GIT OSCE (Week 9) : Mention You Would Observe General Appearance and Take Vitals
GIT OSCE (Week 9) : Mention You Would Observe General Appearance and Take Vitals
Download as pdf or txt
You might also like
- NBME+Anatomy+Review+ 1 PDFDocument59 pagesNBME+Anatomy+Review+ 1 PDFAqsa Mumtaz100% (1)
- Cardiology - CVS OSCE ChecklistDocument5 pagesCardiology - CVS OSCE ChecklistPraveenaNo ratings yet
- CARAS SCUTSHEET 2nd EditDocument2 pagesCARAS SCUTSHEET 2nd EditFrances Katrina Siruno100% (2)
- Os 206: Pe of The Abdomen - ©spcabellera, Upcm Class 2021Document4 pagesOs 206: Pe of The Abdomen - ©spcabellera, Upcm Class 2021Ronneil BilbaoNo ratings yet
- Cardiology Mnemonics PDFDocument22 pagesCardiology Mnemonics PDFEliza SparkNo ratings yet
- Practical Guide To YogaDocument106 pagesPractical Guide To YogaKartik Vashishta100% (2)
- Abdominal Examination GuideDocument4 pagesAbdominal Examination GuidePhysician Associate100% (2)
- Abdominal ExaminationDocument16 pagesAbdominal ExaminationLana IbrahimNo ratings yet
- Abdo and HerniasDocument6 pagesAbdo and Herniasjoedeegan_No ratings yet
- Physical ExaminationDocument5 pagesPhysical ExaminationAmniAzmi100% (2)
- Cranial Nerve ExaminationDocument3 pagesCranial Nerve Examinationapi-195986134No ratings yet
- Abdominal Examination - OSCE Guide - Geeky MedicsDocument9 pagesAbdominal Examination - OSCE Guide - Geeky MedicsJahangir Alam100% (1)
- GIT Examination - Clinical Skills With DRDocument8 pagesGIT Examination - Clinical Skills With DRNaveen KovalNo ratings yet
- Thyroid Status Examination OSCE GuideDocument20 pagesThyroid Status Examination OSCE GuideemmaNo ratings yet
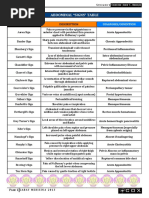
- Abdominal "Signs" Table: Sign Diagnosis/ConditionDocument1 pageAbdominal "Signs" Table: Sign Diagnosis/ConditionMeg AmoonNo ratings yet
- Almaghrabi Cardio ExaminationDocument22 pagesAlmaghrabi Cardio ExaminationSagit Nauman81No ratings yet
- Investigations Management Notes For FinalsDocument138 pagesInvestigations Management Notes For FinalsThistell ThistleNo ratings yet
- Cardiovascular History Taking and Physical ExaminationsDocument35 pagesCardiovascular History Taking and Physical ExaminationsEndalk AsfawNo ratings yet
- How To Take HistoryDocument59 pagesHow To Take HistoryBelalNo ratings yet
- Pathognomonic Is A Term, Often Used in Medicine That Means Characteristic For A Particular Disease - The WordDocument3 pagesPathognomonic Is A Term, Often Used in Medicine That Means Characteristic For A Particular Disease - The WordKristian Jane de JesusNo ratings yet
- HW InotropesDocument3 pagesHW InotropesNatalie YeohNo ratings yet
- CVS Heart MurmursDocument2 pagesCVS Heart MurmursIamTinesh100% (1)
- Cardiovascular ExaminationDocument5 pagesCardiovascular ExaminationMTBRISCOENo ratings yet
- Emergency Lecture PDFDocument57 pagesEmergency Lecture PDFDuane Liloc100% (2)
- Classification of MurmursDocument2 pagesClassification of MurmursNazneen SiddiquiNo ratings yet
- RS 12 Steps Respiratory Examination ChecklistDocument1 pageRS 12 Steps Respiratory Examination ChecklistEe Chen HengNo ratings yet
- Acute Abdominal Pain History and Exam HPCDocument5 pagesAcute Abdominal Pain History and Exam HPCnaafNo ratings yet
- Introduction History and ExaminationDocument43 pagesIntroduction History and ExaminationDanyal Hassan100% (1)
- Cardiovascular Examination GuideDocument2 pagesCardiovascular Examination Guiderhea100% (1)
- General Exam and Q&A For MBBS DR ShamolDocument320 pagesGeneral Exam and Q&A For MBBS DR Shamolmaybe100% (3)
- Thyroid Case ProformaDocument2 pagesThyroid Case ProformaSneha NaulakhaNo ratings yet
- Abdomenal Exam HandoutDocument5 pagesAbdomenal Exam HandoutNesma AdelNo ratings yet
- Examination of The AbdomenDocument2 pagesExamination of The Abdomenkenners100% (13)
- Almaghrabi Abdomen ExaminationDocument27 pagesAlmaghrabi Abdomen ExaminationSagit Nauman81100% (1)
- Examination Medicine: General Systems ChapterDocument17 pagesExamination Medicine: General Systems ChapterMahmoud AbouelsoudNo ratings yet
- Medical MnemonicsDocument15 pagesMedical MnemonicsPrashantVedwanNo ratings yet
- Neuro 1 and 2 LabDocument3 pagesNeuro 1 and 2 LabHardikPatelNo ratings yet
- Thyroid Examination FiryaLDocument3 pagesThyroid Examination FiryaLFiryal Balushi100% (1)
- How To Read An ECG: Confirm DetailsDocument15 pagesHow To Read An ECG: Confirm DetailsRinothja Rajaratnam100% (1)
- Physical Exam ChecklistDocument2 pagesPhysical Exam ChecklistRaisah Bint Abdullah100% (5)
- Right Hypochondrium2Document4 pagesRight Hypochondrium2Subash KarkiNo ratings yet
- Cardiovascular ExaminationDocument13 pagesCardiovascular ExaminationBitu JaaNo ratings yet
- Differentials For Finals: - Pleuritic Chest Pain - Pulmonary Embolism - Pneumothorax PneumoniaDocument9 pagesDifferentials For Finals: - Pleuritic Chest Pain - Pulmonary Embolism - Pneumothorax PneumoniaOlivia MoranNo ratings yet
- Rapid History Taking: 1. Patient ProfileDocument3 pagesRapid History Taking: 1. Patient ProfileTunio Usama100% (1)
- Right Iliac Fossa Mass: Case Presentation by K. Umashankar and G. PraveenDocument19 pagesRight Iliac Fossa Mass: Case Presentation by K. Umashankar and G. Praveen7hhdfc8vmwNo ratings yet
- MCQ 1. Heart Sound Heart Sound S1 S2Document7 pagesMCQ 1. Heart Sound Heart Sound S1 S2Atirah AaNo ratings yet
- Clinical Examination NOTESDocument11 pagesClinical Examination NOTESDanielDzinotyiweiD-cubedNo ratings yet
- ToxidromesDocument1 pageToxidromesMayer Rosenberg100% (7)
- Cardiac MurmursDocument3 pagesCardiac MurmursDanielleNo ratings yet
- Cranial Nerves ExaminationDocument11 pagesCranial Nerves ExaminationAlena JosephNo ratings yet
- 2 Approach To The Neuro Exam Feb 2011Document35 pages2 Approach To The Neuro Exam Feb 2011suaqaziNo ratings yet
- Clinical Examination Sheet (General Examination)Document3 pagesClinical Examination Sheet (General Examination)Yara WaelNo ratings yet
- Examination of The Peripheral Neurological SystemDocument2 pagesExamination of The Peripheral Neurological Systemkenners100% (12)
- Nervous System ProformaDocument10 pagesNervous System ProformaEBNo ratings yet
- Nervous System AlterationsDocument45 pagesNervous System AlterationsMajesty ParkerNo ratings yet
- Electrolyte Cheat SheetDocument1 pageElectrolyte Cheat SheetChristinaNo ratings yet
- Problem-based Approach to Gastroenterology and HepatologyFrom EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisNo ratings yet
- AssesssingDocument20 pagesAssesssingKRISTIAN DRAZEN MIRANDANo ratings yet
- AbdomenDocument9 pagesAbdomenMDNICNo ratings yet
- Abdomen and GI ExaminationDocument22 pagesAbdomen and GI ExaminationabdiwahabNo ratings yet
- Pa of Abdomen PrintDocument14 pagesPa of Abdomen PrintAnj LTNo ratings yet
- CHIR919 Rehabilitation Exam Session 2 2017Document13 pagesCHIR919 Rehabilitation Exam Session 2 2017renae_vardNo ratings yet
- Physical Examination by RegionDocument13 pagesPhysical Examination by Regionrenae_vard100% (1)
- Upper Extremity Week 9: Presented by Navine HaworthDocument27 pagesUpper Extremity Week 9: Presented by Navine Haworthrenae_vardNo ratings yet
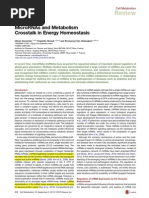
- MiRNA MetabolismDocument13 pagesMiRNA Metabolismrenae_vardNo ratings yet
- ATS1371 MoralityDocument28 pagesATS1371 Moralityrenae_vardNo ratings yet
- Phy2042 Renal 3Document6 pagesPhy2042 Renal 3renae_vardNo ratings yet
- Science 6 - Q2 - L3 - Parts and Function of Digestive SystemDocument23 pagesScience 6 - Q2 - L3 - Parts and Function of Digestive SystemSonny Matias100% (1)
- Gnaps: Lomerulo Efritis KUT Asca TreptokokusDocument32 pagesGnaps: Lomerulo Efritis KUT Asca TreptokokusRamsyifa VirzanisdaNo ratings yet
- Abdominal UltrasoundDocument6 pagesAbdominal Ultrasounds0800841739100% (1)
- Acute CholecystitisDocument18 pagesAcute CholecystitisOktavia PutriNo ratings yet
- ### O Level Notes - Human Digestive SystemDocument2 pages### O Level Notes - Human Digestive SystemboyaneshNo ratings yet
- COLPORRHEXISDocument12 pagesCOLPORRHEXISAsogaa Meteran50% (2)
- Kadek Miantari (C1118051) Tugas Keperawatan Medikal Bedah IIDocument34 pagesKadek Miantari (C1118051) Tugas Keperawatan Medikal Bedah IIAA Made Agus Dwi SuprasthaNo ratings yet
- Acute Liver FailureDocument3 pagesAcute Liver FailureElisabeth F. OjhaNo ratings yet
- Reviewer Digestive SystemDocument12 pagesReviewer Digestive SystemLorenzo Gabriel RSNo ratings yet
- The Cichlids Yearbook Vol 1Document22 pagesThe Cichlids Yearbook Vol 1elisav100% (1)
- Grading of Hydronephrosis: An Ongoing Challenge: Abdurrahman OnenDocument13 pagesGrading of Hydronephrosis: An Ongoing Challenge: Abdurrahman OnensavitageraNo ratings yet
- Anatomy of Digestive SystemDocument20 pagesAnatomy of Digestive Systemolive jollyNo ratings yet
- Physical AssessmentDocument1 pagePhysical AssessmentSoriao, Lovely Rose V.No ratings yet
- Meralgia Paresthetica: Case PresentationDocument2 pagesMeralgia Paresthetica: Case PresentationjalalfaizNo ratings yet
- Git AnatomyDocument62 pagesGit AnatomyBimo HarmajiNo ratings yet
- Cholelithiasis & CholecystitisDocument2 pagesCholelithiasis & CholecystitisKate DNo ratings yet
- Laparoscopic Cholecystectomy - StatPearls - NCBI BookshelfDocument1 pageLaparoscopic Cholecystectomy - StatPearls - NCBI BookshelfOmar HamwiNo ratings yet
- Mindmap Digestive AnatomyDocument2 pagesMindmap Digestive Anatomyapi-535582646No ratings yet
- Abdominal Examination - 2 - 1Document16 pagesAbdominal Examination - 2 - 1Zeinab AmerNo ratings yet
- Ch06 Digestive SystemDocument69 pagesCh06 Digestive Systemgeotina.kelseyNo ratings yet
- GIT Mcqs by DR Elsayed EmaraDocument13 pagesGIT Mcqs by DR Elsayed EmaraHasen umerNo ratings yet
- 9 Regions of AbdomenDocument4 pages9 Regions of AbdomenKryza Dale Bunado Batican50% (2)
- Identification of Shrimp and PrawnsDocument50 pagesIdentification of Shrimp and PrawnsRajan KumarNo ratings yet
- Klasifikasi Tindakan Bedah Digestif Update 20 Juni 2022 (BPJS)Document7 pagesKlasifikasi Tindakan Bedah Digestif Update 20 Juni 2022 (BPJS)Eko RistiyantoNo ratings yet
- Abdominal SurgeriesDocument16 pagesAbdominal SurgeriesKunal BhardwajNo ratings yet
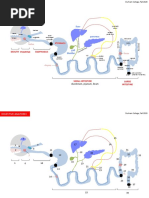
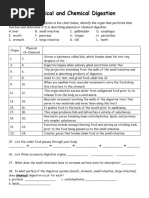
- Physical and Chemical Digestion With DiagramDocument2 pagesPhysical and Chemical Digestion With Diagramlaralapolice83No ratings yet
- Esophageal Reconstruction With Large Intestine: 1. Vascular Anatomy of The ColonDocument26 pagesEsophageal Reconstruction With Large Intestine: 1. Vascular Anatomy of The ColonCitra AryantiNo ratings yet