0% found this document useful (0 votes)
323 viewsRheumatic Endocarditis: o o o o o
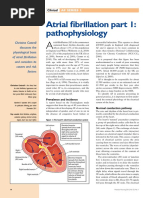
Rheumatic endocarditis is an inflammatory disease caused by streptococcal infection that damages heart valves, resulting in leakage or narrowing. It commonly affects school-aged children following strep throat. Prompt antibiotic treatment of strep throat can prevent rheumatic fever and associated heart damage. Patients may experience joint pain, involuntary movements, or heart murmurs. Treatment involves antibiotics, medications for pain and fever, and long-term antibiotic prophylaxis to prevent recurrence. Nurses educate patients on disease management, medication adherence, and symptom reporting.
Uploaded by
garatoh099Copyright
© Attribution Non-Commercial (BY-NC)
Available Formats
Download as DOCX, PDF, TXT or read online on Scribd
0% found this document useful (0 votes)
323 viewsRheumatic Endocarditis: o o o o o
Rheumatic endocarditis is an inflammatory disease caused by streptococcal infection that damages heart valves, resulting in leakage or narrowing. It commonly affects school-aged children following strep throat. Prompt antibiotic treatment of strep throat can prevent rheumatic fever and associated heart damage. Patients may experience joint pain, involuntary movements, or heart murmurs. Treatment involves antibiotics, medications for pain and fever, and long-term antibiotic prophylaxis to prevent recurrence. Nurses educate patients on disease management, medication adherence, and symptom reporting.
Uploaded by
garatoh099Copyright
© Attribution Non-Commercial (BY-NC)
Available Formats
Download as DOCX, PDF, TXT or read online on Scribd
/ 5