chronic lymphadenopathy or splenomegaly) and A recent retrospective study reviewed the course, laboratory data,
consideration for an underlying immune dysregulation. treatment, and clinical outcome of 308 primary autoimmune he-
molytic anemia (AIHA) cases (including 10 pediatric patients) over
ALPS is caused by germline or occasionally somatic mutations in a follow-up period of 12 to 372 months (median, 33 months).44 Sixty
the genes FAS, FASL, or CASP10, resulting in impaired Fas- percent of these patients, had w-AIHA, 27% had CAS, 8% had
mediated lymphocyte apoptosis that allows survival of activated mixed (DAT positive for IgG and C3d with coexistence of warm
autoreactive lymphocytes.35-37 Its first manifestation in childhood is autoantibodies and high-titer cold agglutinins), and 5% were
frequently a chronic autoimmune cytopenia, usually ITP or w-AIHA, atypical (mostly DAT-negative w-AIHA). The mixed and atypical
with variable degrees of lymphadenopathy and splenomegaly. cases presented frequently with severe onset (Hb ,6 g/dL) along
Hypersplenism is occasionally contributing to cytopenias. Patients with reticulocytopenia. The level of Hb at presentation was pre-
with ALPS may develop more autoimmune manifestations, in- dictive of the relapse risk, with the more severe cases (including
cluding uveitis, hepatitis, glomerulonephritis, and interstitial lung mixed and atypical ones) having .50% cumulative incidence of
disease with lymphocytic infiltrates, whereas they are also at in- relapse after 3 years or a threefold increased risk of relapse in
creased risk for malignancy, mainly lymphomas. Therefore, high comparison with the mild cases (Hb .10 g/dL) and requiring
index of suspicion for malignancy is recommended at any age when multiple lines of treatment.44 Table 1 provides an outline for
an ALPS patient presents with refractory cytopenias.36 With the a sequential approach to treatment options for w-AIHA, which is
advent of whole exome sequencing, mutations in several genes discussed in detail below.
critical for immune cell biology, including NRAS, KRAS, MAGT1,
CASP8, FADD, PRKCD, CTLA4, LRBA, PI3K, and STAT3, have The first-line treatment of w-AIHA includes glucocorticosteroids
been identified and validated over the last few years as the cause of and likely transfusion. The first dose of steroids (1-2 mg/kg of
novel PID syndromes, each one with its own particular clinical and prednisone orally or methylprednisolone intravenously) should be
laboratory characteristics and a variable possibility for autoimmune given immediately after the call that DAT is positive. If DAT is
cytopenias.34,36,38 negative but the disease has the clinical and laboratory picture of
w-AIHA, steroid treatment should also be initiated along with
Autoimmune hemolytic anemia developing as a manifestation of PID transfusion because the atypical cases of DAT-negative w-AIHA
tends to be chronic and refractory. Although corticosteroids with are also the ones with the higher risk of mortality, either due to
or without intravenous immunoglobulin (IVIG) are frequently an precipitous hemolysis because of the antibody characteristics (eg,
effective first-line treatment, second- and third-line treatments are monomeric IgM causing w-AIHA) or because of the delay in
typically required to avoid the side effects of chronic corticosteroid treatment caused by the negative result of the routine DAT.19,27,43
use. The management of ALPS patients in clinical trials has provided It is important not to withhold RBC transfusion that can be life
valuable insights for the management of refractory AIHA and/or saving, especially in cases of brisk hemolysis and precipitous
ITP in patients with an underlying immunodeficiency either defined anemia. The pretransfusion serologic workup may be complicated
Hematology 2016 693
Table 1. Sequential approach to treatment options for w-AIHA and common dosing regimens
Treatment option Common dosing regimens
First-line treatment: with the goal to support
and stabilize during acute hemolysis
Steroids The first 72 hours, dose varies widely between different hematology teams from 1 to 2 mg/kg/dose of
prednisone every 8-12 hours up to high-dose steroids, eg, methylprednisolone 250-1000 mg/day
After the first 72 hours, the dose is decreased to 1-2 mg/kg/day in children and 30-80 mg/day in
adults
Disease is considered responsive to steroids if stabilization of Hb to .10 g/dL within 1-3 weeks
After such a response, the steroid dosing should continue for $6 months with a very slow wean
Transfusions Establish good communication with transfusion services to provide as needed to treat anemia
IVIG Usually 1 g/kg/day 3 2 days; consider when response to steroids in the acute setting is not
satisfactory
Plasmapheresis Consider when response to steroids in the acute setting is not satisfactory
Second-line treatment: in refractory disease
with no or limited response to steroids
and/or when steroids cannot be weaned
appropriately
Rituximab Most frequently 375 mg/m2 intravenously weekly for 4 weeks but decreased dose of 100 mg
intravenously weekly for 4 weeks has also been effective; caution recommended in cases of
underlying immune dysregulation, eg, ALPS
Splenectomy Caution recommended in cases of underlying immune dysregulation, eg, ALPS
Second-line treatment: when steroids
cannot be weaned appropriately
MMF 600 mg/m2 by mouth twice daily37
Sirolimus 2 mg/m2 by mouth once daily (goal trough 5-15 ng/mL)37
Danazol (off-label) Initial dosages ranged from 600 to 800 mg/day (by mouth in 3-4 divided doses), with maintenance
therapy of 200-600 mg/day
Third-line treatment: when disease relapses
or remains refractory despite 2nd line
treatment
Azathioprine In pediatrics used typically for w-AIHA accompanied by autoimmune hepatitis, at initial dose of
0.5 mg/kg titrated to response up to 2 mg/kg by mouth once daily
Adults: 1-2 mg/kg (maximum, 150 mg daily)
6-Mercaptopurine 50-75 mg/m 2 by mouth once daily (2.5 mg/kg once daily for children with body surface area
under 1 m2)53
Cyclosporine 5 mg/kg/day initially, decreased after response to 2-3 mg/kg/day by mouth divided every 12 hours
Cyclophosphamide Dosing used in ITP has been 1-2 mg/kg/day orally for $16 weeks or 300-1000 mg/m2 intravenously
for 1-3 doses every 2-4 weeks56
Fourth-line treatment: high risk treatment to
consider as last resort
High-dose cyclophosphamide 50 mg/kg/day for 4 days followed by granulocyte colony-stimulating factor43
Alemtuzumab 3 mg intravenously or subcutaneously on day 1 and then if tolerated, 10 mg on day 2, and then if
tolerated, 30 mg on day 3, continue with maintenance 10-30 mg 3 times weekly for up to 12 weeks
HSCT Autologous or allogeneic has been used
For danazol and most of the third- and fourth-line treatment medications, limited data are available; dosing regimen is based on case reports or small case series for patients with
w-AIHA or dosages that have been used in patients with ITP.
by the presence of autoantibodies, but transfusion services can a fatal outcome.43 Lechner and Jäger42 recommend an in vivo
usually evaluate for underlying alloantibodies that may have de- compatibility test when initiating a packed RBC transfusion in
veloped as a result of previous transfusions or pregnancies. Good a patient with w-AIHA: rapid infusion of 20 mL blood followed by
communication between the hematologist and the transfusion 20-minute observation. If no reaction is noted, then the rest of the
medicine physician is critical to assess and minimize the risks of unit is given at the usual speed.
transfusion in these settings.45,46 Of note, although reticulocytosis
is a typical diagnostic finding in hemolytic anemia, up to 20% of The dose of steroids used the first 72 hours varies widely between
adults and 39% of children with w-AIHA may present with re- different hematology teams from 1 to 2 mg/kg/dose of prednisone
ticulocytopenia, either due to inefficient erythropoietic response every 8 to 12 hours up to high-dose steroids, for example, 250 to
or due to autoantibody-mediated destruction of the late erythro- 1000 mg/day methylprednisolone.32,42,43 After the first 72 hours,
blasts and reticulocytes. Such cases typically demonstrate signif- the dose is decreased to 1 to 2 mg/kg/day in children and usually to
icant anemia and require aggressive transfusion support to avoid 30 to 80 mg/day in adults. About 80% of the patients with w-AIHA
694 American Society of Hematology
respond fairly well to steroids within 1 to 3 weeks,47 with stabili- may be of suboptimal effect if the patient is in considerable steroid
zation of Hb to .10 g/dL. It is strongly advised that after a complete doses), medical evaluation for fevers after splenectomy and
or partial remission, the steroid dosing continues for $6 months treatment with antibiotics is recommended. Pediatric recom-
with a very slow wean. This prolonged steroid course significantly mendations include postsplenectomy prophylactic antibiotics.
decreases the risk of relapse.43 A point to be made here is that, in Thromboprophylaxis with low-molecular-weight heparin at least
contrast, steroids are not indicated in CAS, where they are rarely for the postoperative period is usually recommended for adults.42
necessary or effective; if started in those cases, they should be As discussed above, in children, where w-AIHA is frequently
aggressively weaned off.43 High-dose IVIG (usually 1 g/kg dose 3 a manifestation of an underlying immune dysregulation with
2 days) and plasmapheresis have been used in w-AIHA, although varying degrees of immunodeficiency, the infectious risks after
with inconsistent results, when response to steroids in the acute splenectomy or rituximab need to be strongly considered. Lessons
setting is not satisfactory. that we learn from autoimmune cytopenias and primary immu-
nodeficiency in children may expand to young adults because
Refractory patients, with no or limited response to steroids, require even monogenic PID disorders have a variable phenotype se-
diagnostic reevaluation for an underlying disease, especially ma- verity, and it is likely that less severe forms present after
lignancy or rheumatologic disorders.42,43 Warm IgM AIHA also childhood. Therefore, a heightened awareness for such conditions
tends to be steroid refractory and the presence of these antibodies is needed to follow the Hippocratic oath to “first do no harm.” If
may have not been recognized if they exist in parallel to IgG in mixed steroids cannot be weaned appropriately with consequent high
w-AIHA. Control of the primary disease that has predisposed to risk of development of side effects (hypertension, drug-induced
the development of w-AIHA is typically necessary for improvement diabetes, osteoporosis, etc), a steroid-sparing medication with
in hemolysis. Additionally, a second-line approach for AIHA will a low side effect profile will need to be added such as MMF or
need to be considered in cases of refractory disease, which may be danazol.42,43,52 Recent pediatric experience with sirolimus in
rituximab or splenectomy. Rituximab (anti-CD20 monoclonal patients with autoimmune cytopenias and ALPS adds sirolimus
antibody targeting B-lymphocytes) is an off-label medication as a consideration at this step.32,36,39
for autoimmune cytopenias, including w-AIHA. It has been used
as a second-line treatment before or after splenectomy with on- In the pre-rituximab era, azathioprine, 6-mercaptopurine, cyclo-
going debate on which should be the first choice in second-line sporine, and cyclophosphamide were used as second-line therapy;
management.42,43 The decision is individualized based on pa- these medications are now reserved as third-line treatment due to
tient’s age, comorbidities, and preference; several centers, especially inadequate data on efficacy and the high risk of side effects.42,43,53
pediatric ones, use rituximab as immediate second-line therapy High-dose cyclophosphamide and alemtuzumab (anti-CD52 mono-
before splenectomy. Adverse events may include reactions to in- clonal antibody targeting mature lymphocytes) have shown an effi-
fusion, hepatitis B reactivation, opportunistic infections, and on rare cacy of 60% to 80% in the few cases treated with these medications
occasions progressive multifocal leukoencephalopathy. Long-term as a “last resort” due to their high-risk profile. Alemtuzumab has
hypogammaglobulinemia has been observed after rituximab treat- been especially effective (ORR, 92%) in 12 cases of CLL-associated
ment of autoimmune cytopenias with consequent IVIG dependency w-AIHA.43 Hematopoietic stem cell transplant (HSCT) has been
(reported in 2 of 135 patients [~1.5%] treated with rituximab tried as treatment of patients with w-AIHA with rather disap-
for ITP).48 This complication may be more likely in patients with pointing results. Fourteen patients with refractory cytopenias
underline hypogammaglobilinemia49 or after repeated rituximab (7 with w-AIHA, and 7 with Evans syndrome) were reported as
courses.50 A meta-analysis of 21 studies of rituximab use in patients transplant recipients by the Registry of the European Group of
with AIHA (standard dosing of 375 mg/m2 intravenously weekly Blood and Marrow Transplantation; continuous remission was
for 4 weeks) concluded that the overall response rate (ORR) for achieved only in 1 of 7 patients who had autologous HSCT and in
154 patients with w-AIHA was close to 70%, whereas the complete 3 of 7 who had allogeneic HSCT, with a transplant-related mor-
response rate evaluated within 2 to 4 months after treatment was tality of ~15%.54
42%. Of 364 patients with w-AIHA or CAS who were evaluated for
toxicity of rituximab, 38 adverse events were noted, mostly infusion w-AIHA is a chronic disease. Patients, even after response to
related, and 1 case of opportunistic infection (Pneumocystis jiroveci steroids, have a .60% probability to relapse after steroid ta-
pneumonia).51 Low-dose rituximab (100 mg fixed dose for 4 weekly pering and withdrawal.43,55 Further understanding of the path-
infusions) was also studied as a second-line therapy in 23 patients ogenesis and the variability of the disease will be necessary to
with AIHA (14 with w-AIHA and 9 with CAS).44 The ORR for optimally tailor individualized treatment strategies with the goal
the patients with w-AIHA was 100% up to a year after treatment, of optimal efficacy with the lowest possible short- and long-term
with estimated relapsed-free survival at 2 years of 81%. Because toxicity.
the IgG-coated RBCs in w-AIHA are phagocytosed by the Fcg
receptor–carrying macrophages of the spleen, it is not surprising Acknowledgment
that splenectomy is effective for w-AIHA at least in short-term The authors would like to acknowledge the Henry Loring Masters
follow-up.42 Relapses are noted in 50% to 80% of patients in long- Foundation, Inc., established in memory of Henry, a young adult
term (.2 years) follow-up, but frequently patients require a low who died of AIHA at 25 years of age, with the goal to build
dose of steroids (15 mg of prednisone per day or less) to maintain awareness of the risks of death due to w-AIHA and support the need
a Hb .10 g/dL.42 The increased risk of sepsis from encapsulated for further education and research.
organisms (pneumococci, meningococci, and hemophilus in-
fluenzae) and of venous thromboembolism after splenectomy Correspondence
should be considered and discussed with the patients, especially Theodosia A. Kalfa, Division of Hematology, Cincinnati Children’s
to identify concurrent risk factors for infection or thrombosis. Hospital Medical Center, 3333 Burnet Ave, MLC 7015, Cincinnati,
Immunizations preferably .6 weeks before splenectomy (which OH 45229-3039; e-mail: theodosia.kalfa@cchmc.org.
Hematology 2016 695
References 26. Leger RM, Co A, Hunt P, Garrity G. Attempts to support an immune
1. Franco RS. Measurement of red cell lifespan and aging. Transfus Med etiology in 800 patients with direct antiglobulin test-negative hemolytic
Hemother. 2012;39(5):302-307. anemia. Immunohematology. 2010;26(4):156-160.
2. Garratty G. The James Blundell Award Lecture 2007: do we really un- 27. Arndt PA, Leger RM, Garratty G. Serologic findings in autoimmune
derstand immune red cell destruction? Transfus Med. 2008;18(6):321-334. hemolytic anemia associated with immunoglobulin M warm autoanti-
3. Barcellini W. New insights in the pathogenesis of autoimmune hemolytic bodies. Transfusion. 2009;49(2):235-242.
anemia. Transfus Med Hemother. 2015;42(5):287-293. 28. Biagi E, Assali G, Rossi F, Jankovic M, Nicolini B, Balduzzi A.
4. Coombs RR, Mourant AE, Race RR. A new test for the detection of weak A persistent severe autoimmune hemolytic anemia despite apparent
and incomplete Rh agglutinins. Br J Exp Pathol. 1945;26:255-266. direct antiglobulin test negativization. Haematologica. 1999;84(11):
5. Zantek ND, Koepsell SA, Tharp DR Jr, Cohn CS. The direct antiglobulin 1043-1045.
test: a critical step in the evaluation of hemolysis. Am J Hematol. 2012; 29. Karafin MS, Denomme GA, Schanen M, Gottschall JL. Clinical and
87(7):707-709. reference lab characteristics of patients with suspected direct antiglobulin
6. Barros MM, Blajchman MA, Bordin JO. Warm autoimmune hemolytic test (DAT)-negative immune hemolytic anemia. Immunohematology.
anemia: recent progress in understanding the immunobiology and the 2015;31(3):108-115.
treatment. Transfus Med Rev. 2010;24(3):195-210. 30. Sachs UJ, Röder L, Santoso S, Bein G. Does a negative direct anti-
7. Bass GF, Tuscano ET, Tuscano JM. Diagnosis and classification of globulin test exclude warm autoimmune haemolytic anaemia? A pro-
autoimmune hemolytic anemia. Autoimmun Rev. 2014;13(4-5):560-564. spective study of 504 cases. Br J Haematol. 2006;132(5):655-656.
8. Michel M. Classification and therapeutic approaches in autoimmune 31. Evans RS, Takahashi K, Duane RT, Payne R, Liu C. Primary throm-
hemolytic anemia: an update. Expert Rev Hematol. 2011;4(6):607-618. bocytopenic purpura and acquired hemolytic anemia; evidence for
9. Sokol RJ, Hewitt S, Stamps BK. Autoimmune haemolysis: an 18-year a common etiology. AMA Arch Intern Med. 1951;87(1):48-65.
study of 865 cases referred to a regional transfusion centre. Br Med J 32. Miano M. How I manage Evans Syndrome and AIHA cases in children.
(Clin Res Ed). 1981;282(6281):2023-2027. Br J Haematol. 2016;172(4):524-534.
10. Aladjidi N, Leverger G, Leblanc T, et al; Centre de Référence National des 33. Ghosh S, Seidel MG. Editorial: current challenges in immune and other
Cytopénies Auto-immunes de l’Enfant (CEREVANCE). New insights into acquired cytopenias of childhood. Front Pediatr. 2016;4:3.
childhood autoimmune hemolytic anemia: a French national observational 34. Seidel MG. Autoimmune and other cytopenias in primary immunode-
study of 265 children. Haematologica. 2011;96(5):655-663. ficiencies: pathomechanisms, novel differential diagnoses, and treatment.
11. Sokol RJ, Hewitt S, Stamps BK, Hitchen PA. Autoimmune haemolysis Blood. 2014;124(15):2337-2344.
in childhood and adolescence. Acta Haematol. 1984;72(4):245-257. 35. Teachey DT. New advances in the diagnosis and treatment of autoimmune
12. Berentsen S. Role of complement in autoimmune hemolytic anemia. lymphoproliferative syndrome. Curr Opin Pediatr. 2012;24(1):1-8.
Transfus Med Hemother. 2015;42(5):303-310. 36. Rao VK. Approaches to managing autoimmune cytopenias in novel
13. Ma K, Caplan S. Refractory IgG warm autoimmune hemolytic anemia immunological disorders with genetic underpinnings like autoimmune
treated with eculizumab: a novel application of anticomplement therapy. lymphoproliferative syndrome. Front Pediatr. 2015;3:65.
Case Rep Hematol. 2016;2016:9181698. 37. Teachey DT, Seif AE, Grupp SA. Advances in the management and
14. LoBuglio AF, Cotran RS, Jandl JH. Red cells coated with immuno- understanding of autoimmune lymphoproliferative syndrome (ALPS).
globulin G: binding and sphering by mononuclear cells in man. Science. Br J Haematol. 2010;148(2):205-216.
1967;158(3808):1582-1585. 38. Oliveira JB. The expanding spectrum of the autoimmune lymphopro-
15. Barcellini W, Clerici G, Montesano R, et al. In vitro quantification of anti- liferative syndromes. Curr Opin Pediatr. 2013;25(6):722-729.
red blood cell antibody production in idiopathic autoimmune haemolytic 39. Bride KL, Vincent T, Smith-Whitley K, et al. Sirolimus is effective in
anaemia: effect of mitogen and cytokine stimulation. Br J Haematol. relapsed/refractory autoimmune cytopenias: results of a prospective
2000;111(2):452-460. multi-institutional trial. Blood. 2016;127(1):17-28.
16. Ahmad E, Elgohary T, Ibrahim H. Naturally occurring regulatory T cells and 40. Price S, Shaw PA, Seitz A, et al. Natural history of autoimmune lym-
interleukins 10 and 12 in the pathogenesis of idiopathic warm autoimmune phoproliferative syndrome associated with FAS gene mutations. Blood.
hemolytic anemia. J Investig Allergol Clin Immunol. 2011;21(4):297-304. 2014;123(13):1989-1999.
17. Evans RS, Weiser RS. The serology of autoimmune hemolytic disease; 41. Neven B, Bruneau J, Stolzenberg MC, et al. Defective anti-
observations on forty-one patients. AMA Arch Intern Med. 1957;100(3): polysaccharide response and splenic marginal zone disorganization in
371-399. ALPS patients. Blood. 2014;124(10):1597-1609.
18. Segel GB, Lichtman MA. Direct antiglobulin (“Coombs”) test-negative 42. Lechner K, Jäger U. How I treat autoimmune hemolytic anemias in
autoimmune hemolytic anemia: a review. Blood Cells Mol Dis. 2014; adults. Blood. 2010;116(11):1831-1838.
52(4):152-160. 43. Zanella A, Barcellini W. Treatment of autoimmune hemolytic anemias.
19. Kamesaki T, Toyotsuji T, Kajii E. Characterization of direct antiglobulin Haematologica. 2014;99(10):1547-1554.
test-negative autoimmune hemolytic anemia: a study of 154 cases. Am J 44. Barcellini W, Fattizzo B, Zaninoni A, et al. Clinical heterogeneity and
Hematol. 2013;88(2):93-96. predictors of outcome in primary autoimmune hemolytic anemia:
20. Kajii E, Omi T, Miura Y, Ikemoto S. [A new approach for diagnosis of a GIMEMA study of 308 patients. Blood. 2014;124(19):2930-2936.
autoimmune hemolytic anemia]. Rinsho Ketsueki. 1994;35(4):336-340. 45. King KE, Ness PM. Treatment of autoimmune hemolytic anemia. Semin
21. Gilliland BC, Baxter E, Evans RS. Red-cell antibodies in acquired he- Hematol. 2005;42(3):131-136.
molytic anemia with negative antiglobulin serum tests. N Engl J Med. 46. Petz LD. A physician’s guide to transfusion in autoimmune haemolytic
1971;285(5):252-256. anaemia. Br J Haematol. 2004;124(6):712-716.
22. Chaudhary R, Das SS, Gupta R, Khetan D. Application of flow cytometry 47. Murphy S, LoBuglio AF. Drug therapy of autoimmune hemolytic
in detection of red-cell-bound IgG in Coombs-negative AIHA. Hema- anemia. Semin Hematol. 1976;13(4):323-334.
tology. 2006;11(4):295-300. 48. Patel VL, Mahévas M, Lee SY, et al. Outcomes 5 years after response to
23. Fayek MH, Saad AA, Eissa DG, Tawfik LM, Kamal G. Role of gel test rituximab therapy in children and adults with immune thrombocytopenia.
and flow cytometry in diagnosis of Coombs’ negative autoimmune Blood. 2012;119(25):5989-5995.
haemolytic anaemia. Int J Lab Hematol. 2012;34(3):311-319. 49. Diwakar L, Gorrie S, Richter A, et al. Does rituximab aggravate pre-
24. Sokol RJ, Booker DJ, Stamps R, Jalihal S, Paul B. Direct Coombs test- existing hypogammaglobulinaemia? J Clin Pathol. 2010;63(3):275-277.
negative autoimmune hemolytic anemia and low-affinity IgG class an- 50. Cooper N, Davies EG, Thrasher AJ. Repeated courses of rituximab for au-
tibodies. Immunohematology. 1997;13(4):115-118. toimmune cytopenias may precipitate profound hypogammaglobulinaemia
25. Sokol RJ, Booker DJ, Stamps R, Booth JR. Autoimmune hemolytic anemia requiring replacement intravenous immunoglobulin. Br J Haematol. 2009;
due to IgA class autoantibodies. Immunohematology. 1996;12(1):14-19. 146(1):120-122.
696 American Society of Hematology
51. Reynaud Q, Durieu I, Dutertre M, et al. Efficacy and safety of rituximab Haematopoietic SCT in severe autoimmune diseases: updated guidelines
in auto-immune hemolytic anemia: A meta-analysis of 21 studies. of the European Group for Blood and Marrow Transplantation. Bone
Autoimmun Rev. 2015;14(4):304-313. Marrow Transplant. 2012;47(6):770-790.
52. Ahn YS, Harrington WJ, Mylvaganam R, Ayub J, Pall LM. Danazol therapy 55. Kulpa J, Skrabs C, Simanek R, et al. Probability of remaining in
for autoimmune hemolytic anemia. Ann Intern Med. 1985;102(3):298-301. unsustained complete remission after steroid therapy withdrawal in
53. Sobota A, Neufeld EJ, Lapsia S, Bennett CM. Response to mercapto- patients with primary warm-antibody reactive autoimmune hemolytic
purine for refractory autoimmune cytopenias in children. Pediatr Blood anemia. Wien Klin Wochenschr. 2016;128(7-8):234-237.
Cancer. 2009;52(1):80-84. 56. Provan D, Stasi R, Newland AC, et al. International consensus report on
54. Snowden JA, Saccardi R, Allez M, et al; EBMT Autoimmune Disease the investigation and management of primary immune thrombocytope-
Working Party (ADWP); Paediatric Diseases Working Party (PDWP). nia. Blood. 2010;115(2):168-186.
Hematology 2016 697
You might also like
- Acls Pre Course Self Assessment Study Guide100% (11)Acls Pre Course Self Assessment Study Guide7 pages
- Updates in The Management of Warm Autoimmune Hemolytic AnemiaNo ratings yetUpdates in The Management of Warm Autoimmune Hemolytic Anemia15 pages
- Warm Autoimmune Hemolytic Anemia: Recent Progress in Understanding The Immunobiology and The TreatmentNo ratings yetWarm Autoimmune Hemolytic Anemia: Recent Progress in Understanding The Immunobiology and The Treatment16 pages
- Autoimmune Hemolytic Anemia: Bradley C. Gehrs and Richard C. FriedbergNo ratings yetAutoimmune Hemolytic Anemia: Bradley C. Gehrs and Richard C. Friedberg14 pages
- Autoimmune Hemolytic Anemia (AIHA) : Becca Greenstein and Rebekah Wood Immunology 2 December 2014No ratings yetAutoimmune Hemolytic Anemia (AIHA) : Becca Greenstein and Rebekah Wood Immunology 2 December 201412 pages
- Warm Autoimmune Hemolytic Anemia (AIHA) in AdultsNo ratings yetWarm Autoimmune Hemolytic Anemia (AIHA) in Adults45 pages
- Autoimmune Hemolytic Anemia: Anita Hill and Quentin A. HillNo ratings yetAutoimmune Hemolytic Anemia: Anita Hill and Quentin A. Hill8 pages
- Autoimmune Hemolytic Anemia: From Lab To Bedside: Review ArticleNo ratings yetAutoimmune Hemolytic Anemia: From Lab To Bedside: Review Article9 pages
- The Clinical Pictures of Autoimmune Hemolytic Anemia: Charles H. PackmanNo ratings yetThe Clinical Pictures of Autoimmune Hemolytic Anemia: Charles H. Packman8 pages
- Autoimmune Hemolytic Anemia Diagnosis and Differential DiagnosisNo ratings yetAutoimmune Hemolytic Anemia Diagnosis and Differential Diagnosis10 pages
- Mixed-Type Autoimmune (Hand Out) : Renegado Janine PNo ratings yetMixed-Type Autoimmune (Hand Out) : Renegado Janine P2 pages
- How I Treat Autoimmune Hemolytic AnemiaNo ratings yetHow I Treat Autoimmune Hemolytic Anemia32 pages
- Warm Autoimmune Hemolytic Anemia: Advances in Pathophysiology and TreatmentNo ratings yetWarm Autoimmune Hemolytic Anemia: Advances in Pathophysiology and Treatment8 pages
- Diagnostic Testing and Interpretation of Tests ForNo ratings yetDiagnostic Testing and Interpretation of Tests For10 pages
- Autoimmune Hepatitis - Pathogenesis - UpToDateNo ratings yetAutoimmune Hepatitis - Pathogenesis - UpToDate11 pages
- Pathomecanisme Autoimmune Hemolytic AnemiaNo ratings yetPathomecanisme Autoimmune Hemolytic Anemia3 pages
- Aquired Haemolytic Anaemia-Handout-By DR - Chandima Kulathilake-26th BatchNo ratings yetAquired Haemolytic Anaemia-Handout-By DR - Chandima Kulathilake-26th Batch8 pages
- Haemolytic Anemia by DR Gireesh Kumar K P, Department of Emergency Medicine, Amrita Institute of Medical Sciences, Kochi, KeralaNo ratings yetHaemolytic Anemia by DR Gireesh Kumar K P, Department of Emergency Medicine, Amrita Institute of Medical Sciences, Kochi, Kerala14 pages
- Pathology SGD 4: Diseases-Of-The-Immune-System: Group-4No ratings yetPathology SGD 4: Diseases-Of-The-Immune-System: Group-423 pages
- Archive CourseprintPDF Immune Hemolytic Anemias 221144 2f02d5eb D7e5 4f0f Bc16 1261f0c88b18No ratings yetArchive CourseprintPDF Immune Hemolytic Anemias 221144 2f02d5eb D7e5 4f0f Bc16 1261f0c88b1824 pages
- 79-Year-Old Woman With Jaundice and Anemia: Residents ' ClinicNo ratings yet79-Year-Old Woman With Jaundice and Anemia: Residents ' Clinic5 pages
- Autoimmune Hepatitis: Diagnostic Criteria and Serological TestingNo ratings yetAutoimmune Hepatitis: Diagnostic Criteria and Serological Testing4 pages
- (03241750 - Acta Medica Bulgarica) A Case of Agglutination and Hemolysis of Erythrocytes Caused by The Patient's Own PlasmaNo ratings yet(03241750 - Acta Medica Bulgarica) A Case of Agglutination and Hemolysis of Erythrocytes Caused by The Patient's Own Plasma6 pages
- Hemolytic-Anemias 2021-Haber-Lecture Pres.No ratings yetHemolytic-Anemias 2021-Haber-Lecture Pres.71 pages
- A Comprehensive Exploration of Autoimmune Hemolytic Anemia and Holistic Well-beingFrom EverandA Comprehensive Exploration of Autoimmune Hemolytic Anemia and Holistic Well-beingNo ratings yet
- Eczm Policies and Procedures Part 2 - HerpetologyNo ratings yetEczm Policies and Procedures Part 2 - Herpetology19 pages
- Rekayasa Genetik, Konsultasi Genetik Dan Terapi GeneNo ratings yetRekayasa Genetik, Konsultasi Genetik Dan Terapi Gene124 pages
- Thyroid Function Tests: A Review: G. Shivaraj, B. Desai Prakash, V. Sonal, K. Shruthi, H. Vinayak, M. AvinashNo ratings yetThyroid Function Tests: A Review: G. Shivaraj, B. Desai Prakash, V. Sonal, K. Shruthi, H. Vinayak, M. Avinash9 pages
- Lecture 06.8 (Dr. Althekair's Lecture) - Common Peripheral NeuropathiesNo ratings yetLecture 06.8 (Dr. Althekair's Lecture) - Common Peripheral Neuropathies68 pages
- Significance of Fermented Food in Nutrition and Food ScienceNo ratings yetSignificance of Fermented Food in Nutrition and Food Science14 pages
- Use of Opend Vaccine Vial in ImmunizationNo ratings yetUse of Opend Vaccine Vial in Immunization9 pages
- Instant Download Allergy Essentials, 2nd Edition Robyn E O'Hehir - Ebook PDF PDF All Chapters100% (5)Instant Download Allergy Essentials, 2nd Edition Robyn E O'Hehir - Ebook PDF PDF All Chapters41 pages
- Critical Care After Major Surgery A Systematic Review of Risk Factors Unplanned Admission - Onwochei UK 2020No ratings yetCritical Care After Major Surgery A Systematic Review of Risk Factors Unplanned Admission - Onwochei UK 202013 pages
- Manual Vacuum Aspiration: An Outpatient Alternative For Surgical Management of MiscarriageNo ratings yetManual Vacuum Aspiration: An Outpatient Alternative For Surgical Management of Miscarriage5 pages
- No Need To Ask Income or Wage For OBC Caste Certificate' - TN Govt Tells CollectorsNo ratings yetNo Need To Ask Income or Wage For OBC Caste Certificate' - TN Govt Tells Collectors6 pages
- Stem Cell-Derived Exosomes For Wound Healing: Current Status and Promising DirectionsNo ratings yetStem Cell-Derived Exosomes For Wound Healing: Current Status and Promising Directions17 pages

























































































- Updates in The Management of Warm Autoimmune Hemolytic AnemiaUpdates in The Management of Warm Autoimmune Hemolytic Anemia
- Warm Autoimmune Hemolytic Anemia: Recent Progress in Understanding The Immunobiology and The TreatmentWarm Autoimmune Hemolytic Anemia: Recent Progress in Understanding The Immunobiology and The Treatment
- Autoimmune Hemolytic Anemia: Bradley C. Gehrs and Richard C. FriedbergAutoimmune Hemolytic Anemia: Bradley C. Gehrs and Richard C. Friedberg
- Autoimmune Hemolytic Anemia (AIHA) : Becca Greenstein and Rebekah Wood Immunology 2 December 2014Autoimmune Hemolytic Anemia (AIHA) : Becca Greenstein and Rebekah Wood Immunology 2 December 2014
- Autoimmune Hemolytic Anemia: Anita Hill and Quentin A. HillAutoimmune Hemolytic Anemia: Anita Hill and Quentin A. Hill
- Autoimmune Hemolytic Anemia: From Lab To Bedside: Review ArticleAutoimmune Hemolytic Anemia: From Lab To Bedside: Review Article
- The Clinical Pictures of Autoimmune Hemolytic Anemia: Charles H. PackmanThe Clinical Pictures of Autoimmune Hemolytic Anemia: Charles H. Packman
- Autoimmune Hemolytic Anemia Diagnosis and Differential DiagnosisAutoimmune Hemolytic Anemia Diagnosis and Differential Diagnosis
- Mixed-Type Autoimmune (Hand Out) : Renegado Janine PMixed-Type Autoimmune (Hand Out) : Renegado Janine P
- Warm Autoimmune Hemolytic Anemia: Advances in Pathophysiology and TreatmentWarm Autoimmune Hemolytic Anemia: Advances in Pathophysiology and Treatment
- Diagnostic Testing and Interpretation of Tests ForDiagnostic Testing and Interpretation of Tests For
- Aquired Haemolytic Anaemia-Handout-By DR - Chandima Kulathilake-26th BatchAquired Haemolytic Anaemia-Handout-By DR - Chandima Kulathilake-26th Batch
- Haemolytic Anemia by DR Gireesh Kumar K P, Department of Emergency Medicine, Amrita Institute of Medical Sciences, Kochi, KeralaHaemolytic Anemia by DR Gireesh Kumar K P, Department of Emergency Medicine, Amrita Institute of Medical Sciences, Kochi, Kerala
- Pathology SGD 4: Diseases-Of-The-Immune-System: Group-4Pathology SGD 4: Diseases-Of-The-Immune-System: Group-4
- Archive CourseprintPDF Immune Hemolytic Anemias 221144 2f02d5eb D7e5 4f0f Bc16 1261f0c88b18Archive CourseprintPDF Immune Hemolytic Anemias 221144 2f02d5eb D7e5 4f0f Bc16 1261f0c88b18
- 79-Year-Old Woman With Jaundice and Anemia: Residents ' Clinic79-Year-Old Woman With Jaundice and Anemia: Residents ' Clinic
- Autoimmune Hepatitis: Diagnostic Criteria and Serological TestingAutoimmune Hepatitis: Diagnostic Criteria and Serological Testing
- (03241750 - Acta Medica Bulgarica) A Case of Agglutination and Hemolysis of Erythrocytes Caused by The Patient's Own Plasma(03241750 - Acta Medica Bulgarica) A Case of Agglutination and Hemolysis of Erythrocytes Caused by The Patient's Own Plasma
- A Comprehensive Exploration of Autoimmune Hemolytic Anemia and Holistic Well-beingFrom EverandA Comprehensive Exploration of Autoimmune Hemolytic Anemia and Holistic Well-being
- Rekayasa Genetik, Konsultasi Genetik Dan Terapi GeneRekayasa Genetik, Konsultasi Genetik Dan Terapi Gene
- Thyroid Function Tests: A Review: G. Shivaraj, B. Desai Prakash, V. Sonal, K. Shruthi, H. Vinayak, M. AvinashThyroid Function Tests: A Review: G. Shivaraj, B. Desai Prakash, V. Sonal, K. Shruthi, H. Vinayak, M. Avinash
- Lecture 06.8 (Dr. Althekair's Lecture) - Common Peripheral NeuropathiesLecture 06.8 (Dr. Althekair's Lecture) - Common Peripheral Neuropathies
- Significance of Fermented Food in Nutrition and Food ScienceSignificance of Fermented Food in Nutrition and Food Science
- Instant Download Allergy Essentials, 2nd Edition Robyn E O'Hehir - Ebook PDF PDF All ChaptersInstant Download Allergy Essentials, 2nd Edition Robyn E O'Hehir - Ebook PDF PDF All Chapters
- Critical Care After Major Surgery A Systematic Review of Risk Factors Unplanned Admission - Onwochei UK 2020Critical Care After Major Surgery A Systematic Review of Risk Factors Unplanned Admission - Onwochei UK 2020
- Manual Vacuum Aspiration: An Outpatient Alternative For Surgical Management of MiscarriageManual Vacuum Aspiration: An Outpatient Alternative For Surgical Management of Miscarriage
- No Need To Ask Income or Wage For OBC Caste Certificate' - TN Govt Tells CollectorsNo Need To Ask Income or Wage For OBC Caste Certificate' - TN Govt Tells Collectors
- Stem Cell-Derived Exosomes For Wound Healing: Current Status and Promising DirectionsStem Cell-Derived Exosomes For Wound Healing: Current Status and Promising Directions