23 03 09 07 03 11 - Expansion
23 03 09 07 03 11 - Expansion
Download as pdf or txt
You might also like
- House Tree PersonDocument34 pagesHouse Tree PersonJackylou Blanco100% (2)
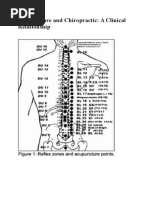
- Acupuncture and ChiropracticDocument5 pagesAcupuncture and Chiropracticمحمد زبيدي نور الدين100% (2)
- Горизонтальная дистракцияDocument7 pagesГоризонтальная дистракцияIrinaBorodulinaNo ratings yet
- Cleft PalateDocument4 pagesCleft PalateShoaib A. KaziNo ratings yet
- Aumento de Reborde Con Tejido BlandoDocument8 pagesAumento de Reborde Con Tejido BlandoSilvia SolisNo ratings yet
- 2005 Laster Width Distraction OsteogenesisDocument7 pages2005 Laster Width Distraction Osteogenesislisal1saNo ratings yet
- Enhancing Implantology With Autogenous Bone Block Ridge Augmentation Report of Two Cases - July - 2024 - 7952180220 - 4911983Document3 pagesEnhancing Implantology With Autogenous Bone Block Ridge Augmentation Report of Two Cases - July - 2024 - 7952180220 - 4911983Kaveri PawarNo ratings yet
- A New Approach To Maintenance of Regenerated Abm: Delayed Relining W: Xenograft and Resorbable Membrane. Stavola y TunkelDocument6 pagesA New Approach To Maintenance of Regenerated Abm: Delayed Relining W: Xenograft and Resorbable Membrane. Stavola y TunkelCristina Avramoff AguilarNo ratings yet
- Horizontal Ridge Augmentation Using Particulate BoneDocument12 pagesHorizontal Ridge Augmentation Using Particulate Bonecmfvaldesr7No ratings yet
- Pps 2Document5 pagesPps 2Hendy NurahadiNo ratings yet
- The Palatal Advanced Flap: A Pedicle Flap For Primary Coverage of Immediately Placed ImplantsDocument7 pagesThe Palatal Advanced Flap: A Pedicle Flap For Primary Coverage of Immediately Placed ImplantsMárcia ChatelieNo ratings yet
- Augmentation of The Sinus Floor With Mandibular Bone Block and Simultaneous Implantation: A 6-Year Clinical InvestigationDocument8 pagesAugmentation of The Sinus Floor With Mandibular Bone Block and Simultaneous Implantation: A 6-Year Clinical InvestigationWesley Silva100% (1)
- Screw Tent Pole Graft TechniqueDocument8 pagesScrew Tent Pole Graft TechniqueSweet ToothNo ratings yet
- Transcrestal Sinus Grafting With Immediate Implant Insertion Using Densa Burs in Severely Resorbed Alveolus A Special Case Report 6587a70d067e6Document5 pagesTranscrestal Sinus Grafting With Immediate Implant Insertion Using Densa Burs in Severely Resorbed Alveolus A Special Case Report 6587a70d067e6Mohamed TalaatNo ratings yet
- Implant Placement in Ridge SplitDocument10 pagesImplant Placement in Ridge SplitQuang Bui100% (1)
- 2015 - Pouch Roll Technique For Implant Soft-Tissue Augmentation of Small DefectsDocument5 pages2015 - Pouch Roll Technique For Implant Soft-Tissue Augmentation of Small DefectsVõHoàngThủyTiênNo ratings yet
- Bone Ring Autogenous GraftDocument4 pagesBone Ring Autogenous GraftHub SciNo ratings yet
- Jurnal ProstodonsiaDocument4 pagesJurnal ProstodonsiaWulan Ambar WatyNo ratings yet
- Bone Ring 1Document6 pagesBone Ring 1Pradusha RevuruNo ratings yet
- AJDSM Volume 22 Issue 3 Pages 247-251Document5 pagesAJDSM Volume 22 Issue 3 Pages 247-251MarisbebelaNo ratings yet
- Articulo ProtodonciaDocument5 pagesArticulo ProtodonciaMilton David Rios SerratoNo ratings yet
- New Microsoft Word DocumentDocument18 pagesNew Microsoft Word DocumentrnvisNo ratings yet
- Sequential Piezocision A Novel Approach To Acelerated Orthodontic TreatmentDocument11 pagesSequential Piezocision A Novel Approach To Acelerated Orthodontic TreatmentMargareth BritoNo ratings yet
- Expansión MaxilarDocument6 pagesExpansión MaxilarJennifer SalazarNo ratings yet
- Removal Of..Document4 pagesRemoval Of..Andrea ValverdeNo ratings yet
- 6 IntroductionDocument6 pages6 IntroductionDrsaumyaNo ratings yet
- Ann Maxillofac Surg Baikul 2014 205 7Document8 pagesAnn Maxillofac Surg Baikul 2014 205 7dimiz77No ratings yet
- Implants in Narrow Ridge Situations: A Piezo-Surgical Approach For Alveolar Ridge SplitDocument5 pagesImplants in Narrow Ridge Situations: A Piezo-Surgical Approach For Alveolar Ridge SplitNIMMY ANTONo ratings yet
- Implants in MandiblesDocument81 pagesImplants in MandiblesMoataz Mohamed Barakat100% (1)
- Background and ObjectivesDocument18 pagesBackground and ObjectivesrnvisNo ratings yet
- Trans Sinus Dental Implants For Immediate.11Document6 pagesTrans Sinus Dental Implants For Immediate.11Michal PerkowskiNo ratings yet
- Osteogenesis InglesDocument4 pagesOsteogenesis InglesJulio TorresNo ratings yet
- Khoury Bone Augmentation Tunneling-TechniqueDocument4 pagesKhoury Bone Augmentation Tunneling-TechniqueSeptimiu TiplicaNo ratings yet
- Maintenance of Gingival Form Following Implant PlacementDocument4 pagesMaintenance of Gingival Form Following Implant PlacementRomina BitaNo ratings yet
- 43 52 10Document10 pages43 52 10zeklawy73No ratings yet
- Crim - Dentistry2013 260707Document5 pagesCrim - Dentistry2013 260707gamhaelNo ratings yet
- Tent-Pole in Regeneration TechniqueDocument4 pagesTent-Pole in Regeneration TechniqueangelicapgarciacastilloNo ratings yet
- Three-Dimensional Vertical Alveolar Ridge Augmentation in The Posterior Maxilla: A 10-Year Clinical StudyDocument10 pagesThree-Dimensional Vertical Alveolar Ridge Augmentation in The Posterior Maxilla: A 10-Year Clinical StudyFabian Sanabria100% (1)
- Bone and Tissue LevelDocument3 pagesBone and Tissue LevelSaleh AlsadiNo ratings yet
- Direct Maxillary Sinus Lift For Single Tooth Implant A Clinical StudyDocument4 pagesDirect Maxillary Sinus Lift For Single Tooth Implant A Clinical StudyRadita Dwihaning PutriNo ratings yet
- Esthetic Localized Soft Tissue Ridge Augmentation in A Fixed Partial Denture A Case Report PDFDocument3 pagesEsthetic Localized Soft Tissue Ridge Augmentation in A Fixed Partial Denture A Case Report PDFAmar Bhochhibhoya0% (1)
- Resective Osseous Surgery: A Tool in Restoring Smile - A Case ReportDocument3 pagesResective Osseous Surgery: A Tool in Restoring Smile - A Case ReportdoctormallikaNo ratings yet
- 19 - 23 Gopu Chandran LPDocument5 pages19 - 23 Gopu Chandran LPBagis Emre GulNo ratings yet
- Bone Ring 3Document4 pagesBone Ring 3Pradusha RevuruNo ratings yet
- Restoration of The Severely Decayed Tooth Using Crown Lengthening With Simultaneous Tooth-PreparationDocument5 pagesRestoration of The Severely Decayed Tooth Using Crown Lengthening With Simultaneous Tooth-PreparationIntelligentiaNo ratings yet
- The Socket-Shield Technique To Support The Buccofacial Tissues at Immediate Implant Placement PDFDocument7 pagesThe Socket-Shield Technique To Support The Buccofacial Tissues at Immediate Implant Placement PDFAhmed Mohammed Saaduddin Sapri100% (2)
- Decision Making With Zygomatic and Pterygoid Dental Implants - 2022 - DentistrDocument5 pagesDecision Making With Zygomatic and Pterygoid Dental Implants - 2022 - DentistrHien TruongNo ratings yet
- Immediate One-Stage Postextraction Implant: A Human Clinical and Histologic Case ReportDocument6 pagesImmediate One-Stage Postextraction Implant: A Human Clinical and Histologic Case ReportBagis Emre GulNo ratings yet
- Alveolar Ridge Augmentation by Distraction OsteogenesisDocument8 pagesAlveolar Ridge Augmentation by Distraction OsteogenesisCarlos Santiago VivenzaNo ratings yet
- EDI Journal - A Graftless Solution For Adjacent Implants in The Aesthetic Zone - Dr. Tunkiwala Et AlDocument6 pagesEDI Journal - A Graftless Solution For Adjacent Implants in The Aesthetic Zone - Dr. Tunkiwala Et AlNaina TalwarNo ratings yet
- JCDR 8 ZD04Document3 pagesJCDR 8 ZD04rajaniNo ratings yet
- Prosthetic Rehabilitation of Maxillectomy Patient With Telescopic DenturesDocument6 pagesProsthetic Rehabilitation of Maxillectomy Patient With Telescopic DenturesVero AngelNo ratings yet
- JDS 25 86Document5 pagesJDS 25 86Mozar Andrade Mota NetoNo ratings yet
- 7.review of LiteratureDocument18 pages7.review of LiteratureDrsaumyaNo ratings yet
- Digital New MohmDocument6 pagesDigital New MohmDina AbdelmoezNo ratings yet
- An 2/2 Implant Overdenture: Case ReportDocument3 pagesAn 2/2 Implant Overdenture: Case ReportasclepiuspdfsNo ratings yet
- Immediate Dentoalveolar Restoration in CompromisedDocument14 pagesImmediate Dentoalveolar Restoration in Compromisedbarrera2001No ratings yet
- Osseodensificação Com o TarcioDocument7 pagesOsseodensificação Com o Tarcioalessandra camposNo ratings yet
- Her Ford 2004Document9 pagesHer Ford 2004Prateik RathodNo ratings yet
- Split Technique 2Document8 pagesSplit Technique 2Alejandro RuizNo ratings yet
- Alargamiento Quirurgico de La Corona ClinicaDocument5 pagesAlargamiento Quirurgico de La Corona ClinicajulianNo ratings yet
- MAXUS Ebrochure-2021 LRDocument28 pagesMAXUS Ebrochure-2021 LRRaed Abu HamadNo ratings yet
- 043930BaselineReportDocument339 pages043930BaselineReportRaed Abu HamadNo ratings yet
- Commercial Aquaponic SystemsDocument12 pagesCommercial Aquaponic SystemsRaed Abu HamadNo ratings yet
- Aquaponics Toolkit O Hara 11-06-2016Document44 pagesAquaponics Toolkit O Hara 11-06-2016Raed Abu HamadNo ratings yet
- Binder 1Document18 pagesBinder 1Raed Abu Hamad50% (4)
- Diabetic Ketoacidosis: From Wikipedia, The Free EncyclopediaDocument4 pagesDiabetic Ketoacidosis: From Wikipedia, The Free EncyclopediaTika Fajar WulandariNo ratings yet
- Asia3 Product List 2 PDFDocument17 pagesAsia3 Product List 2 PDFYoussef KaidNo ratings yet
- A Clinical Study On Aya Bringaraja Karpam in Veluppu NoiDocument6 pagesA Clinical Study On Aya Bringaraja Karpam in Veluppu NoiparibashaiNo ratings yet
- Pityriasis RoseaDocument23 pagesPityriasis RoseaYellyasta Siusiu Imran100% (3)
- ن مقرر علم النفس التأهيليDocument38 pagesن مقرر علم النفس التأهيليZEINABNo ratings yet
- Critical Evaluation of FreudDocument23 pagesCritical Evaluation of FreudSakshi Jain100% (1)
- Laboratory Unit 3 1Document6 pagesLaboratory Unit 3 1Mushy_ayaNo ratings yet
- Surgical Atlas Transureteroureterostomy: John M. BarryDocument7 pagesSurgical Atlas Transureteroureterostomy: John M. BarrycristiangelsNo ratings yet
- E&M SheetDocument4 pagesE&M SheettimvrghsNo ratings yet
- Control of Communicable Disease in Man PDFDocument715 pagesControl of Communicable Disease in Man PDFNarendra50% (2)
- UrolithiasisDocument19 pagesUrolithiasisPupu Ayu WandiraNo ratings yet
- Mendeley SkoliosisDocument4 pagesMendeley SkoliosisTheonly LazabelNo ratings yet
- Refrensi Kodet 2Document8 pagesRefrensi Kodet 2A Syahriana NannaNo ratings yet
- Dermasol SDocument3 pagesDermasol SRedwanIsmailNo ratings yet
- II-118 High Alert Medications: PurposeDocument9 pagesII-118 High Alert Medications: PurposeAhmad Al-RusasiNo ratings yet
- Crohn DiseaseDocument31 pagesCrohn DiseasePoppy IndriasariNo ratings yet
- WaterMatrix - BrochureDocument2 pagesWaterMatrix - BrochureJamesNo ratings yet
- YelpDocument6 pagesYelpfazilakhan740No ratings yet
- Nursing Care Plan Patient: Mrs. K Age: 68 Diagnosis: Community Acquired PneumoniaDocument6 pagesNursing Care Plan Patient: Mrs. K Age: 68 Diagnosis: Community Acquired PneumoniaKerks Von Gladiel NapaoNo ratings yet
- Off Label Drug - Bu SintaDocument18 pagesOff Label Drug - Bu SintaChandra NiansariNo ratings yet
- Warner LambertDocument23 pagesWarner Lambertanon_963198911No ratings yet
- Gyorgyi Szabo Classification and Management of WoundDocument50 pagesGyorgyi Szabo Classification and Management of WoundMatheis Laskar PelangiNo ratings yet
- Pathogenic Parenting Concern Scale Childress 2011Document3 pagesPathogenic Parenting Concern Scale Childress 2011Milos VuckovicNo ratings yet
- Nib Advantage Visitor Cover FactsheetDocument3 pagesNib Advantage Visitor Cover Factsheethayat khanNo ratings yet
- Influence of Spray Drying Technology On The Physical and Nutritional Properties of Guava PowderDocument14 pagesInfluence of Spray Drying Technology On The Physical and Nutritional Properties of Guava PowderDr-Paras PorwalNo ratings yet
- NEBULIZATIONDocument3 pagesNEBULIZATIONkeyden adoNo ratings yet
- Interpretation of CPET PosterDocument1 pageInterpretation of CPET PosterczukmiklosNo ratings yet
- Cdnpsoriasisguidelines PDFDocument109 pagesCdnpsoriasisguidelines PDFbeberosariNo ratings yet