Pengkajian Modul 6 Materi English
Pengkajian Modul 6 Materi English
Download as doc, pdf, or txt
You might also like
- The Incredible Journey by Burnford SheilaDocument51 pagesThe Incredible Journey by Burnford Sheilabah50% (2)
- Nursing Health HistoryDocument11 pagesNursing Health Historyrubycorazon_edizaNo ratings yet
- Health AssessmentDocument28 pagesHealth AssessmentPiyush Dutta100% (2)
- Physical Assessment Exam Study Guide Final DraftDocument39 pagesPhysical Assessment Exam Study Guide Final DraftNicky Cranford89% (18)
- Step 3 Board-Ready USMLE Junkies 2nd Edition: The Must-Have USMLE Step 3 Review CompanionFrom EverandStep 3 Board-Ready USMLE Junkies 2nd Edition: The Must-Have USMLE Step 3 Review CompanionNo ratings yet
- Physical AssessmentDocument66 pagesPhysical AssessmentShyvonne Elisan LosariaNo ratings yet
- Gruop 4 EnglishDocument13 pagesGruop 4 Englishindah kurniaNo ratings yet
- Nursing Process Care PlanningDocument10 pagesNursing Process Care Planningogunbiyiolajumoke4No ratings yet
- Physical AssessmenDocument3 pagesPhysical AssessmenJohn Lawrence Fernandez EboNo ratings yet
- Health Assessment AssignmentDocument15 pagesHealth Assessment Assignmentpslokesha84100% (1)
- (Tugas) Pyhsical ExaminationDocument11 pages(Tugas) Pyhsical ExaminationDewi NurpitasariNo ratings yet
- Fon 2Document36 pagesFon 2chelsea pasiahNo ratings yet
- Topic 2-6 Introduction To Physical AssessmentDocument16 pagesTopic 2-6 Introduction To Physical Assessmentnaayao100% (1)
- History Taking and Interview SkillsDocument63 pagesHistory Taking and Interview Skillsroama3359No ratings yet
- 1. Assessment NCPDocument82 pages1. Assessment NCPNeil MasongsongNo ratings yet
- Health Assessment: by Dr. Hala YehiaDocument115 pagesHealth Assessment: by Dr. Hala YehiaRazaCreciaLastrillaMenesesNo ratings yet
- Assessment: Stikes Madani YogyakartaDocument37 pagesAssessment: Stikes Madani YogyakartaSintalia DewiNo ratings yet
- Health AssessmentDocument15 pagesHealth Assessmentmeghana100% (1)
- Makalah KEL 1. BAHASA INGGRISDocument13 pagesMakalah KEL 1. BAHASA INGGRISMuhammad PanduNo ratings yet
- Physical Health AssessmentDocument31 pagesPhysical Health Assessmentpreeti.13isNo ratings yet
- Health AssessmentDocument24 pagesHealth Assessmentjee2024maitriNo ratings yet
- FundamentalsDocument126 pagesFundamentalsFull ErosNo ratings yet
- Health AssessmentDocument14 pagesHealth AssessmentLakshmi RjNo ratings yet
- Health AssessmentDocument31 pagesHealth AssessmentLoi Ocampo Crespo100% (1)
- Ha NotesDocument39 pagesHa NotesGlecy Ann MagnoNo ratings yet
- Health Assessment Intro, Nsg. Process, Interviwe, RosDocument216 pagesHealth Assessment Intro, Nsg. Process, Interviwe, RosHyacinth Jane Dela PeñaNo ratings yet
- The Health Care Process: April T. CajandigDocument26 pagesThe Health Care Process: April T. CajandigIra Louise Paraguya ParejaNo ratings yet
- Nursing Process QuestionsDocument12 pagesNursing Process QuestionsSritama Ghosh100% (2)
- Nursing Process 2Document95 pagesNursing Process 2Chippy SinghNo ratings yet
- Health Assessment by BaniDocument10 pagesHealth Assessment by BaniSujata Mishra100% (1)
- Physical Assessment Exam Study GuideDocument55 pagesPhysical Assessment Exam Study GuideApRil Anne Balanon100% (1)
- UNIT-I Introduction and Components of Health AssementDocument37 pagesUNIT-I Introduction and Components of Health Assementraima ayazNo ratings yet
- Nursing Process PresentationDocument67 pagesNursing Process PresentationAr-jay JubaneNo ratings yet
- PPTDocument11 pagesPPTVina NovitaNo ratings yet
- Fundamental in Nursing-Assessment Objective & Subjective DataDocument5 pagesFundamental in Nursing-Assessment Objective & Subjective DataarzooNo ratings yet
- Midterm ExamDocument4 pagesMidterm ExamFranzelle Estrella ÜNo ratings yet
- Nursing ProcessDocument5 pagesNursing Processanimesh pandaNo ratings yet
- اساسيات تمريضDocument38 pagesاساسيات تمريضHamza WeshahNo ratings yet
- Presentation On Health AssessmentDocument12 pagesPresentation On Health AssessmentSimran ChauhanNo ratings yet
- Nursing ProcessDocument9 pagesNursing ProcessJeffrey Valdez EsteronNo ratings yet
- Definition of NursingDocument28 pagesDefinition of NursingamiranabilelshazlyNo ratings yet
- Uni 2 Nursing ProcessDocument59 pagesUni 2 Nursing ProcessDoraemonNo ratings yet
- Nurs Assessment 1Document14 pagesNurs Assessment 1Putri Nandani AlifahNo ratings yet
- HA Lec Reporting LATESTDocument12 pagesHA Lec Reporting LATESTErwin MarceloNo ratings yet
- G. The Nursing ProcessDocument83 pagesG. The Nursing Processemma rose lutellaNo ratings yet
- Clinical Exam HTT Focused Assessment STUDENTDocument23 pagesClinical Exam HTT Focused Assessment STUDENTtavakol akbarimehmandostiNo ratings yet
- Nursing Process - Assessment - D3Document3 pagesNursing Process - Assessment - D3Claras VinarNo ratings yet
- NCM 101jDocument93 pagesNCM 101jRada JulailiNo ratings yet
- Remember: Goals and Plan of Care Should Be Base According To Client's Problems/needs NOT According To Your OwnDocument11 pagesRemember: Goals and Plan of Care Should Be Base According To Client's Problems/needs NOT According To Your Ownavinash dhameriyaNo ratings yet
- W1 Nursing ProcessDocument18 pagesW1 Nursing ProcessColeen Tan100% (1)
- Introduction To Nursing Process (NP) : Presenter:M.Salman Alam Nursing Instructor, RCN Acknowledgement: FON TeamDocument51 pagesIntroduction To Nursing Process (NP) : Presenter:M.Salman Alam Nursing Instructor, RCN Acknowledgement: FON TeamSaqlain M.No ratings yet
- Nursing ProcessDocument16 pagesNursing Processabdo mo . M7.No ratings yet
- Nursing Assessment: Mr.G.Harsha Nursing officer-AIIMS MangalagiriDocument52 pagesNursing Assessment: Mr.G.Harsha Nursing officer-AIIMS Mangalagirilakkki143No ratings yet
- Nursing Process: MRSCH - Lavanya M.Sc. (N) Associate Professor Gitam Institute of Nursing GitamDocument83 pagesNursing Process: MRSCH - Lavanya M.Sc. (N) Associate Professor Gitam Institute of Nursing GitamLavanya ChNo ratings yet
- Nursing ProcessDocument114 pagesNursing ProcessTrisha Mae BalladNo ratings yet
- History TakingDocument4 pagesHistory Takingabdulmarwat88No ratings yet
- Health Assessment in NursingDocument58 pagesHealth Assessment in NursingCj MayoyoNo ratings yet
- Lab Values: An Easy Guide to Learn Everything You Need to Know About Laboratory Medicine and Its Relevance in Diagnosing DiseaseFrom EverandLab Values: An Easy Guide to Learn Everything You Need to Know About Laboratory Medicine and Its Relevance in Diagnosing DiseaseRating: 4.5 out of 5 stars4.5/5 (3)
- Physician Assistant PANCE & PANRE: a QuickStudy Laminated Reference GuideFrom EverandPhysician Assistant PANCE & PANRE: a QuickStudy Laminated Reference GuideNo ratings yet
- 111 Veterinary Gross Anatomy - I (Osteology, Arthrology & Biomechanics)Document161 pages111 Veterinary Gross Anatomy - I (Osteology, Arthrology & Biomechanics)Vaidika YadavNo ratings yet
- Dutch Oven RecipesDocument133 pagesDutch Oven RecipesskycrateNo ratings yet
- $R46MVGODocument3 pages$R46MVGOJustin CallNo ratings yet
- WHO - Guidelines On Establishment of Virology LaboratoryDocument79 pagesWHO - Guidelines On Establishment of Virology LaboratoryAjeng MutvakadwiaNo ratings yet
- Chapter 17 BloodDocument10 pagesChapter 17 BloodTony SnearlyNo ratings yet
- Study of Children With AerophagiaDocument7 pagesStudy of Children With AerophagiajmccoyNo ratings yet
- MLG 4Document20 pagesMLG 4GS ShawonNo ratings yet
- LunchmenuDocument14 pagesLunchmenueatlocalmenusNo ratings yet
- Eye Dissection Report Write Up 2014Document8 pagesEye Dissection Report Write Up 2014api-351895935No ratings yet
- Influenza VirusDocument28 pagesInfluenza VirusDave Despabiladeras100% (2)
- Libris Mortis 5e - SpellsDocument7 pagesLibris Mortis 5e - SpellsLuke FreemanNo ratings yet
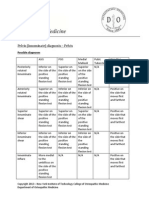
- Pelvis (Innominate) Diagnosis - Pelvis: Possible DiagnosesDocument4 pagesPelvis (Innominate) Diagnosis - Pelvis: Possible DiagnosesMjidKarimNo ratings yet
- Msds Kloroform)Document6 pagesMsds Kloroform)Muhammad SaprizalNo ratings yet
- Pointers To Review (Gen Bio 2)Document5 pagesPointers To Review (Gen Bio 2)jayrald cruzadaNo ratings yet
- Enquiry Metamorphosis Week 6Document25 pagesEnquiry Metamorphosis Week 6sireane123No ratings yet
- Grade 6 English Self Study PackDocument95 pagesGrade 6 English Self Study PackWathsala GunarathnaNo ratings yet
- English LBDocument10 pagesEnglish LBmuskaan.kukrejaNo ratings yet
- Travel Opticons in 5eDocument7 pagesTravel Opticons in 5eFedericoPironiNo ratings yet
- The Following Text Is For Questions No. 1 and 2Document11 pagesThe Following Text Is For Questions No. 1 and 2Ardhiansyah Ilmostro WijayaNo ratings yet
- 500 Best-Ever Recipes Appetizers PDFDocument7 pages500 Best-Ever Recipes Appetizers PDFENACHE GEORGETANo ratings yet
- A Practical Approach To Hemodialysis For Canine Renal DiseaseDocument8 pagesA Practical Approach To Hemodialysis For Canine Renal Diseaseaniel_bmNo ratings yet
- Lampiran 1 Tensimeter Digital Non Invasive Blood Pressure: Coda Kent Scientific CorporationDocument11 pagesLampiran 1 Tensimeter Digital Non Invasive Blood Pressure: Coda Kent Scientific Corporationdimas gilang prakosoNo ratings yet
- GiraffeDocument2 pagesGiraffeDogie FacdoNo ratings yet
- Beef Breeds and Their Functional TypesDocument6 pagesBeef Breeds and Their Functional TypesPegNo ratings yet
- Wakifa and Soophumore .2023pdfDocument16 pagesWakifa and Soophumore .2023pdfMohammed JundiNo ratings yet
- 2.1 Gas Exchange in HumansDocument61 pages2.1 Gas Exchange in HumansTAN SHI LE CHARLOTTENo ratings yet
- Uzair KhiljiDocument9 pagesUzair KhiljitanvirNo ratings yet
- Indoors Natural Substrates For Elephants & Medical Issues Associated With Hard SurfacesDocument13 pagesIndoors Natural Substrates For Elephants & Medical Issues Associated With Hard SurfacesCoraKiriNo ratings yet
- 13850bio Guess PaperDocument10 pages13850bio Guess PaperJayaram GowdaNo ratings yet