0% found this document useful (0 votes)
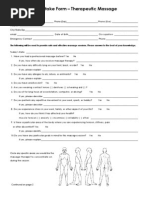
Massage Client Intake Form: Personal Information
Massage Client Intake Form: Personal Information
Download as pdf or txt
Download as pdf or txt
Download as pdf or txt
/ 1
Massage Client Intake Form: Personal Information