Mello 2016
Mello 2016
Download as pdf or txt
You might also like
- Types of ReduplicationDocument46 pagesTypes of Reduplicationდავით იაკობიძეNo ratings yet
- QlikView in Virtual EnvironmentsDocument4 pagesQlikView in Virtual Environmentspipi das meias0% (1)
- 1 s2.0 S2214139116300026 Main PDFDocument8 pages1 s2.0 S2214139116300026 Main PDFAnonymous T4IxYOoBBGNo ratings yet
- Multiple SclerosisDocument6 pagesMultiple Sclerosisandrearuzzi100% (1)
- Pain AssessentDocument9 pagesPain AssessentJoanna RachelNo ratings yet
- Knowledge and Attitudes of Nurses Regarding Pain in The Intensive Care Unit Pa-Tients in RwandaDocument7 pagesKnowledge and Attitudes of Nurses Regarding Pain in The Intensive Care Unit Pa-Tients in Rwandaibrahim salimNo ratings yet
- Arfan Nursing EducationDocument13 pagesArfan Nursing EducationwahyuningsihhusainNo ratings yet
- Cognitive Behavior Therapy For Patients With Cancer: Sheena Daniels, DNP, Arnp, FNP-BCDocument3 pagesCognitive Behavior Therapy For Patients With Cancer: Sheena Daniels, DNP, Arnp, FNP-BCditeABCNo ratings yet
- Listening Is Therapy Patient Interviewing From A Pain Science PerspectiveDocument13 pagesListening Is Therapy Patient Interviewing From A Pain Science PerspectiveVizaNo ratings yet
- Distress in The Context of Cancer and ChemotherapyDocument14 pagesDistress in The Context of Cancer and ChemotherapyeliaperNo ratings yet
- Cancer ATDocument9 pagesCancer ATBence BakosNo ratings yet
- Lakha2021 Article DemographicsPainCharacteristicDocument14 pagesLakha2021 Article DemographicsPainCharacteristicneurologi standart4No ratings yet
- Valle Rand 2011Document13 pagesValle Rand 2011Azhari BaedlawiNo ratings yet
- a pilot study to compare cognitive behavioral therapy with virtual reality vs. standard cognitive behavioral therapy for patients who suffer from cervical cancerDocument14 pagesa pilot study to compare cognitive behavioral therapy with virtual reality vs. standard cognitive behavioral therapy for patients who suffer from cervical cancersiwar.boudicheNo ratings yet
- Cancer Depre Anx 2º ArtículoDocument12 pagesCancer Depre Anx 2º Artículoalvarogmc02No ratings yet
- Article IjpnDocument6 pagesArticle Ijpndr harrieNo ratings yet
- Pain Management and Assessment by Nurses in Different Wards of A Tertiary Care Hospital in Pakistan eDocument5 pagesPain Management and Assessment by Nurses in Different Wards of A Tertiary Care Hospital in Pakistan eQadri Khalil EmreNo ratings yet
- Mediators, Moderators, and Predictors of Therapeutic Change in Cognitive-Behavioral Therapy For Chronic Pain PDFDocument11 pagesMediators, Moderators, and Predictors of Therapeutic Change in Cognitive-Behavioral Therapy For Chronic Pain PDFRaluca GeorgescuNo ratings yet
- Pain Assessment and Management of Trauma Patients in An Emergency Department of A Tertiary Hospital in TanzaniaDocument6 pagesPain Assessment and Management of Trauma Patients in An Emergency Department of A Tertiary Hospital in TanzaniamandsximenesNo ratings yet
- A Trial Examining An Advanced Practice Nurse Intervention To Promote Medication Adherence and Symptom Management in Adult Cancer Patients Prescribed Oral Anti-Cancer Agents - Study ProtocolDocument12 pagesA Trial Examining An Advanced Practice Nurse Intervention To Promote Medication Adherence and Symptom Management in Adult Cancer Patients Prescribed Oral Anti-Cancer Agents - Study ProtocolyawnerNo ratings yet
- Winn Effective Pain Management in The Long Term Care SettingDocument11 pagesWinn Effective Pain Management in The Long Term Care SettingJonathan MendhamNo ratings yet
- Listening Is Therapy Patient Interviewing From A Pain Science PerspectiveDocument13 pagesListening Is Therapy Patient Interviewing From A Pain Science PerspectiveDuvan CarvajalNo ratings yet
- Jurnal Paint 2 PDFDocument4 pagesJurnal Paint 2 PDFAlpendLadjarNo ratings yet
- Akpanudoh 1,2,3 Last WorkDocument51 pagesAkpanudoh 1,2,3 Last Workessiendaniel001No ratings yet
- Aplikasi Brief Pain Inventory Bpi Indonesian VersiDocument12 pagesAplikasi Brief Pain Inventory Bpi Indonesian Versixiongmao2389No ratings yet
- 17. Trevino et al, 2021 - NÃO - PACIENTES MISTOS EM TRATAMENTO E APÓS A FINALIZAÇÃODocument20 pages17. Trevino et al, 2021 - NÃO - PACIENTES MISTOS EM TRATAMENTO E APÓS A FINALIZAÇÃOAline Antunes Pereira RosaNo ratings yet
- Jurnal 3Document7 pagesJurnal 3adi suciptoNo ratings yet
- HHS Public Access: The ABCDEF Bundle in Critical CareDocument23 pagesHHS Public Access: The ABCDEF Bundle in Critical CareRodrigoSachiFreitasNo ratings yet
- Journal Nursing Management 2006: March 2014Document11 pagesJournal Nursing Management 2006: March 2014Joana R. SilvaNo ratings yet
- Scale Comfort Touch Scale 2015Document15 pagesScale Comfort Touch Scale 2015Johana CifuentesNo ratings yet
- Tickell2019 Article TheEffectivenessOfMindfulnessDocument12 pagesTickell2019 Article TheEffectivenessOfMindfulnessDinda Putri KarinaNo ratings yet
- Ujph5 17607655 PDFDocument8 pagesUjph5 17607655 PDFImam Arni YusufNo ratings yet
- Good 2 Accuracy - of - The - Defining - CharaDocument9 pagesGood 2 Accuracy - of - The - Defining - CharaAhmad Umar MukhtarNo ratings yet
- Barriers To Cancer Pain Management Among Nurses in Kenya - A  Focused EthnographyDocument7 pagesBarriers To Cancer Pain Management Among Nurses in Kenya - A  Focused EthnographyBIETRIS WARISYUNo ratings yet
- Saifan2018 PDFDocument8 pagesSaifan2018 PDFClaudya TamaNo ratings yet
- DolorDocument21 pagesDolorfelipeguitastudiosNo ratings yet
- Pain Assessment in The Critically Ill Adult - Recent Evidence and New Trends PDFDocument11 pagesPain Assessment in The Critically Ill Adult - Recent Evidence and New Trends PDFSayonara BarbosaNo ratings yet
- Clinician BurnoutDocument7 pagesClinician Burnoutfgump123No ratings yet
- Critical Reviews in Oncology / HematologyDocument18 pagesCritical Reviews in Oncology / HematologyLiterasi MedsosNo ratings yet
- Top 10 Things Palliative Care Clinicians Wished Everyone Knew About Palliative CareDocument7 pagesTop 10 Things Palliative Care Clinicians Wished Everyone Knew About Palliative CareMateja BrebenNo ratings yet
- Impact of Nursing Diagnoses On Patient and Organisational Outcomes: A Systematic Literature ReviewDocument43 pagesImpact of Nursing Diagnoses On Patient and Organisational Outcomes: A Systematic Literature ReviewLucas Teles IanniNo ratings yet
- Nop2 10 2877Document9 pagesNop2 10 2877Oncología CdsNo ratings yet
- s12630 019 01482 WDocument12 pagess12630 019 01482 WAlex CullenNo ratings yet
- Qualitative ResearchDocument9 pagesQualitative ResearchGideon M KimariNo ratings yet
- Jurnal Pubmed Tugas Sik 4Document6 pagesJurnal Pubmed Tugas Sik 4srimaryanitellNo ratings yet
- Jurnal 7Document6 pagesJurnal 7Max MaghribiNo ratings yet
- Hinman 2024 PEAKDocument12 pagesHinman 2024 PEAKmsilvaNo ratings yet
- s00432-023-04679-1Document6 pagess00432-023-04679-1Dinar Khoirun NisaNo ratings yet
- Mullaney 2015Document6 pagesMullaney 2015Angel Paz-JesusNo ratings yet
- Fpsyg 14 1145100Document12 pagesFpsyg 14 1145100Abigail MJNo ratings yet
- Minimizing Pain Wound CareDocument6 pagesMinimizing Pain Wound CareRizki Tri RamadaniNo ratings yet
- 2020 Terri Glioma PRODocument7 pages2020 Terri Glioma PRORimpa Basu Achari100% (1)
- 64Document5 pages64Muthya GhitaNo ratings yet
- NS11530 Author Proof 002Document10 pagesNS11530 Author Proof 002ugwuobachinaemeremNo ratings yet
- Running Head: Anxiety Nursing Diagnosis 1Document8 pagesRunning Head: Anxiety Nursing Diagnosis 1Lucy AnneNo ratings yet
- Occupational Therapy and Management of Multiple Chronic Conditions in The Context of Health Care ReformDocument6 pagesOccupational Therapy and Management of Multiple Chronic Conditions in The Context of Health Care ReformNataliaNo ratings yet
- A Quality Improvement Study On The Feasibility and Potenti - 2023 - Brain BehaviDocument6 pagesA Quality Improvement Study On The Feasibility and Potenti - 2023 - Brain BehaviKourosh PourramezanNo ratings yet
- BrueraDocument21 pagesBrueraThatiana GimenesNo ratings yet
- Art 00036Document6 pagesArt 00036yu55ronNo ratings yet
- Knowledge and BeliefsDocument8 pagesKnowledge and Beliefshayatzu1No ratings yet
- NursingDocument24 pagesNursingPrita LestariNo ratings yet
- Therapy Response Imaging in OncologyFrom EverandTherapy Response Imaging in OncologyMizuki NishinoNo ratings yet
- Contoh AncovaDocument6 pagesContoh AncovaNYONGKERNo ratings yet
- 01.cir.90.1.35 6Document8 pages01.cir.90.1.35 6NYONGKERNo ratings yet
- Vipidia Alogliptin-Epar-Product-Information - enDocument40 pagesVipidia Alogliptin-Epar-Product-Information - enNYONGKERNo ratings yet
- Jurnal PaliatifDocument12 pagesJurnal PaliatifNYONGKERNo ratings yet
- Analisis Kebutuhan Tenaga Berdasarkan Beban Kerja Sebagai Dasar Perencanaan SDM Di Instalasi Farmasi RS. X SemarangDocument7 pagesAnalisis Kebutuhan Tenaga Berdasarkan Beban Kerja Sebagai Dasar Perencanaan SDM Di Instalasi Farmasi RS. X SemarangNYONGKERNo ratings yet
- Ournal of Linical Ncology: Rapid CommunicationDocument15 pagesOurnal of Linical Ncology: Rapid CommunicationNYONGKERNo ratings yet
- Primary Care Action GroupDocument35 pagesPrimary Care Action GroupNYONGKERNo ratings yet
- A Survey of Oncology Advanced Practice Nurses in Ontario: Profile and Predictors of Job SatisfactionDocument19 pagesA Survey of Oncology Advanced Practice Nurses in Ontario: Profile and Predictors of Job SatisfactionNYONGKERNo ratings yet
- Issue Date: February 6, 2017: Accreditation Survey Activity Guide For Health Care OrganizationsDocument107 pagesIssue Date: February 6, 2017: Accreditation Survey Activity Guide For Health Care OrganizationsNYONGKERNo ratings yet
- Manual Lymphatic Drainage Therapy in Patients With Breast Cancer Related LymphoedemaDocument6 pagesManual Lymphatic Drainage Therapy in Patients With Breast Cancer Related LymphoedemaNYONGKERNo ratings yet
- Treatment of Breast-Cancer-related Lymphedema With or Without Manual Lymphatic DrainageDocument7 pagesTreatment of Breast-Cancer-related Lymphedema With or Without Manual Lymphatic DrainageNYONGKERNo ratings yet
- Job Satisfaction, Intent To Stay, and Recommended Job Improvements: The Palliative Nursing Assistant SpeaksDocument6 pagesJob Satisfaction, Intent To Stay, and Recommended Job Improvements: The Palliative Nursing Assistant SpeaksNYONGKERNo ratings yet
- Le Couturier 1999Document9 pagesLe Couturier 1999NYONGKERNo ratings yet
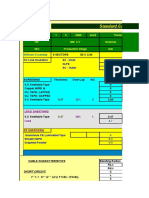
- 2500 - 380 KVDocument32 pages2500 - 380 KVelsayedNo ratings yet
- 56th NMTCDocument9 pages56th NMTCAtharv JainNo ratings yet
- 4 Business Projectors BrochureDocument8 pages4 Business Projectors BrochureKanaisan KarupiahNo ratings yet
- NCSS With GESS 7.1.20 All Versions Serial Number and Keygen For Ncss With Gess Free Download 633d0a67Document2 pagesNCSS With GESS 7.1.20 All Versions Serial Number and Keygen For Ncss With Gess Free Download 633d0a67Hector GonzalezNo ratings yet
- Class 6 UNIT 8-SUPPLY AND DEMAND - PRICE-TAKING AND COMPETITIVE MARKETSDocument5 pagesClass 6 UNIT 8-SUPPLY AND DEMAND - PRICE-TAKING AND COMPETITIVE MARKETSSara MartínNo ratings yet
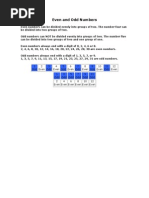
- Even and Odd NumbersDocument1 pageEven and Odd NumbersbarranquitasNo ratings yet
- Iteration Mark SchemeDocument14 pagesIteration Mark SchemeAyra MujibNo ratings yet
- Industrial Electronics Lab Manual UOCDocument81 pagesIndustrial Electronics Lab Manual UOCImran ShaukatNo ratings yet
- Abha Private Hospital - KSA: 1. Project DescriptionDocument6 pagesAbha Private Hospital - KSA: 1. Project DescriptionOsama AlsherifNo ratings yet
- Problems SolutionsDocument4 pagesProblems SolutionsMd Himel HossainNo ratings yet
- CFD Analysis of Shell and Coil Heat Exchanger by Using Different Mass Flow Rate For Hot and Cold FluidDocument19 pagesCFD Analysis of Shell and Coil Heat Exchanger by Using Different Mass Flow Rate For Hot and Cold FluidIJRASETPublicationsNo ratings yet
- GTS Academy Free Demo Test PDFDocument10 pagesGTS Academy Free Demo Test PDFHallo KhanNo ratings yet
- Lab 12Document11 pagesLab 12Travis Jon Wheelwright79% (14)
- Sip Report AllDocument80 pagesSip Report AllSmarak0604100% (1)
- Review On Design and Analysis of Front BumperDocument4 pagesReview On Design and Analysis of Front BumperEditor IJTSRDNo ratings yet
- Parenting StylesDocument14 pagesParenting StylesBruce WayneNo ratings yet
- The Effect of Projection Errors On Cephalometric Length MeasurementsDocument8 pagesThe Effect of Projection Errors On Cephalometric Length MeasurementsNeeraj AroraNo ratings yet
- Colpitts OscillatorDocument3 pagesColpitts Oscillatorasra 10100% (2)
- Electronics & Communication Engineering: Model CurriculumDocument62 pagesElectronics & Communication Engineering: Model CurriculumDj Nk VermaNo ratings yet
- SIFT - The Scale Invariant Feature TransformDocument62 pagesSIFT - The Scale Invariant Feature TransformtantanNo ratings yet
- 1.5b WKSHT Integers in ContextDocument2 pages1.5b WKSHT Integers in ContextGir0faNo ratings yet
- Dead Key: Space So A Plain Grave Accent Can Be Typed by PressingDocument4 pagesDead Key: Space So A Plain Grave Accent Can Be Typed by PressingMaxwell MoralesNo ratings yet
- Geospatial Analysis 6th Edition, : and TerminologyDocument1 pageGeospatial Analysis 6th Edition, : and TerminologyYaseen MuhammadNo ratings yet
- Air - Temperature, Pressure and DensityDocument1 pageAir - Temperature, Pressure and DensitysigmathetaNo ratings yet
- Silica, Calorimetric, Molybd'ate Blue: 1. ApplicationDocument2 pagesSilica, Calorimetric, Molybd'ate Blue: 1. ApplicationLượng Nguyễn VănNo ratings yet
- Tensor Short Sample SecureDocument15 pagesTensor Short Sample SecureDevendra AryaNo ratings yet
- Membrane Filtration TechniquesDocument53 pagesMembrane Filtration TechniquesSreejesh P C100% (1)
- MCom SyllabusDocument24 pagesMCom SyllabusSelvarajr RajaraNo ratings yet