The Head: HEENT: Techniques of Examination
The Head: HEENT: Techniques of Examination
Download as docx, pdf, or txt
You might also like
- Review of Systems (Bates' Super-Long Version)Document3 pagesReview of Systems (Bates' Super-Long Version)jmosser98% (47)
- Essential Notes in Pain MedicineDocument737 pagesEssential Notes in Pain MedicineRichard Pertwee100% (7)
- NR 509 APEA 3P Final Exam Study GuideDocument11 pagesNR 509 APEA 3P Final Exam Study GuideChristine Villamayor100% (5)
- SOAP Note Cheat Sheet - Complete H&PDocument2 pagesSOAP Note Cheat Sheet - Complete H&PAdeline N. Omene95% (19)
- Obgyn Soap Note ExampleDocument2 pagesObgyn Soap Note ExampleBluerobins94% (33)
- HEENT ExamDocument7 pagesHEENT Examnz0ptkNo ratings yet
- Physical Exam ChecklistDocument1 pagePhysical Exam ChecklistLaura Hernandez100% (5)
- Adult Medical SOAP NoteDocument4 pagesAdult Medical SOAP NoteBhanu100% (7)
- Head To Toe Physical Assessment ChecklistDocument16 pagesHead To Toe Physical Assessment ChecklistMichael Allen Fadriquel100% (12)
- Final Assessment Soap NoteDocument13 pagesFinal Assessment Soap Noteapi-494643478100% (3)
- Grand Osce ReviewerDocument16 pagesGrand Osce ReviewerBA Ong100% (1)
- DXR Harrelson SoapDocument4 pagesDXR Harrelson SoapAlexanderWarrenNo ratings yet
- ANCC Crash - Course - Study - Guide - 1Document76 pagesANCC Crash - Course - Study - Guide - 1Anjel JonesNo ratings yet
- Soap Note2Document6 pagesSoap Note2jessica100% (5)
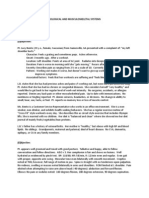
- Soap Note - Musculoskeletal and Nervous SystemsDocument2 pagesSoap Note - Musculoskeletal and Nervous SystemsSummer Keller89% (9)
- List of Medical Triads and Pentads - WikipediaDocument3 pagesList of Medical Triads and Pentads - WikipediaSubhajitPaul100% (1)
- MnemonicsDocument4 pagesMnemonicsLheidaniel MMM.100% (2)
- Nurse Practitioner Board ReviewFrom EverandNurse Practitioner Board ReviewRating: 5 out of 5 stars5/5 (1)
- APEA 3P Question Bank With AnswersDocument10 pagesAPEA 3P Question Bank With AnswersOleg Knaz100% (1)
- Physical Examination ChecklistDocument5 pagesPhysical Examination Checklistsamhie21No ratings yet
- Adult History Taking and Physical ExaminationDocument6 pagesAdult History Taking and Physical ExaminationDoc Prince Caballero100% (3)
- Physical Exam & Interview ChecklistDocument7 pagesPhysical Exam & Interview Checklistjmosser100% (6)
- The Comprehensive Adult Health History and Physical ExaminationDocument8 pagesThe Comprehensive Adult Health History and Physical ExaminationJoseph HernandezNo ratings yet
- Physical Assessment Guide of Head-To-ToeDocument9 pagesPhysical Assessment Guide of Head-To-Toeneleh gray100% (2)
- Dermatitis SOAP NOTEDocument10 pagesDermatitis SOAP NOTEHugs100% (2)
- Peds EORDocument17 pagesPeds EORRachel BarrosNo ratings yet
- SOAP Note DiabetesDocument16 pagesSOAP Note Diabetesmichael thorn92% (25)
- Components of The Adult Health HistoryDocument8 pagesComponents of The Adult Health HistoryCarol Neng CalupitanNo ratings yet
- Ipd B: Finals - Heent: Techniques of Examination For Head (From Bates')Document13 pagesIpd B: Finals - Heent: Techniques of Examination For Head (From Bates')Janica Marie Ragsac100% (2)
- Complete Physical Examination ChecklistDocument5 pagesComplete Physical Examination Checklistapi-641836481No ratings yet
- LWW BATES 13 Abdomen Transcript FINALDocument6 pagesLWW BATES 13 Abdomen Transcript FINALmuhammad Babar50% (2)
- Complete Guide To Physical ExamDocument19 pagesComplete Guide To Physical ExamSeff Causapin100% (2)
- SOAP For Upper Respiratory Infection #4Document3 pagesSOAP For Upper Respiratory Infection #4carlos fernandezNo ratings yet
- Head To Toe Assessment Guide PDFDocument6 pagesHead To Toe Assessment Guide PDFTasha100% (1)
- APEA QBank AANP Review Latest 2022Document22 pagesAPEA QBank AANP Review Latest 2022Oleg KnazNo ratings yet
- H&P Cheat SheetDocument3 pagesH&P Cheat SheetWilliam YangNo ratings yet
- OBGYN Clinical RotationDocument5 pagesOBGYN Clinical Rotationriczen mae vilaNo ratings yet
- Guide in Reporting Complete Physical Examination (2013) - Source: Bates' Guide To Physical Examination.Document8 pagesGuide in Reporting Complete Physical Examination (2013) - Source: Bates' Guide To Physical Examination.Ernie G. Bautista II, RN, MD100% (6)
- Physical Exam ChecklistDocument2 pagesPhysical Exam ChecklistRaisah Bint Abdullah100% (5)
- Bates Outline of Chapter 8Document15 pagesBates Outline of Chapter 8KatherynSotoNo ratings yet
- Final Check Off Soap NoteDocument4 pagesFinal Check Off Soap Notesana100% (1)
- Suggested Word List For DocumentationDocument1 pageSuggested Word List For Documentationjkbills100% (6)
- SOAP Note Tips and Guidelines For The FNP ProgramDocument6 pagesSOAP Note Tips and Guidelines For The FNP ProgramJosh Bat100% (1)
- Bates Physical Examination RED NOTESDocument2 pagesBates Physical Examination RED NOTESAmanda Gomez100% (1)
- Crash Course Study Guide Master Part 12 1Document92 pagesCrash Course Study Guide Master Part 12 1Lou Escobar100% (1)
- Physical ExaminationDocument7 pagesPhysical ExaminationErwin MirandaNo ratings yet
- 5 - Antibiotics 2018Document11 pages5 - Antibiotics 2018nae100% (3)
- 2Document50 pages2Scott Russell McGillivray100% (1)
- Physical Assessment: Lecturer: Mark Fredderick R. Abejo R.N, M.A.NDocument20 pagesPhysical Assessment: Lecturer: Mark Fredderick R. Abejo R.N, M.A.NRyan Biwit100% (4)
- Thorax and Lungs SGDocument2 pagesThorax and Lungs SGDestinee Caple100% (4)
- n703 Chronic Soap NoteDocument3 pagesn703 Chronic Soap NoteJeffrey ViernesNo ratings yet
- Physical Examination: Binal Joshi Assistant Professor Child Health Nursing Manikaka Topawala Institute of NursingDocument101 pagesPhysical Examination: Binal Joshi Assistant Professor Child Health Nursing Manikaka Topawala Institute of NursingBinal JoshiNo ratings yet
- How To Present Cases (Short File) PDFDocument3 pagesHow To Present Cases (Short File) PDFAmjad SaudNo ratings yet
- Docxshadow Health HistoryDocument4 pagesDocxshadow Health HistoryAlejandro Daniel Landa Morales50% (2)
- Adult Gerontology and FNP p.300-345Document46 pagesAdult Gerontology and FNP p.300-345OMGStudy100% (1)
- Back to Zero: FNP Board Review NotesFrom EverandBack to Zero: FNP Board Review NotesRating: 5 out of 5 stars5/5 (3)
- Problem-based Approach to Gastroenterology and HepatologyFrom EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisNo ratings yet
- Master the Physician Assistant National Recertifying Exam (PANRE)From EverandMaster the Physician Assistant National Recertifying Exam (PANRE)No ratings yet
- Prelim Exam NCM 103Document10 pagesPrelim Exam NCM 103Zhyraine Iraj D. CaluzaNo ratings yet
- Is One of The Oldest and Most Popular Forms of Exercise.: DanceDocument8 pagesIs One of The Oldest and Most Popular Forms of Exercise.: DanceIgorota Sheanne100% (1)
- Formulation of Anti-Plaque Toothpaste Ekstrak GambirDocument8 pagesFormulation of Anti-Plaque Toothpaste Ekstrak GambirNyoman Dewi SaptariNo ratings yet
- Patient Based Pathophysiology of Polycystic Kidney DiseaseeeDocument1 pagePatient Based Pathophysiology of Polycystic Kidney DiseaseeeMarc SorianoNo ratings yet
- InfertilityDocument14 pagesInfertilityDewansh NarangNo ratings yet
- HSB Section B Topic #2 (Coordination & Control)Document20 pagesHSB Section B Topic #2 (Coordination & Control)robertsshuryelleNo ratings yet
- Haloperidol: Brand Name: HaldolDocument15 pagesHaloperidol: Brand Name: Haldolteguh aminNo ratings yet
- Agents Affecting Mineral Ion Homeostasis and Bone TurnoverDocument56 pagesAgents Affecting Mineral Ion Homeostasis and Bone TurnoverSanthosh RajNo ratings yet
- Vitiligo Treated Homoeopathically A Case ReportDocument3 pagesVitiligo Treated Homoeopathically A Case ReportEditor IJTSRDNo ratings yet
- Analize LaboratorDocument2 pagesAnalize LaboratorOana PaduraruNo ratings yet
- RRN 125760 Managing Neonatal Intestinal Obstruction Clinical Perspecti - 020218Document14 pagesRRN 125760 Managing Neonatal Intestinal Obstruction Clinical Perspecti - 020218adkhiatul muslihatinNo ratings yet
- Drug Affecting Cardiovascular FunctionDocument21 pagesDrug Affecting Cardiovascular Functionnurliah armandNo ratings yet
- Ataide,+CR 722 12.DECDocument8 pagesAtaide,+CR 722 12.DECkarinaramos.alunoNo ratings yet
- Skin and PsycheDocument7 pagesSkin and PsycheGeorgios Lerios100% (2)
- MCQ NEURO ANGKATAN 2018, Compiled by JoeyDocument25 pagesMCQ NEURO ANGKATAN 2018, Compiled by JoeyVincent ChristiantoNo ratings yet
- Contrast Agents, Cath Lab & Anaphylatic Shock-ParamedDocument29 pagesContrast Agents, Cath Lab & Anaphylatic Shock-ParamedManikanta Guptha100% (1)
- Twitter: Nurse077 - : Preparation / Abdulrahman Al-Gamdi 0533319252Document21 pagesTwitter: Nurse077 - : Preparation / Abdulrahman Al-Gamdi 0533319252troubleeshooting fileNo ratings yet
- Surgical Case PresentationDocument17 pagesSurgical Case Presentationrishi.rrsbNo ratings yet
- Neuroanatomy Notes 2010 4 PDF FreeDocument33 pagesNeuroanatomy Notes 2010 4 PDF Freepoulenesana1110No ratings yet
- Shelly DKADocument18 pagesShelly DKARizkyastari OnnyNo ratings yet
- Rhinitis & SinusitisDocument44 pagesRhinitis & Sinusitishadeer92.hamdy90No ratings yet
- The Paediatric Voice Clinic: Ian Smillie, Kirsy Mcmanus, Wendy Cohen, Elizabeth Lawson, David Macgregor WynneDocument5 pagesThe Paediatric Voice Clinic: Ian Smillie, Kirsy Mcmanus, Wendy Cohen, Elizabeth Lawson, David Macgregor WynneCarolina UrrutiaNo ratings yet
- Fisiología Nasal, Sistema OlfativoDocument39 pagesFisiología Nasal, Sistema OlfativoJuan Herrera SalazarNo ratings yet
- What Is Osteopenia?: What Are Causes and Risk Factors For Osteopenia?Document2 pagesWhat Is Osteopenia?: What Are Causes and Risk Factors For Osteopenia?Jeremy EvansNo ratings yet
- Pituitary Gland PathologyDocument4 pagesPituitary Gland PathologyGerardLumNo ratings yet
- OB HX and PE GuideDocument5 pagesOB HX and PE GuidePatryk DionisioNo ratings yet
- Basal Cell CarcinomaDocument20 pagesBasal Cell Carcinomaemanuel coatesNo ratings yet
- Radiology MSKDocument110 pagesRadiology MSKFarhanNo ratings yet
- Cellulitis of The Lower Limbs: Incidence, Diagnosis and ManagementDocument4 pagesCellulitis of The Lower Limbs: Incidence, Diagnosis and Managementjenifer paathNo ratings yet