0% found this document useful (0 votes)
96 views4 pagesMyocardial Infarction NCLEX Review Guide
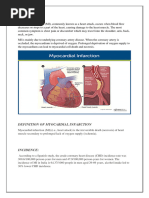
This document provides an overview of myocardial infarction (MI), also known as a heart attack. It defines MI as heart muscle tissue dying due to decreased blood flow, usually from a blockage in a coronary artery. Common causes of blockages are coronary artery disease and illicit drug use. The left anterior descending artery is often the site of blockages due to supplying critical areas of the heart. Signs and symptoms of an MI include chest pain and elevated cardiac enzyme levels. Treatment involves medications to reduce clotting and open arteries, as well as lifestyle changes to prevent future heart attacks.
Uploaded by
lhenCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as PDF, TXT or read online on Scribd
0% found this document useful (0 votes)
96 views4 pagesMyocardial Infarction NCLEX Review Guide
This document provides an overview of myocardial infarction (MI), also known as a heart attack. It defines MI as heart muscle tissue dying due to decreased blood flow, usually from a blockage in a coronary artery. Common causes of blockages are coronary artery disease and illicit drug use. The left anterior descending artery is often the site of blockages due to supplying critical areas of the heart. Signs and symptoms of an MI include chest pain and elevated cardiac enzyme levels. Treatment involves medications to reduce clotting and open arteries, as well as lifestyle changes to prevent future heart attacks.
Uploaded by
lhenCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as PDF, TXT or read online on Scribd