Effect of A Physiotherapy Rehabilitation Program On Knee Osteoarthritis in Patients With Different Pain Intensities
Effect of A Physiotherapy Rehabilitation Program On Knee Osteoarthritis in Patients With Different Pain Intensities
Download as pdf or txt
You might also like
- Total Gym 1000Document30 pagesTotal Gym 1000manhtuan15a88% (24)
- Surgical Handrub Technique PosterDocument1 pageSurgical Handrub Technique PosterAbi Zaki50% (2)
- 01a Using Anatomical LanguageDocument6 pages01a Using Anatomical Languageapi-3067625270% (1)
- Ultimate Calisthenics Full Body Workout PDFDocument10 pagesUltimate Calisthenics Full Body Workout PDFelie bejjaniNo ratings yet
- Efficacy of Retrowalking in Patients With Chronic Knee Osteoarthritis: A Single Group Experimental Pilot StudyDocument9 pagesEfficacy of Retrowalking in Patients With Chronic Knee Osteoarthritis: A Single Group Experimental Pilot StudyDr. Krishna N. SharmaNo ratings yet
- Effects of Kinesiotherapy, Ultrasound and Electrotherapy in Management of Bilateral Knee Osteoarthritis: Prospective Clinical TrialDocument10 pagesEffects of Kinesiotherapy, Ultrasound and Electrotherapy in Management of Bilateral Knee Osteoarthritis: Prospective Clinical TrialDavid Alejandro Cavieres AcuñaNo ratings yet
- The Effect of Proprioceptive Neuromuscular Facilitation Techniques On Muscular Strength in Patients With Knee Osteoarthritis - A Quasi-Experimental StudyDocument7 pagesThe Effect of Proprioceptive Neuromuscular Facilitation Techniques On Muscular Strength in Patients With Knee Osteoarthritis - A Quasi-Experimental Studyemotion.physiotherapyNo ratings yet
- The Effect of Hot Intermittent Cupping On Pain, Stiffness and Disability of Patients With Knee OsteoarthritisDocument8 pagesThe Effect of Hot Intermittent Cupping On Pain, Stiffness and Disability of Patients With Knee OsteoarthritisAsaad AlnhayerNo ratings yet
- Comparison Between Outcomes of Dry Needling With Conventional Protocol and Rood's Approach With Conventional Protocol On Pain, Strength and Balance in Knee OsteoarthritisDocument29 pagesComparison Between Outcomes of Dry Needling With Conventional Protocol and Rood's Approach With Conventional Protocol On Pain, Strength and Balance in Knee OsteoarthritisDrPratibha SinghNo ratings yet
- Evaluating Meridian-Sinew Release Therapy For The Treatment of Knee OsteoarthritisDocument10 pagesEvaluating Meridian-Sinew Release Therapy For The Treatment of Knee OsteoarthritisGuilherme PenicheNo ratings yet
- Effectiveness of Kinesio Taping On Pain and Function After Total Knee ArthroplastyDocument3 pagesEffectiveness of Kinesio Taping On Pain and Function After Total Knee Arthroplastycharmainemargaret.parreno.medNo ratings yet
- Koca Et Al (2014)Document6 pagesKoca Et Al (2014)Mateja BrebenNo ratings yet
- Therapeutic Features of Medical Care of Knee Osteoarthritis A Study of 60 Cases 2329 9096 1000295Document4 pagesTherapeutic Features of Medical Care of Knee Osteoarthritis A Study of 60 Cases 2329 9096 1000295hanindyo rizkyNo ratings yet
- Jpts 29 1689Document6 pagesJpts 29 1689sakyeadropsNo ratings yet
- Oa KneeDocument9 pagesOa KneerohanaNo ratings yet
- Evaluation of The Lateral Instability of The Ankle by Inversion Simulation Device and Assessment of The Rehabilitation ProgramDocument13 pagesEvaluation of The Lateral Instability of The Ankle by Inversion Simulation Device and Assessment of The Rehabilitation ProgramZzDel VerdeNo ratings yet
- Babaei Ghazani2018Document11 pagesBabaei Ghazani2018Renato BastosNo ratings yet
- Journal of Rehabilitation Sciences and Research: Journal Home Page: JRSR - Sums.ac - IrDocument6 pagesJournal of Rehabilitation Sciences and Research: Journal Home Page: JRSR - Sums.ac - IrAtika MayadahNo ratings yet
- Relationship Between Pain Intensity, Pain Catastrophizing, and Self-Efficacy in Patients With Frozen Shoulder: A Cross-Sectional StudyDocument6 pagesRelationship Between Pain Intensity, Pain Catastrophizing, and Self-Efficacy in Patients With Frozen Shoulder: A Cross-Sectional Studyluisherrera1490No ratings yet
- OA Manual Therapy ArticleDocument14 pagesOA Manual Therapy ArticlekapilphysioNo ratings yet
- Ijss Aug Oa12Document5 pagesIjss Aug Oa12Herry HendrayadiNo ratings yet
- The Effect of Obesity On Surgical Treatment of Achilles Tendon RupturesDocument7 pagesThe Effect of Obesity On Surgical Treatment of Achilles Tendon RupturesMusdalipa Hi.palanroNo ratings yet
- Lasers: Effect of Laser Therapy On Chronic Osteoarthritis of The Knee in Older SubjectsDocument8 pagesLasers: Effect of Laser Therapy On Chronic Osteoarthritis of The Knee in Older SubjectsBasith HalimNo ratings yet
- Burger Et Al 2016 Effect of Corticosteroid Injections Versus Physiotherapy On Pain Shoulder Range of Motion andDocument9 pagesBurger Et Al 2016 Effect of Corticosteroid Injections Versus Physiotherapy On Pain Shoulder Range of Motion andchandni saxenaNo ratings yet
- Effect of Joint Mobilization and Kinesiotaping On Knee OsteoarthriticDocument8 pagesEffect of Joint Mobilization and Kinesiotaping On Knee OsteoarthriticAml ELsaid HamedNo ratings yet
- 17 Nor AzlinDocument5 pages17 Nor AzlinWira DharmaNo ratings yet
- Article IN Press: Pain Management NursingDocument8 pagesArticle IN Press: Pain Management NursingWahyu HidayatiNo ratings yet
- Short-Wave Diathermy in The Treatment of Knee OsteoarthritisDocument10 pagesShort-Wave Diathermy in The Treatment of Knee Osteoarthritisapi-462099014No ratings yet
- Original Article: Effects of Exercise Therapy For Knee OsteoarthritisDocument6 pagesOriginal Article: Effects of Exercise Therapy For Knee OsteoarthritisChristian NievesNo ratings yet
- Effect of Isometric Quadriceps Exercise On Muscle Strength, Pain, and Function in Patients With Knee Osteoarthritis: A Randomized Controlled StudyDocument4 pagesEffect of Isometric Quadriceps Exercise On Muscle Strength, Pain, and Function in Patients With Knee Osteoarthritis: A Randomized Controlled StudyHusnannisa ArifNo ratings yet
- No Effect of Cognitive Behavioral Patient EducatioDocument7 pagesNo Effect of Cognitive Behavioral Patient EducatioJay JalaliNo ratings yet
- Massage Therapy For Osteoarthritis of The KneeDocument6 pagesMassage Therapy For Osteoarthritis of The KneeDrAbhay ShankargoudaNo ratings yet
- Effect of Isometric Quadriceps Exercise On Muscle StrengthDocument7 pagesEffect of Isometric Quadriceps Exercise On Muscle StrengthAyu RoseNo ratings yet
- 3-6 - Isometric Exercise Versus Combined Concentric Eccentric Exercise Training in Patients With Osteoarthritis KneeDocument7 pages3-6 - Isometric Exercise Versus Combined Concentric Eccentric Exercise Training in Patients With Osteoarthritis KneeirmarizkyyNo ratings yet
- Schwerla 2020Document8 pagesSchwerla 2020João Paulo Vila Nova GomesNo ratings yet
- 2022-30.8.2022-DINABANG-SANTOS-ISAKOS - Boston-jun2023-Dinapenia-agosto2022 Resumen EnviadoDocument2 pages2022-30.8.2022-DINABANG-SANTOS-ISAKOS - Boston-jun2023-Dinapenia-agosto2022 Resumen EnviadoCristina TouriñoNo ratings yet
- Clinical StudyDocument7 pagesClinical StudyhfhfhNo ratings yet
- Penatalaksanaan Fisioterapi Pada KondisiDocument8 pagesPenatalaksanaan Fisioterapi Pada KondisiMuhamad BenyaminNo ratings yet
- Oa9 PDFDocument9 pagesOa9 PDFElias Oktovianus HaulussyNo ratings yet
- Comparison of Effect of Hip Joint Mobilization and Hip Joint Muscle Strengthening Exercises With Knee Osteoarthritis A. Tanvi, R. Amrita, R. Deepak, P. Kopal Srji Vol 3-Issue 1 Year 2014Document13 pagesComparison of Effect of Hip Joint Mobilization and Hip Joint Muscle Strengthening Exercises With Knee Osteoarthritis A. Tanvi, R. Amrita, R. Deepak, P. Kopal Srji Vol 3-Issue 1 Year 2014Dr. Krishna N. Sharma100% (1)
- 1 s2.0 S1836955319300918 Main PDFDocument7 pages1 s2.0 S1836955319300918 Main PDFJuliano BritoNo ratings yet
- The Effect of Exercise Therapy On Knee Osteoarthritis: A Randomized Clinical TrialDocument10 pagesThe Effect of Exercise Therapy On Knee Osteoarthritis: A Randomized Clinical TrialElva Diany SyamsudinNo ratings yet
- Use of The Kinesio Taping Method in Painful Shoulder SyndromeDocument6 pagesUse of The Kinesio Taping Method in Painful Shoulder SyndromeAl BnNo ratings yet
- Pain Research and Management - 2021 - Weleslassie - Effectiveness of Mobilization With Movement On The Management of KneeDocument12 pagesPain Research and Management - 2021 - Weleslassie - Effectiveness of Mobilization With Movement On The Management of Kneedenzydavid70359No ratings yet
- 1 ANALYSER PAR ETUDIANTS Article Javadov Pain PhysicianDocument12 pages1 ANALYSER PAR ETUDIANTS Article Javadov Pain PhysicianAmir JedidiNo ratings yet
- Annals of Internal Medicine: Effectiveness of Manual Physical Therapy and Exercise in Osteoarthritis of The KneeDocument9 pagesAnnals of Internal Medicine: Effectiveness of Manual Physical Therapy and Exercise in Osteoarthritis of The KneeKhadija AkhundNo ratings yet
- Artigo - US Pra Dor CrônicaDocument12 pagesArtigo - US Pra Dor CrônicaJose Carlos CamposNo ratings yet
- Jurnal Imggris Corset For LBPDocument4 pagesJurnal Imggris Corset For LBPnanik setiyowatiNo ratings yet
- The Short-Term Effects of Hydrotherapy On Pain and Self-Perceived Functional Status in Individuals Living With Osteoarthritis of The Knee JointDocument6 pagesThe Short-Term Effects of Hydrotherapy On Pain and Self-Perceived Functional Status in Individuals Living With Osteoarthritis of The Knee JointMiftah ghaniNo ratings yet
- Disability and Related Factors in Patients With Chronic Cervical Myofascial PainDocument8 pagesDisability and Related Factors in Patients With Chronic Cervical Myofascial Painaria tristayanthiNo ratings yet
- Article 9Document8 pagesArticle 9umair muqriNo ratings yet
- Alp Tekin 2016Document6 pagesAlp Tekin 2016Anisah Imansari RahayuNo ratings yet
- IntroductionDocument13 pagesIntroductionWa'daaNo ratings yet
- HVT With Lumbar Disc HerniationDocument12 pagesHVT With Lumbar Disc HerniationSheena McLennanNo ratings yet
- s13102-023-00704-5Document8 pagess13102-023-00704-5personalmhsantosNo ratings yet
- Elboim-Gabyzon Et Al (2012)Document4 pagesElboim-Gabyzon Et Al (2012)Mateja BrebenNo ratings yet
- The Impact of Glucosamine, Chondroitin Sulfate, and Features As Assessed by MRIDocument7 pagesThe Impact of Glucosamine, Chondroitin Sulfate, and Features As Assessed by MRIResearcher-VNo ratings yet
- The Effect of Mechanical Massage On Early Outcome After Total Knee ArthroplastyDocument4 pagesThe Effect of Mechanical Massage On Early Outcome After Total Knee Arthroplasty이용기No ratings yet
- JURNALDocument8 pagesJURNALYudi SutriadiNo ratings yet
- Effectiveness of Kinesiologic Tape Application in Rotator Cuff InjuriesDocument6 pagesEffectiveness of Kinesiologic Tape Application in Rotator Cuff InjuriesdarisNo ratings yet
- KNEST Keg438Document7 pagesKNEST Keg438jsyugesh21No ratings yet
- International Journal of Health Sciences and ResearchDocument7 pagesInternational Journal of Health Sciences and ResearchMuhamad BenyaminNo ratings yet
- The Influence of Chronic Pain On Postoperative PaiDocument12 pagesThe Influence of Chronic Pain On Postoperative PairflaviogjNo ratings yet
- Comprehensive Treatment of Knee Osteoarthritis: Recent AdvancesFrom EverandComprehensive Treatment of Knee Osteoarthritis: Recent AdvancesNo ratings yet
- Odontogenic Sinusitis: A Review of The Current LiteratureDocument5 pagesOdontogenic Sinusitis: A Review of The Current LiteraturefransAPNo ratings yet
- Report of CaseDocument3 pagesReport of CasefransAPNo ratings yet
- Journal 7 PDFDocument9 pagesJournal 7 PDFfransAPNo ratings yet
- Trends in Exercise Neuroscience: Raising Demand For Brain FitnessDocument4 pagesTrends in Exercise Neuroscience: Raising Demand For Brain FitnessfransAPNo ratings yet
- Total Gym Exercise ListDocument2 pagesTotal Gym Exercise ListFaisal Shafique100% (4)
- Diastasis Recti Abdominis: Diastasis Recti Abdominis and The Abdominal Wall: Considerations For The Childbearing YearDocument5 pagesDiastasis Recti Abdominis: Diastasis Recti Abdominis and The Abdominal Wall: Considerations For The Childbearing YearKollipara SandhyaNo ratings yet
- KIN 2241a Lab 1Document3 pagesKIN 2241a Lab 1Richard NgoNo ratings yet
- Facial Space InfectionsDocument76 pagesFacial Space InfectionsPrathusha UmakhanthNo ratings yet
- Pediatric Orthopedic Leg Problems: Rheumatology and Orthopedics With Brian AlversonDocument14 pagesPediatric Orthopedic Leg Problems: Rheumatology and Orthopedics With Brian Alversondoctorprepper.01No ratings yet
- 1998 Knee Injury and Osteoarthritis Outcome Score (KOOS) - Development of A Self-Administered Outcome MeasureDocument9 pages1998 Knee Injury and Osteoarthritis Outcome Score (KOOS) - Development of A Self-Administered Outcome MeasureCastro WeithNo ratings yet
- Muscles of Facial Expression and MasticationDocument41 pagesMuscles of Facial Expression and MasticationMohd AkmalNo ratings yet
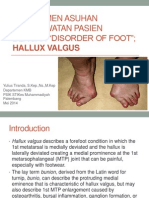
- Manajemen Asuhan Keperawatan Pasien Dengan Disorder of Foot Hammer Toe and Hallux Valgus FREEDocument29 pagesManajemen Asuhan Keperawatan Pasien Dengan Disorder of Foot Hammer Toe and Hallux Valgus FREENovita DamaiyantiNo ratings yet
- CMJ2009 - 7 (2) E4Document5 pagesCMJ2009 - 7 (2) E4sulis tiyowatiNo ratings yet
- Dickson V SA Mutual Fire & General Insurance Co LTD 1977 (2J2) QOD 725 (C)Document5 pagesDickson V SA Mutual Fire & General Insurance Co LTD 1977 (2J2) QOD 725 (C)MalvinaNo ratings yet
- Edexcel Past Paper 2006Document28 pagesEdexcel Past Paper 2006David BrownNo ratings yet
- Carpal Tunnel Syndrome: By: Dr. Masoud Shayesteh AzarDocument34 pagesCarpal Tunnel Syndrome: By: Dr. Masoud Shayesteh AzarTri Ramasari Syanggra DewiNo ratings yet
- Fitness His Edition - US 2017 1-2 Jan-Feb - 8 Week Power Building WorkoutDocument8 pagesFitness His Edition - US 2017 1-2 Jan-Feb - 8 Week Power Building Workoutsoy_bartolete100% (1)
- Stryker CORE Arthroscopic Shaver SystemDocument6 pagesStryker CORE Arthroscopic Shaver SystemEng. Edelson MartinsNo ratings yet
- SplintingDocument31 pagesSplinting4LetterLie31No ratings yet
- 3 HangingDocument22 pages3 HangingNimra TariqNo ratings yet
- Bi SyndromeDocument0 pagesBi Syndromerasputin2250% (2)
- CH 20Document98 pagesCH 20nhieuntnNo ratings yet
- Comparative Anatomy LecDocument2 pagesComparative Anatomy LecKerbie JaydNo ratings yet
- Shalya Tantra-2 (Short Book) @bamsbooksinDocument211 pagesShalya Tantra-2 (Short Book) @bamsbooksinDivya MakhareNo ratings yet
- The Squat BibleDocument6 pagesThe Squat BibleAlejandro JustoNo ratings yet
- Pe LT2Document3 pagesPe LT2Richa RodrigoNo ratings yet
- Anatomy of The Canine HindlimbDocument26 pagesAnatomy of The Canine HindlimbShuhada Hamid100% (2)
- Anatomy & Physiology 1ADocument2 pagesAnatomy & Physiology 1AkennethNo ratings yet
- Vanguard System SummaryDocument6 pagesVanguard System SummaryBobNo ratings yet
- The Aging Face: January 2016Document16 pagesThe Aging Face: January 2016David BaramidzeNo ratings yet