Post Insertion Problems and Their Management in Co PDF
Post Insertion Problems and Their Management in Co PDF
Download as pdf or txt
You might also like
- Completedenture Theory and PracticeDocument1,233 pagesCompletedenture Theory and PracticeMostafa Fayad100% (7)
- Soap Note - Musculoskeletal and Nervous SystemsDocument2 pagesSoap Note - Musculoskeletal and Nervous SystemsSummer Keller89% (9)
- 05 Clinical Failures and Its Management in Fixed Partial DentureDocument45 pages05 Clinical Failures and Its Management in Fixed Partial Denturesonal_karania66% (29)
- Space Maintainer - A ReviewDocument5 pagesSpace Maintainer - A ReviewHabeeb AL-Absi100% (1)
- Increasing Vertical DimensionDocument6 pagesIncreasing Vertical DimensionAriel Acevedo100% (1)
- Document (Denture Over Denture)Document39 pagesDocument (Denture Over Denture)Saifurahman TarakiNo ratings yet
- Relining & RebasingDocument86 pagesRelining & RebasingJASPREETKAUR0410100% (2)
- Prosthodontics Lec#3Document12 pagesProsthodontics Lec#3Forat hussienNo ratings yet
- Biologic Width & Emergence ProfileDocument33 pagesBiologic Width & Emergence ProfileNirav RathodNo ratings yet
- Preparation of Mouth For Removable Partial Dentures Dr. Mazen KanoutDocument9 pagesPreparation of Mouth For Removable Partial Dentures Dr. Mazen KanoutManjeev GuragainNo ratings yet
- Preparation of Mouth For Removable Partial DenturesDocument47 pagesPreparation of Mouth For Removable Partial DenturesSeena Sam100% (2)
- Insersi Instruksi Evaluasi GTL Presentasi DRG - HelmiDocument37 pagesInsersi Instruksi Evaluasi GTL Presentasi DRG - HelmigilangNo ratings yet
- Faliur Partial Denture FixxDocument45 pagesFaliur Partial Denture FixxsalmagintokiNo ratings yet
- Pros Lec11Document15 pagesPros Lec11منتظر الحمدانيNo ratings yet
- Patient Selection in Lingual OrthodonticsDocument8 pagesPatient Selection in Lingual OrthodonticsSreenivasa Krishna ChaitanyaNo ratings yet
- Ceramic Veneers in General Dental PracticeDocument11 pagesCeramic Veneers in General Dental PracticeheycoolalexNo ratings yet
- Extractions in OrthodonticsDocument6 pagesExtractions in OrthodonticsZubair AhmedNo ratings yet
- Full Mouth RehabDocument37 pagesFull Mouth RehabAravind Krishnan100% (6)
- A New Fixed Acrylic Bite Plane For Deep Bite CorrectionDocument6 pagesA New Fixed Acrylic Bite Plane For Deep Bite CorrectionFisaNo ratings yet
- Fixed Partial Dentures and Operative DentistryDocument6 pagesFixed Partial Dentures and Operative DentistryAlina AnechiteiNo ratings yet
- Lecture No8 Drnidhal 2017 Treatment PlaningDocument9 pagesLecture No8 Drnidhal 2017 Treatment PlaningQueen LiveNo ratings yet
- Seminar 6 Preventive Prosthodontics in CD WordDocument29 pagesSeminar 6 Preventive Prosthodontics in CD Wordketaki kunteNo ratings yet
- Orthodontic Retention and RelapseDocument6 pagesOrthodontic Retention and RelapseNada BrassnNo ratings yet
- Prostho Rehabilitation - HypodontiaDocument24 pagesProstho Rehabilitation - HypodontiaAmniAzmiNo ratings yet
- Lingual-Keys For SuccessDocument8 pagesLingual-Keys For SuccessGoutam NookalaNo ratings yet
- Post Insertion InstructionsDocument23 pagesPost Insertion InstructionsAnkita Reddy VallapNo ratings yet
- How To Effectively Use A 264 Appliance: Features SectionDocument11 pagesHow To Effectively Use A 264 Appliance: Features SectionJulio Ugás ZapataNo ratings yet
- Single Complete Denture FinalDocument15 pagesSingle Complete Denture FinalVikas Aggarwal100% (1)
- Periodontics With Other Aspect of Dentistry: DR Alaa OmranDocument7 pagesPeriodontics With Other Aspect of Dentistry: DR Alaa OmranYehya Al KhashabNo ratings yet
- Try-In RPDDocument8 pagesTry-In RPDSRO oONo ratings yet
- Orthodontics and Periodontal Therapy (Vandarshall)Document18 pagesOrthodontics and Periodontal Therapy (Vandarshall)Priya SJNo ratings yet
- Overdenture 4th Year 15-3-2020Document52 pagesOverdenture 4th Year 15-3-2020Ahmed AliNo ratings yet
- Failures of Fixed Partial DenturesDocument24 pagesFailures of Fixed Partial DenturesBalamurugan Devaraj100% (1)
- A To Z Orthodontics Vol 20 SurgicalDocument23 pagesA To Z Orthodontics Vol 20 Surgicalshruti premsagarNo ratings yet
- InfractionDocument44 pagesInfractionAisyahNasirNo ratings yet
- 2 Diagnosis - IntraoralDocument73 pages2 Diagnosis - IntraoralmanoNo ratings yet
- Complete Denture Fabrication For Old Denture Wearer in One DayDocument3 pagesComplete Denture Fabrication For Old Denture Wearer in One DayAsma Akram - ProsthodonticsNo ratings yet
- Mouth Preparation in RPDDocument14 pagesMouth Preparation in RPDDr. Mangala Jyothi KJNo ratings yet
- Tooth Supported Overdenture: Year 5 ProsthodonticsDocument10 pagesTooth Supported Overdenture: Year 5 ProsthodonticsLiz Jain J AlapattNo ratings yet
- The Correction of Occlusal Vertical Dimension On Tooth Wear: RostinyDocument4 pagesThe Correction of Occlusal Vertical Dimension On Tooth Wear: RostinyNabila AzzahraNo ratings yet
- International Journal of Current Advanced Research International Journal of Current Advanced ResearchDocument3 pagesInternational Journal of Current Advanced Research International Journal of Current Advanced ResearchgilangNo ratings yet
- Post Insertion ProblemsDocument22 pagesPost Insertion Problemsزياد حميد رشيدNo ratings yet
- CHAPTER 02 HistoryDocument13 pagesCHAPTER 02 Historyمحمد حسنNo ratings yet
- OverdentureDocument76 pagesOverdentureRaj Sha80% (5)
- Tooth-Supported Overdentures 2 PDFDocument7 pagesTooth-Supported Overdentures 2 PDFKrupali JainNo ratings yet
- Perio 2005 PresentationDocument115 pagesPerio 2005 Presentationraiesa hashemNo ratings yet
- Pedo Pulp Therapy Y4Document49 pagesPedo Pulp Therapy Y4Noor MaxeemNo ratings yet
- Curtis. The Influence of Removable Prosthodontic Procedures and Concepts On The Esthetics of Complete Dentures. (1987)Document9 pagesCurtis. The Influence of Removable Prosthodontic Procedures and Concepts On The Esthetics of Complete Dentures. (1987)Jose Enrique AvilaNo ratings yet
- How To Effectively Use A 264 Appliance: Features SectionDocument11 pagesHow To Effectively Use A 264 Appliance: Features Sectionvefiisphepy83312No ratings yet
- Falier in Fixed: 1-Tramatatic Periodontitis (Occlusal Imbalance)Document4 pagesFalier in Fixed: 1-Tramatatic Periodontitis (Occlusal Imbalance)s2s3No ratings yet
- Retantion and Relapse by DR Tamanna HabibDocument32 pagesRetantion and Relapse by DR Tamanna HabibTamanna HabibNo ratings yet
- Management Flabby RidgeDocument4 pagesManagement Flabby RidgeNidya Patricia Sembiring100% (1)
- Pre Prosthetic Surgery Lec. 9&10Document7 pagesPre Prosthetic Surgery Lec. 9&10Hassan BotaniNo ratings yet
- FMR of Worn Out DentititonDocument6 pagesFMR of Worn Out Dentititonrayavarapu sunilNo ratings yet
- Sturdevant's Bab 3 21-24Document4 pagesSturdevant's Bab 3 21-24andi ranggaNo ratings yet
- Orthodontics - 8th LectureDocument4 pagesOrthodontics - 8th LectureMarwan Qasim GhNo ratings yet
- Midline Diastema Treatment OptionsDocument6 pagesMidline Diastema Treatment OptionsnandaNo ratings yet
- Benefits of RPD: Elements and Compromised Function. The Removal of Exostoses and Tori Is Not A Complex ProcedureDocument8 pagesBenefits of RPD: Elements and Compromised Function. The Removal of Exostoses and Tori Is Not A Complex ProcedureSonia LeeNo ratings yet
- Treatment Planning Single Maxillary Anterior Implants for DentistsFrom EverandTreatment Planning Single Maxillary Anterior Implants for DentistsNo ratings yet
- Progressive Langerhans' Cell Histiocytosis in A Puppy (Pages 241-246)Document6 pagesProgressive Langerhans' Cell Histiocytosis in A Puppy (Pages 241-246)jenNo ratings yet
- WWW - Shaolinchikung.co - Uk: How Chi Kung WorksDocument11 pagesWWW - Shaolinchikung.co - Uk: How Chi Kung WorksarbkhanNo ratings yet
- AveNews (February 2021 Issue) PDFDocument4 pagesAveNews (February 2021 Issue) PDFCordellia ShereniNo ratings yet
- IHU - Company Profile (Update Oct 2022)Document10 pagesIHU - Company Profile (Update Oct 2022)Sherly ThendianNo ratings yet
- COVID 19 RT PCR Screening (Nucleic Acid Amplification Qualitative)Document2 pagesCOVID 19 RT PCR Screening (Nucleic Acid Amplification Qualitative)bawa sagguNo ratings yet
- Eliminación Ayunas Precontraste IVDocument61 pagesEliminación Ayunas Precontraste IVcpastorsNo ratings yet
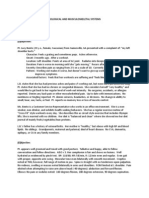
- Nimhans: National Institute of Mental Health and Neuro SciencesDocument32 pagesNimhans: National Institute of Mental Health and Neuro SciencesVikings GamingNo ratings yet
- The Musculoskeletal SystemDocument173 pagesThe Musculoskeletal SystemSupratik Chakraborty100% (1)
- Parwati Devi PDFDocument2 pagesParwati Devi PDFPRAGADEESHNo ratings yet
- Clarke Summative Clinical EvaluationDocument2 pagesClarke Summative Clinical Evaluationapi-610184566No ratings yet
- Bukidnon State UniversityDocument106 pagesBukidnon State UniversityfLOR_ZIANE_MAENo ratings yet
- PRUValue Med PRUMillion Med Booster Leaflet - ENGDocument14 pagesPRUValue Med PRUMillion Med Booster Leaflet - ENGchau thiranNo ratings yet
- Gordon's 11 Functional Health PatternDocument4 pagesGordon's 11 Functional Health PatternVhince Norben PiscoNo ratings yet
- Pharmacology 4th Edition George M. Brenner 2024 scribd downloadDocument81 pagesPharmacology 4th Edition George M. Brenner 2024 scribd downloadhordovselamaNo ratings yet
- Pediatric History FormatDocument3 pagesPediatric History Formatthebidaman1No ratings yet
- Diseases of The Spleen Burnett PDFDocument146 pagesDiseases of The Spleen Burnett PDFDrAbhay Meghaji ChhedaNo ratings yet
- Jackson Baumgartner ResumeDocument2 pagesJackson Baumgartner Resumeapi-399299717No ratings yet
- UK NHS Declines To Accelerate Grail Galleri Implementation Following Early Data Review - 360DxDocument2 pagesUK NHS Declines To Accelerate Grail Galleri Implementation Following Early Data Review - 360DxDivya PanchalNo ratings yet
- Dermaology CareDocument2 pagesDermaology CareSankita SandalNo ratings yet
- Pathophysiology of NephrolithiasisDocument3 pagesPathophysiology of NephrolithiasisArumDesiPratiwiNo ratings yet
- Panadol Sinus Relief Original Formula Tablets Product InformationDocument8 pagesPanadol Sinus Relief Original Formula Tablets Product Informationredof markzNo ratings yet
- Balint 1969Document8 pagesBalint 1969IsabelGuijarroMartinezNo ratings yet
- Hip Case Study 1Document3 pagesHip Case Study 1superhoofy7186No ratings yet
- ARTHRITIS-FINAL-PPT-2Document63 pagesARTHRITIS-FINAL-PPT-2DARIO BIDESNo ratings yet
- Ardio Ulmonary EsucitationDocument24 pagesArdio Ulmonary EsucitationfaizasaleemsameNo ratings yet
- Haydari Et Al 2017Document8 pagesHaydari Et Al 2017Valentina Llanca MejíasNo ratings yet
- ValsartanDocument3 pagesValsartanapi-3797941100% (1)
- Alcohol Dependence SyndromeDocument6 pagesAlcohol Dependence Syndromemaakkan100% (2)
- Red EyesDocument3 pagesRed EyesirijoaNo ratings yet