Hyperthyroidism in Gestational Trophoblastic Neoplasia: Clinical Endocrinology 15, 395-401
Hyperthyroidism in Gestational Trophoblastic Neoplasia: Clinical Endocrinology 15, 395-401
Download as pdf or txt
You might also like
- Sas PDFDocument2 pagesSas PDFWisnu Surya WardhanaNo ratings yet
- Letter 2024 01 18 1Document4 pagesLetter 2024 01 18 1jennifermoule0No ratings yet
- Status Epilepticus A Clinical PerspectiveDocument385 pagesStatus Epilepticus A Clinical PerspectiveNitish100% (1)
- A Hydatidiform Mole Can Cause Severe Gestational HyperthyroidismDocument3 pagesA Hydatidiform Mole Can Cause Severe Gestational HyperthyroidismhendraNo ratings yet
- Investigations For Thyroid DiseasesDocument18 pagesInvestigations For Thyroid DiseasesAjay YANo ratings yet
- Mbs127 Slide Hyperthyroidism 1Document46 pagesMbs127 Slide Hyperthyroidism 1revita262No ratings yet
- Thyroid Storm - UpToDateDocument21 pagesThyroid Storm - UpToDateJENNYLA HAZEL SICLOTNo ratings yet
- Tormenta Tiroidea: Una Urgencia Endocrinológica: Thyroid Storm: An Endocrinological UrgencyDocument4 pagesTormenta Tiroidea: Una Urgencia Endocrinológica: Thyroid Storm: An Endocrinological UrgencyConstanza Moraga HerreraNo ratings yet
- Hyperthyroidism in Pregnancy: Jorge H. MDDocument23 pagesHyperthyroidism in Pregnancy: Jorge H. MDRashid HussainNo ratings yet
- Cắt tuyến giáp điều trị Graves ở BN giảm bạch cầu hạt do MMIDocument54 pagesCắt tuyến giáp điều trị Graves ở BN giảm bạch cầu hạt do MMInhoxhaoga1999No ratings yet
- Ten KasusDocument4 pagesTen KasusIndra IhsanNo ratings yet
- GoiterDocument21 pagesGoiterAminah Safiah100% (1)
- Hypothyroidism: Kommerien Daling, MD Chiefs Conference August 14th 2008Document50 pagesHypothyroidism: Kommerien Daling, MD Chiefs Conference August 14th 2008HaNy NejNo ratings yet
- Dental Subs 123122312Document5 pagesDental Subs 123122312a1111No ratings yet
- Euthyroid Sick Syndrome in Pulmonary Tuberculosis Before and After TreatmentDocument7 pagesEuthyroid Sick Syndrome in Pulmonary Tuberculosis Before and After TreatmentMallikarjun PiskaNo ratings yet
- Therapeutics: Thyroid DisordersDocument24 pagesTherapeutics: Thyroid DisordersSharas FarhadNo ratings yet
- Endocrinologic DisordersDocument80 pagesEndocrinologic Disordersfanuiel mandefroNo ratings yet
- Hypo & HyperthyroidismDocument13 pagesHypo & Hyperthyroidismgolden fleeceNo ratings yet
- Epidemiology of Subtypes of Hyperthyroidism in Denmark: A Population-Based StudyDocument9 pagesEpidemiology of Subtypes of Hyperthyroidism in Denmark: A Population-Based StudyNaila SulhaNo ratings yet
- Clinical and Laboratory Manifestations of Typhoid Fever at Persahabatan Hospital, JakartaDocument6 pagesClinical and Laboratory Manifestations of Typhoid Fever at Persahabatan Hospital, JakartaFebyan AbotNo ratings yet
- Transfusion and Apheresis ScienceDocument4 pagesTransfusion and Apheresis ScienceroshamaharaniNo ratings yet
- Edmonds 1988Document7 pagesEdmonds 1988Nhân Phạm HuỳnhNo ratings yet
- The Diagnosis and Management of Primary Hypothyroidism: British Thyroid AssociationDocument3 pagesThe Diagnosis and Management of Primary Hypothyroidism: British Thyroid AssociationdustydiamondNo ratings yet
- Evaluation of Thyroid Hormone Status After Acute Myocardial Infarction in South IndiansDocument5 pagesEvaluation of Thyroid Hormone Status After Acute Myocardial Infarction in South Indianskhalidjamil123No ratings yet
- MCQs Endo FinalDocument6 pagesMCQs Endo Finalhassan qureshiNo ratings yet
- 4.15 DR. ROBERTO MIRASOL HYperthyroidism PSEM 2017 1 PDFDocument89 pages4.15 DR. ROBERTO MIRASOL HYperthyroidism PSEM 2017 1 PDFjackie funtanilla100% (1)
- Atow 496 00 01Document9 pagesAtow 496 00 01Nguyen Ngoc ChungNo ratings yet
- Incidence of Thyroid Cancer in Patients Operated FDocument4 pagesIncidence of Thyroid Cancer in Patients Operated FFaisal AhmedNo ratings yet
- Jurnal Kedokteran Dan Kesehatan Indonesia: Indonesian Journal of Medicine and HealthDocument6 pagesJurnal Kedokteran Dan Kesehatan Indonesia: Indonesian Journal of Medicine and Healthabidin9No ratings yet
- Adrenal Carcinoma - A Case StudyDocument3 pagesAdrenal Carcinoma - A Case StudyНиколина ГроздановскаNo ratings yet
- Лекция english Поликлиника Заб щитовиднй и паращитовидное железыDocument190 pagesЛекция english Поликлиника Заб щитовиднй и паращитовидное железыmohammed shafique ahmed hussainNo ratings yet
- Cardiac Troponin T Is Not Increased in PatientsDocument5 pagesCardiac Troponin T Is Not Increased in PatientsAnanda Putri ImsezNo ratings yet
- Dome-And-Dart T Waves and Hyperthyroidism - A Case ReportDocument3 pagesDome-And-Dart T Waves and Hyperthyroidism - A Case ReportMiftah MiftahNo ratings yet
- Thyroid by Dr. Shyam Kalavalapalli, Endocrinologist, HyderabadDocument87 pagesThyroid by Dr. Shyam Kalavalapalli, Endocrinologist, HyderabadSherman BellNo ratings yet
- Poorly Differentiated Thyroid CarcinomaDocument67 pagesPoorly Differentiated Thyroid Carcinomaperie_md100% (1)
- Toxic Multinodular GoiterDocument25 pagesToxic Multinodular GoiterGamer MadaNo ratings yet
- Thyroid-Hormone Concentrations After Radiolodine Therapy For HyperthyroidismDocument5 pagesThyroid-Hormone Concentrations After Radiolodine Therapy For HyperthyroidismShane AllenNo ratings yet
- Euthyroid Goiter With and Without Nodules-Diagnosis and TreatmentDocument12 pagesEuthyroid Goiter With and Without Nodules-Diagnosis and TreatmentOkky Winang SaktyawanNo ratings yet
- Endocrine Davidson Shortlisted (Hira - Fj'23)Document45 pagesEndocrine Davidson Shortlisted (Hira - Fj'23)saifsaffa2No ratings yet
- Goiter: Signs and Symptoms of GoitersDocument15 pagesGoiter: Signs and Symptoms of GoitersGraceLanaNo ratings yet
- Management of Thyrotoxic Crisis: A. Migneco, V. Ojetti, A. Testa, A. de Lorenzo, N. Gentiloni SilveriDocument6 pagesManagement of Thyrotoxic Crisis: A. Migneco, V. Ojetti, A. Testa, A. de Lorenzo, N. Gentiloni SilveriNur Rizqiatul AuliaNo ratings yet
- AAFP Marzo 2016 HipertiroidismoDocument11 pagesAAFP Marzo 2016 HipertiroidismoAntonio MoncadaNo ratings yet
- American Thyroid Association Guidelines For Detection of Thyroid DysfunctionDocument5 pagesAmerican Thyroid Association Guidelines For Detection of Thyroid DysfunctionUdsanee SukpimonphanNo ratings yet
- Ann Int Med 2020 - HyperthiroidismDocument19 pagesAnn Int Med 2020 - HyperthiroidismKarla WevarNo ratings yet
- Transient Rise in Intact Parathyroid Hormone Concentration After Surgery For Parathyroid AdenomaDocument6 pagesTransient Rise in Intact Parathyroid Hormone Concentration After Surgery For Parathyroid Adenomaimran qaziNo ratings yet
- Hipertiroidismo en Niños y AdolescentesDocument9 pagesHipertiroidismo en Niños y AdolescentesMiguelRoblesNo ratings yet
- Thyroid StormDocument36 pagesThyroid StormSabrina ShalhoutNo ratings yet
- Diagnosis TherapyDocument9 pagesDiagnosis TherapymarioNo ratings yet
- Thyroid Function Tests: A Review: G. Shivaraj, B. Desai Prakash, V. Sonal, K. Shruthi, H. Vinayak, M. AvinashDocument9 pagesThyroid Function Tests: A Review: G. Shivaraj, B. Desai Prakash, V. Sonal, K. Shruthi, H. Vinayak, M. Avinashbelakang rumahNo ratings yet
- IndianJEndocrMetab177184-6475539 175915Document4 pagesIndianJEndocrMetab177184-6475539 175915Atika SugiartoNo ratings yet
- Background: Excessive Release of Thyroid Hormones (THS) Hypertension Congestive Heart FailureDocument13 pagesBackground: Excessive Release of Thyroid Hormones (THS) Hypertension Congestive Heart FailureFebria ArmaNo ratings yet
- Thyroid StormDocument3 pagesThyroid StormSuprit SnNo ratings yet
- 2005 H Diagnostic Si TratamentDocument9 pages2005 H Diagnostic Si TratamentCaulfield DariaNo ratings yet
- Enteric FeverDocument20 pagesEnteric Fevergynns_15No ratings yet
- Brmedj01547 0041Document6 pagesBrmedj01547 0041داریوش بستامNo ratings yet
- Thyroid Disorders 2023Document87 pagesThyroid Disorders 2023Amir MajdiNo ratings yet
- Thyroid Disorders: Physiology of Thyroid HarmonesDocument68 pagesThyroid Disorders: Physiology of Thyroid Harmonesspicychips7No ratings yet
- Interpretation of Thyroid Function TestsDocument6 pagesInterpretation of Thyroid Function TestsJuan CanoNo ratings yet
- Subclinicsl HyperthyroidismDocument9 pagesSubclinicsl HyperthyroidismDudella Desnani Firman YasinNo ratings yet
- D'Aurizio Et Al - Free Thyroxine Measurement in Clinical Practice How To Optimize Indications Analytical Procedures and Interpretation Criteria While Waiting ForDocument41 pagesD'Aurizio Et Al - Free Thyroxine Measurement in Clinical Practice How To Optimize Indications Analytical Procedures and Interpretation Criteria While Waiting ForerixNo ratings yet
- PEAC Enfermedades de La Tiroides 2023Document22 pagesPEAC Enfermedades de La Tiroides 2023Eloisa PayanoNo ratings yet
- Neuroendocrine Tumors: Surgical Evaluation and ManagementFrom EverandNeuroendocrine Tumors: Surgical Evaluation and ManagementJordan M. CloydNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 8: UrologyFrom EverandComplementary and Alternative Medical Lab Testing Part 8: UrologyRating: 3 out of 5 stars3/5 (1)
- Schizophrenia and Other Psychotic Disorders: Agustine Mahardika MD, PsychDocument57 pagesSchizophrenia and Other Psychotic Disorders: Agustine Mahardika MD, PsychLydia AmaliaNo ratings yet
- StuntingDocument8 pagesStuntingLydia AmaliaNo ratings yet
- Pen TingDocument4 pagesPen TingLydia AmaliaNo ratings yet
- Cognitive Behavioural Therapy For Schizophrenia - Outcomes For Functioning, Distress and Quality of Life: A Meta-AnalysisDocument10 pagesCognitive Behavioural Therapy For Schizophrenia - Outcomes For Functioning, Distress and Quality of Life: A Meta-AnalysisLydia AmaliaNo ratings yet
- Ectopic Pregnancy 3.0Document19 pagesEctopic Pregnancy 3.0Lydia AmaliaNo ratings yet
- Cognitive-Behavioural Therapy For Personal Recovery of Patients With Schizophrenia: A Systematic Review and Meta-AnalysisDocument13 pagesCognitive-Behavioural Therapy For Personal Recovery of Patients With Schizophrenia: A Systematic Review and Meta-AnalysisLydia AmaliaNo ratings yet
- Exercise and The Prevention of Depression: Results of The HUNT Cohort StudyDocument9 pagesExercise and The Prevention of Depression: Results of The HUNT Cohort StudyLydia AmaliaNo ratings yet
- Textbook Geriatric Psychiatry 09 PDFDocument23 pagesTextbook Geriatric Psychiatry 09 PDFLydia AmaliaNo ratings yet
- JR 1Document9 pagesJR 1Lydia AmaliaNo ratings yet
- Review: Management of Venous Port Systems in Oncology: A Review of Current EvidenceDocument7 pagesReview: Management of Venous Port Systems in Oncology: A Review of Current EvidenceLydia AmaliaNo ratings yet
- Central Venous Port Placement in Advanced Breast Cancer Patients: Comparison of The Anatomic-Landmark and Ultrasound-Guided TechniquesDocument4 pagesCentral Venous Port Placement in Advanced Breast Cancer Patients: Comparison of The Anatomic-Landmark and Ultrasound-Guided TechniquesLydia AmaliaNo ratings yet
- Use of Port-A-Cath in Cancer Patients: A Single-Center ExperienceDocument7 pagesUse of Port-A-Cath in Cancer Patients: A Single-Center ExperienceLydia AmaliaNo ratings yet
- "Difficult To Flush Chemoport: An Important Clinical Sign": Case ReportDocument3 pages"Difficult To Flush Chemoport: An Important Clinical Sign": Case ReportLydia AmaliaNo ratings yet
- A Study of Use of "PORT" Catheter in Patients With Cancer: A Single-Center ExperienceDocument6 pagesA Study of Use of "PORT" Catheter in Patients With Cancer: A Single-Center ExperienceLydia AmaliaNo ratings yet
- Assessment of Adverse Events and Quality of Life of Cancer Patients in A Secondary Level Care, Rural Hospital in South IndiaDocument4 pagesAssessment of Adverse Events and Quality of Life of Cancer Patients in A Secondary Level Care, Rural Hospital in South IndiaLydia AmaliaNo ratings yet
- Wahlberg2016 2Document8 pagesWahlberg2016 2Lydia AmaliaNo ratings yet
- Aune 2017Document11 pagesAune 2017Lydia AmaliaNo ratings yet
- Butler 2015Document8 pagesButler 2015Lydia AmaliaNo ratings yet
- Kuretase Case Report 2Document3 pagesKuretase Case Report 2Lydia AmaliaNo ratings yet
- Price List BopiDocument4 pagesPrice List BopiRiffi doressonNo ratings yet
- STUDY DESIGNS-for PPT Use OnlyDocument4 pagesSTUDY DESIGNS-for PPT Use OnlyEricka GenoveNo ratings yet
- Pgmee Test Series For Neet & Aiims: WWW - Aim4Aiims - In/Pg +91-7529938911Document74 pagesPgmee Test Series For Neet & Aiims: WWW - Aim4Aiims - In/Pg +91-7529938911salamredNo ratings yet
- Mental Status ExaminationDocument13 pagesMental Status ExaminationJosé Ramón Pérez-Accino100% (1)
- NipedipinDocument4 pagesNipedipindesty sanzNo ratings yet
- CHN Ratio Test 2022Document12 pagesCHN Ratio Test 2022Arvinjohn GacutanNo ratings yet
- Care Plan PresentationDocument15 pagesCare Plan Presentationapi-307590979No ratings yet
- Benign Bone Tumours LectureDocument11 pagesBenign Bone Tumours Lecturekyliever100% (1)
- Emergency and Disaster NursingDocument19 pagesEmergency and Disaster NursingNina Oaip100% (1)
- Faktor-Faktor Yang Mempengaruhi Tuberculosis Multidrug Resistance (TB MDR)Document9 pagesFaktor-Faktor Yang Mempengaruhi Tuberculosis Multidrug Resistance (TB MDR)Dian RohmayantiNo ratings yet
- BotulismDocument5 pagesBotulismsubhash nayakNo ratings yet
- National TB GuidelineDocument70 pagesNational TB Guidelinezvkznhsw2tNo ratings yet
- Pe1 - Week 3Document23 pagesPe1 - Week 3Norman NarbonitaNo ratings yet
- EVITDocument1 pageEVITAshutosh RaiNo ratings yet
- ACS NSTEMI Clinical PathwayDocument3 pagesACS NSTEMI Clinical PathwayXtiaRNo ratings yet
- Connect Simplicity SchemeDocument4 pagesConnect Simplicity SchemeRajarajeshwari KommuNo ratings yet
- Risk Factors For Speech Disorders in Children: A. V. Fox, Barbara Dodd and David HowardDocument15 pagesRisk Factors For Speech Disorders in Children: A. V. Fox, Barbara Dodd and David HowardRaul Morales VillegasNo ratings yet
- The Child With Alterations in Activity Exercise PatternsDocument6 pagesThe Child With Alterations in Activity Exercise PatternsBg NatzzNo ratings yet
- Joana Marie E. Gantuangco: Harrison's 20th EditionDocument27 pagesJoana Marie E. Gantuangco: Harrison's 20th EditionJoana Marie Gantuangco-MaglinteNo ratings yet
- I - Clinical ExamDocument63 pagesI - Clinical ExamMadi LazarNo ratings yet
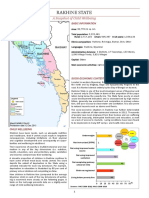
- Rakhine State: A Snapshot of Child WellbeingDocument4 pagesRakhine State: A Snapshot of Child Wellbeingmarcmyomyint1663No ratings yet
- Drug StudyDocument2 pagesDrug StudySavannah KhrisNo ratings yet
- A Study To Assess The Effectiveness of Structured Teaching Programme On Prevention of Polycystic Ovarian Disease Among Adolescent Girls in Selected Intermediate College at LucknowDocument4 pagesA Study To Assess The Effectiveness of Structured Teaching Programme On Prevention of Polycystic Ovarian Disease Among Adolescent Girls in Selected Intermediate College at LucknowEditor IJTSRDNo ratings yet
- Questions and Answers On Benzyl Alcohol Used As An Excipient in Medicinal Products For Human UseDocument8 pagesQuestions and Answers On Benzyl Alcohol Used As An Excipient in Medicinal Products For Human Usemayra chipanaNo ratings yet
- 2009432Document32 pages2009432Luis Alberto Letona QuispeNo ratings yet
- Roams 2 Review of All Medical Subjects Pdfdrivecom PDF PDF FreeDocument5 pagesRoams 2 Review of All Medical Subjects Pdfdrivecom PDF PDF FreeBiswajitNo ratings yet
- 3.casual or Causal Relationship Between Periodontal Infection and Non Oral DiseaseDocument3 pages3.casual or Causal Relationship Between Periodontal Infection and Non Oral DiseaseEstherNo ratings yet
- What Is Chronic Venous Insufficiency (CVI) ?Document2 pagesWhat Is Chronic Venous Insufficiency (CVI) ?atika5No ratings yet