Stroke
Stroke
Download as pdf or txt
You might also like
- Orthopedic Inpatient Protocols: A Guide to Orthopedic Inpatient RoundingFrom EverandOrthopedic Inpatient Protocols: A Guide to Orthopedic Inpatient RoundingNo ratings yet
- Nurse Bob's MICU/CCU Survival Guide Critical Care Concepts General Nursing Requirements of The Intensive Care PatientDocument7 pagesNurse Bob's MICU/CCU Survival Guide Critical Care Concepts General Nursing Requirements of The Intensive Care Patientlil' princessNo ratings yet
- Conscious Sedation StandardsDocument43 pagesConscious Sedation StandardsGhaleb Nasrallah95% (22)
- Nclex ReviewerDocument108 pagesNclex ReviewerKatrina Blancaver Nopuente100% (12)
- Ineffective Cerebral Tissue PerfusionDocument3 pagesIneffective Cerebral Tissue PerfusionHanya Bint Potawan88% (25)
- Hina J. Talib (Eds.) - Adolescent Gynecology - A Clinical Casebook-Springer International Publishing (2018) PDFDocument281 pagesHina J. Talib (Eds.) - Adolescent Gynecology - A Clinical Casebook-Springer International Publishing (2018) PDFsalah subbah100% (1)
- Stroke PPT Nursing Care New EvidencesDocument41 pagesStroke PPT Nursing Care New EvidencesrajniNo ratings yet
- Anaesthesia Clerkship HandbookDocument12 pagesAnaesthesia Clerkship HandbookKay BristolNo ratings yet
- Dzino's SurgeryDocument718 pagesDzino's SurgeryHuram SeremaniNo ratings yet
- Management of Medically Compromised PatientsDocument31 pagesManagement of Medically Compromised PatientsRiyashi ChandaNo ratings yet
- Truma Sllide 3Document22 pagesTruma Sllide 3adnanreshunNo ratings yet
- Guidelines For The Management of Acute Stroke: Emergency DepartmentDocument10 pagesGuidelines For The Management of Acute Stroke: Emergency DepartmentUhuebor DavidNo ratings yet
- Ischemic Stroke ManagementDocument8 pagesIschemic Stroke ManagementBa LitNo ratings yet
- SP50 Cardiac Stress-Exercise Testing (Adult, Peds)Document8 pagesSP50 Cardiac Stress-Exercise Testing (Adult, Peds)Sonu JacobNo ratings yet
- Chapter 3: Perioperative ManagementDocument14 pagesChapter 3: Perioperative ManagementpoddataNo ratings yet
- 062 Cerebral-Challenge 5 Update 2011 PDFDocument5 pages062 Cerebral-Challenge 5 Update 2011 PDFcignalNo ratings yet
- Assessment and Management of The Unconscious PatientDocument6 pagesAssessment and Management of The Unconscious PatientRed DevilNo ratings yet
- Induction of AnaesthesiaDocument6 pagesInduction of Anaesthesiaapi-142637023No ratings yet
- Monitoring & Devices Used in ICU CCUDocument48 pagesMonitoring & Devices Used in ICU CCUProf. Ramsharan Mehta100% (3)
- BCM 229 General Consideration in AnesthesiaDocument11 pagesBCM 229 General Consideration in AnesthesiaTechnoveNo ratings yet
- National Stroke Thrombolysis Guideline Template v9 5-12-13 FINAL 2Document15 pagesNational Stroke Thrombolysis Guideline Template v9 5-12-13 FINAL 2Muhammad FauziNo ratings yet
- SP8 Lumbar PunctureDocument5 pagesSP8 Lumbar PunctureAgeng RestiNo ratings yet
- Procedural AnesthesiaDocument40 pagesProcedural AnesthesiaHaris TanNo ratings yet
- Uhns Guidelines 2010Document187 pagesUhns Guidelines 2010varrakesh100% (1)
- Procedural AnesthesiaDocument40 pagesProcedural AnesthesiaJovian LutfiNo ratings yet
- Neuro-Critical Care For Acute Ischemic Stroke: Daniel Akhavan, MD, FCCPDocument28 pagesNeuro-Critical Care For Acute Ischemic Stroke: Daniel Akhavan, MD, FCCPGita WardhaniNo ratings yet
- Cardio Pulmonary ResuscitationDocument12 pagesCardio Pulmonary Resuscitationalpana.rajput87No ratings yet
- Special Circumstances GuidelinesDocument19 pagesSpecial Circumstances GuidelinesRayNo ratings yet
- The Preoperative EvaluationDocument25 pagesThe Preoperative Evaluationnormie littlemonsterNo ratings yet
- Unit 6Document51 pagesUnit 6Elsemieke SiemonsmaNo ratings yet
- Lumber PunctureDocument8 pagesLumber PunctureInam KhanNo ratings yet
- Using The ACLS Primary Survey For A Patient in Respiratory ArrestDocument34 pagesUsing The ACLS Primary Survey For A Patient in Respiratory Arrest강기연100% (1)
- Management of Medically Compromised PatientsDocument32 pagesManagement of Medically Compromised PatientssnigxrtNo ratings yet
- ACLS II Sept 25 StudentsDocument60 pagesACLS II Sept 25 StudentsLex CatNo ratings yet
- Special Circumstances Guidelines ALSDocument19 pagesSpecial Circumstances Guidelines ALSHamzaMasoodNo ratings yet
- Postoperative PhaseDocument8 pagesPostoperative PhasereymarhayNo ratings yet
- General ProtocolDocument7 pagesGeneral ProtocolAbdella UmerNo ratings yet
- Management of Cardiac and Peptic Ulcer PatientDocument13 pagesManagement of Cardiac and Peptic Ulcer Patientwajiha sheikhNo ratings yet
- SKILL STATION Management of Critically Ill Patient With Septic Shock Provider GuideDocument27 pagesSKILL STATION Management of Critically Ill Patient With Septic Shock Provider GuidesrinidhiNo ratings yet
- Penatalaksanaan StrokeDocument15 pagesPenatalaksanaan StrokerizeviNo ratings yet
- Purpose: CVA (Stroke) Patients (Ischemic and Hemorrhagic), Management ofDocument4 pagesPurpose: CVA (Stroke) Patients (Ischemic and Hemorrhagic), Management ofRoxanne AlvarezNo ratings yet
- ERCP Procedure GuideDocument7 pagesERCP Procedure GuideFachrur Rodji100% (1)
- Anaes Tutorial 1 - DR - MungrooDocument8 pagesAnaes Tutorial 1 - DR - MungrooChris DwarikaNo ratings yet
- Online LectureDocument9 pagesOnline LectureJobelle AcenaNo ratings yet
- Acute MX of StrokeDocument23 pagesAcute MX of StrokeAshish GuragainNo ratings yet
- Primary and Secondary SurveyDocument7 pagesPrimary and Secondary Surveyandila.muhammad20No ratings yet
- Trauma and Emergency NursingDocument9 pagesTrauma and Emergency Nursingchinthaka18389021No ratings yet
- Politrauma - Rolul AtiDocument18 pagesPolitrauma - Rolul AtiChirita ElenaNo ratings yet
- Anaesthesia For Trauma PatientsDocument42 pagesAnaesthesia For Trauma PatientsMerindukan Surga MuNo ratings yet
- Periodontics يرﻛﺷ ﺎﮭﻣ د: Periodontal management of medically compromised patientsDocument8 pagesPeriodontics يرﻛﺷ ﺎﮭﻣ د: Periodontal management of medically compromised patientsYehya Al KhashabNo ratings yet
- ABC ResuscitationDocument5 pagesABC ResuscitationIamTineshNo ratings yet
- Code Blue Free For EveryoneDocument93 pagesCode Blue Free For EveryonedindaNo ratings yet
- Module 1 - Acute Ischemic StrokeDocument51 pagesModule 1 - Acute Ischemic StrokeRick RanitNo ratings yet
- Sedation in Critically IllDocument32 pagesSedation in Critically IllSamantha Deshapriya100% (2)
- Traumatic ShockDocument22 pagesTraumatic ShockOlga GoryachevaNo ratings yet
- Activating A Stroke Alert - A Neurological Emergency - CE591Document7 pagesActivating A Stroke Alert - A Neurological Emergency - CE591Czar Julius Malasaga100% (1)
- VF PediDocument6 pagesVF PedixiphoideusNo ratings yet
- Ambulatory Management of Myocardial Infarction at First HourDocument33 pagesAmbulatory Management of Myocardial Infarction at First HourDr Gaurav SinghNo ratings yet
- Clinical case in the emergency room of a patient with an ischemic strokeFrom EverandClinical case in the emergency room of a patient with an ischemic strokeNo ratings yet
- Compiled by Hapc' in Association With Icf Hospital' Compiled by Hapc' in Association With Icf Hospital'Document1 pageCompiled by Hapc' in Association With Icf Hospital' Compiled by Hapc' in Association With Icf Hospital'Chellamani UmakanthanNo ratings yet
- Compiled by Hapc' in Association With Icf Hospital' Compiled by Hapc' in Association With Icf Hospital'Document1 pageCompiled by Hapc' in Association With Icf Hospital' Compiled by Hapc' in Association With Icf Hospital'Chellamani UmakanthanNo ratings yet
- Compiled by Hapc' in Association With Icf Hospital' Compiled by Hapc' in Association With Icf Hospital'Document1 pageCompiled by Hapc' in Association With Icf Hospital' Compiled by Hapc' in Association With Icf Hospital'Chellamani UmakanthanNo ratings yet
- Compiled by Hapc' in Association With Icf Hospital' Compiled by Hapc' in Association With Icf Hospital'Document1 pageCompiled by Hapc' in Association With Icf Hospital' Compiled by Hapc' in Association With Icf Hospital'Chellamani UmakanthanNo ratings yet
- Compiled by Hapc' in Association With Icf Hospital' Compiled by Hapc' in Association With Icf Hospital'Document1 pageCompiled by Hapc' in Association With Icf Hospital' Compiled by Hapc' in Association With Icf Hospital'Chellamani UmakanthanNo ratings yet
- Sterilization ProtocolDocument6 pagesSterilization ProtocolChellamani UmakanthanNo ratings yet
- Abdominal PainDocument16 pagesAbdominal PainSumit KhetarpalNo ratings yet
- Casualty ProtocolDocument89 pagesCasualty ProtocolChellamani UmakanthanNo ratings yet
- Sterilization ProtocolDocument6 pagesSterilization ProtocolChellamani UmakanthanNo ratings yet
- HTTPDocument1 pageHTTPChellamani UmakanthanNo ratings yet
- Ecg Reporting: The Atria Normal AtriaDocument5 pagesEcg Reporting: The Atria Normal AtriaChellamani UmakanthanNo ratings yet
- Eye ExaminationDocument6 pagesEye ExaminationChellamani UmakanthanNo ratings yet
- Guidelines For Management of Head InjuryDocument18 pagesGuidelines For Management of Head InjuryChellamani UmakanthanNo ratings yet
- New Doc 2019-03-30 09.46.15Document1 pageNew Doc 2019-03-30 09.46.15Chellamani UmakanthanNo ratings yet
- Notification Admit Card Results Exam AnalysisDocument10 pagesNotification Admit Card Results Exam AnalysisChellamani UmakanthanNo ratings yet
- CardiomegalyDocument6 pagesCardiomegalyChellamani UmakanthanNo ratings yet
- Self-Compassion in Clinical PracticeDocument13 pagesSelf-Compassion in Clinical PracticeMircea PocolNo ratings yet
- Alcohol Treatment CodesDocument3 pagesAlcohol Treatment CodesMia JacksonNo ratings yet
- Sentinel Lymph Node (SLN) Biopsy PDFDocument5 pagesSentinel Lymph Node (SLN) Biopsy PDFMDNo ratings yet
- Ivac Ayurveda HandbookDocument24 pagesIvac Ayurveda HandbookfeefaldemahNo ratings yet
- Kelly Wilson ACT Substance AbuseDocument22 pagesKelly Wilson ACT Substance AbuseAnonymous Ax12P2srNo ratings yet
- PhobiasDocument10 pagesPhobiasapi-276690632No ratings yet
- Get Rid of Dark Spots - The Power of Homeopathy For Pigmentation - Schwabe IndiaDocument11 pagesGet Rid of Dark Spots - The Power of Homeopathy For Pigmentation - Schwabe Indianadee.ak2023No ratings yet
- Sport Science and Sports Medicine Framework 2017 v1Document31 pagesSport Science and Sports Medicine Framework 2017 v1api-443327549No ratings yet
- Application PDF FormatDocument13 pagesApplication PDF FormatnokulungalebzamNo ratings yet
- Altering Occlusal Vertical Dimension in FunctionalDocument8 pagesAltering Occlusal Vertical Dimension in FunctionalDavid ColonNo ratings yet
- 5 Biopharmaceutic Considerations of A Drug DesignDocument89 pages5 Biopharmaceutic Considerations of A Drug DesignImDanaBananaaaNo ratings yet
- Depression in Older Adults.21Document9 pagesDepression in Older Adults.21April Mae Balatibat LapueblaNo ratings yet
- AsthmaDocument46 pagesAsthmaHafiz Muhammad Aeymon100% (1)
- Adlerian Family TherapyDocument24 pagesAdlerian Family Therapynurakbulut100% (3)
- The Use of Barium Sulfate For Implant TemplatesDocument4 pagesThe Use of Barium Sulfate For Implant TemplatesFreddy GarciaNo ratings yet
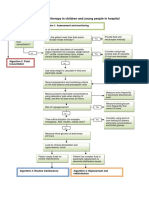
- Algorithms For IV Fluid Therapy in Children and Young People in Hospital Set of 6 PDF 2190274957 PDFDocument6 pagesAlgorithms For IV Fluid Therapy in Children and Young People in Hospital Set of 6 PDF 2190274957 PDFFurqon AfandriNo ratings yet
- Shockwave Treatment For Denerved MuscleDocument6 pagesShockwave Treatment For Denerved MuscleMauricio PinalNo ratings yet
- ChecklistDocument2 pagesChecklistRuzi Falahi KautsarNo ratings yet
- Streptococcus AgalactiaeDocument16 pagesStreptococcus Agalactiaeapi-232630489No ratings yet
- Chap 02 - Set 3Document7 pagesChap 02 - Set 3Khor Han YiNo ratings yet
- Rebt DepressionDocument31 pagesRebt DepressionAlina Macavei100% (1)
- TriageDocument27 pagesTriageDanette Mae RocNo ratings yet
- Iacobo TxplanningpaperDocument11 pagesIacobo Txplanningpaperapi-524151719No ratings yet
- The Good Doctor S01E02Document59 pagesThe Good Doctor S01E02Algorithove AlgorithoveNo ratings yet
- Greetings: Pushpagiri College of Dental SciencesDocument27 pagesGreetings: Pushpagiri College of Dental SciencesDilu DavisNo ratings yet
- Reversal and Alternating Treatments Designs: Cooper, Heron, and Heward All Rights ReservedDocument22 pagesReversal and Alternating Treatments Designs: Cooper, Heron, and Heward All Rights ReservedSantiagoTrujilloLemus100% (1)
- Cell Sept 2011Document201 pagesCell Sept 2011mekkararameshNo ratings yet
- Unlock 2-3 Revision TestDocument2 pagesUnlock 2-3 Revision TestDeniz FerahNo ratings yet