PDF 16900547 1584487082104 PDF
PDF 16900547 1584487082104 PDF
Download as pdf or txt
At a glance
Powered by AI
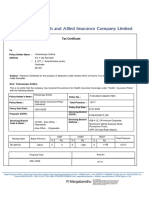
The key takeaways are that the document outlines an insurance policy purchase for Avinash Kumar with Religare Health Insurance. It provides details of the policy holder, insured individuals, sum insured, policy period and premium paid.
The policy being purchased is a floater policy under the CARE plan with a sum insured of Rs. 500,000 for a period between 17-Feb-2020 to 16-Feb-2021. The premium paid is Rs. 13,043 for a single premium payment.
The terms and conditions agreed to include consenting to medical examinations, sharing of medical information, receiving communications via electronic means, and responsibility for providing accurate information. The policy could be void in case of misrepresentation of details.
You might also like
- Premium ReceiptDocument1 pagePremium ReceiptPraba KaranNo ratings yet
- 80D CertificateDocument2 pages80D CertificateYogy YNo ratings yet
- Premium ReceiptDocument1 pagePremium ReceiptAbhishek TerdalkarNo ratings yet
- PremiumRept FamilyDocument2 pagesPremiumRept Familynavengg521No ratings yet
- PremiumRept MDS - RameshDocument2 pagesPremiumRept MDS - Rameshnavengg521No ratings yet
- NPS Contribution T-I INR 50KDocument3 pagesNPS Contribution T-I INR 50Ksumanpal78No ratings yet
- Care Health Policy 2023Document8 pagesCare Health Policy 2023Veda SiriNo ratings yet
- Health Insurance PolicyDocument3 pagesHealth Insurance PolicyNewsletter Online Technical supportNo ratings yet
- Cert 1335182145Document1 pageCert 1335182145Harbor View PlazaNo ratings yet
- HDFC ERGO General Insurance Company LimitedDocument4 pagesHDFC ERGO General Insurance Company LimitedHIMANSHU MEHTANo ratings yet
- Star Health PolicyDocument5 pagesStar Health PolicyTripathy RadhakrishnaNo ratings yet
- HDFC ERGO General Insurance Company LimitedDocument5 pagesHDFC ERGO General Insurance Company LimitedChiranjib PatraNo ratings yet
- MediclaimDocument3 pagesMediclaimPrajwal ShettyNo ratings yet
- Premium Receipt - 008927742 - 131423Document2 pagesPremium Receipt - 008927742 - 131423Vignesh MahadevanNo ratings yet
- LTA Bill Template 1 PDFDocument1 pageLTA Bill Template 1 PDF9816494828No ratings yet
- LIC Premium Receipt StatementDocument2 pagesLIC Premium Receipt StatementRMNo ratings yet
- 090003e88105430f SONIADocument3 pages090003e88105430f SONIAKoushik DuttaNo ratings yet
- 13 18 0038121 00 PDFDocument7 pages13 18 0038121 00 PDFRaoul JhaNo ratings yet
- Premium Receipt PDFDocument1 pagePremium Receipt PDFChidambaram VNo ratings yet
- 2825100207112402000Document4 pages2825100207112402000bipin012No ratings yet
- Received With Thanks ' 9,971.00 Through Payment Gateway Over The Internet FromDocument1 pageReceived With Thanks ' 9,971.00 Through Payment Gateway Over The Internet FromamitNo ratings yet
- Religare PDFDocument5 pagesReligare PDFsomnathNo ratings yet
- Kumar NagmaniDocument7 pagesKumar NagmaniKumar NagmoniNo ratings yet
- CareHealth Policy 2020-21 Nihit FamilyDocument5 pagesCareHealth Policy 2020-21 Nihit FamilyJacob Pruitt100% (1)
- FHP H0225594Document2 pagesFHP H0225594Raghavendra KamathNo ratings yet
- Medical InsuranceDocument1 pageMedical InsuranceMasood Ahmad100% (1)
- HDFC ERGO General Insurance Company Limited: Policy No. 2952 2007 9281 0602 001Document3 pagesHDFC ERGO General Insurance Company Limited: Policy No. 2952 2007 9281 0602 001Deena DayalanNo ratings yet
- Relig AreDocument5 pagesRelig AresomnathNo ratings yet
- Backup of Gopal InsurenceDocument5 pagesBackup of Gopal Insurencemkm969No ratings yet
- Renewal of Your Optima Restore Floater Insurance PolicyDocument4 pagesRenewal of Your Optima Restore Floater Insurance PolicyNikky KapoorNo ratings yet
- Parents Insurance TaxDocument1 pageParents Insurance Taxdev77729100% (1)
- ICICI COI IncomeProtect 445605Document5 pagesICICI COI IncomeProtect 445605sree koundinyaNo ratings yet
- Medical Insurance Certificate Max BupaDocument1 pageMedical Insurance Certificate Max BupaBinod DashNo ratings yet
- MedicalInsurancePremiumSrCitizen PDFDocument1 pageMedicalInsurancePremiumSrCitizen PDFRajul MathurNo ratings yet
- Health Insurance Policy Certificate Section80DDocument1 pageHealth Insurance Policy Certificate Section80DDebosmita DasNo ratings yet
- Renewal of Your Ican Essential Advanced Insurance PolicyDocument3 pagesRenewal of Your Ican Essential Advanced Insurance PolicySuganthi ChandrasekaranNo ratings yet
- FDGSDFGSDFGSDF: ICICI Lombard General Insurance Company Limited, IRDA Regn - No.115Document4 pagesFDGSDFGSDFGSDF: ICICI Lombard General Insurance Company Limited, IRDA Regn - No.115arjunNo ratings yet
- Medical Premium Receipt SelfDocument1 pageMedical Premium Receipt SelfRakesh AggarwalNo ratings yet
- Intermediary Code CO0000000062 Akshaya Wealth Management PVT - LTD Phone No 080-26535701/02/8026535701 E-Mail Id Services@AkshayaweaDocument4 pagesIntermediary Code CO0000000062 Akshaya Wealth Management PVT - LTD Phone No 080-26535701/02/8026535701 E-Mail Id Services@Akshayaweapushpkant kumarNo ratings yet
- RenewalReceipt 502-7066983 PolicyRenewalDocument2 pagesRenewalReceipt 502-7066983 PolicyRenewalSoumitra GuptaNo ratings yet
- PolicyDocument4 pagesPolicyJiso ThomasNo ratings yet
- Individual Premium Paid STMTDocument1 pageIndividual Premium Paid STMTGanesh SlvNo ratings yet
- Group Activ Travel - Certificate of Insurance: Insured Person DetailsDocument2 pagesGroup Activ Travel - Certificate of Insurance: Insured Person Detailsabhinay anandNo ratings yet
- Subject: Risk Assumption Letter: LAN Number: 19020618531140 Policy Number: 4111/EPP/164559158/00/000Document2 pagesSubject: Risk Assumption Letter: LAN Number: 19020618531140 Policy Number: 4111/EPP/164559158/00/000shekarNo ratings yet
- Star Health Cover NoteDocument3 pagesStar Health Cover NoteLakshya MittalNo ratings yet
- 80D SelfDocument1 page80D Selfnikhil nadakuditiNo ratings yet
- Prashant (1) CompletedDocument1 pagePrashant (1) CompletedAsifshaikh7566No ratings yet
- Royalsundaram - IT CERTIFICATE ParentsDocument1 pageRoyalsundaram - IT CERTIFICATE ParentsRaju GbNo ratings yet
- S.Kannan: 131118 SD CODE SD131118 Intermediary Code NameDocument3 pagesS.Kannan: 131118 SD CODE SD131118 Intermediary Code NamesuhailafrozNo ratings yet
- Certificate of Insurance HDFC ERGO Group ProtectDocument5 pagesCertificate of Insurance HDFC ERGO Group Protectzahid aliNo ratings yet
- Tax Certificate: R MargabandhuDocument2 pagesTax Certificate: R MargabandhuTrollstyleNo ratings yet
- Statement of Public Provident Fund Account: Ms - Neha Raghubar YadavDocument2 pagesStatement of Public Provident Fund Account: Ms - Neha Raghubar YadavNeha100% (1)
- Discovery Fund Premium ReceiptsDocument1 pageDiscovery Fund Premium ReceiptsKartikNo ratings yet
- Dear Saurabh SinghDocument1 pageDear Saurabh SinghSaurabh SinghNo ratings yet
- LIC Premium Jan 2023Document4 pagesLIC Premium Jan 2023Akriti SinghNo ratings yet
- Abhay KumarDocument5 pagesAbhay KumarSunil SahNo ratings yet
- Icici Lombard Mh!49966Document3 pagesIcici Lombard Mh!49966suresh sivadasanNo ratings yet
- 111528070Document6 pages111528070Sanjay KapoorNo ratings yet
- 10007104150chan PDFDocument4 pages10007104150chan PDFChandrasekhara kNo ratings yet
- PDF 17145960 1585132385521 PDFDocument7 pagesPDF 17145960 1585132385521 PDFLucky TraderNo ratings yet
- My Insurance PolicyDocument7 pagesMy Insurance PolicyMuntaj BegumNo ratings yet
- Black Pepper PDFDocument7 pagesBlack Pepper PDFLucky TraderNo ratings yet
- Lecture 24 Organic Certification PDFDocument28 pagesLecture 24 Organic Certification PDFLucky TraderNo ratings yet
- King Chilli PDFDocument6 pagesKing Chilli PDFLucky TraderNo ratings yet
- Biofertilizer and Organic Farming in FCO PDFDocument94 pagesBiofertilizer and Organic Farming in FCO PDFLucky TraderNo ratings yet
- Potato PDFDocument13 pagesPotato PDFLucky TraderNo ratings yet
- CHH14-Kanker Draft Plan-10.07.14 PDFDocument12 pagesCHH14-Kanker Draft Plan-10.07.14 PDFLucky TraderNo ratings yet
- BUCKWHEAT (Fagopyrum SPP.) Buckwheat A Nutri-CerealDocument8 pagesBUCKWHEAT (Fagopyrum SPP.) Buckwheat A Nutri-CerealLucky TraderNo ratings yet
- Spice Crops Ginger: Photo - Ginger Crop (Left) and Ginger Rhizome (Right) Soil and ClimateDocument12 pagesSpice Crops Ginger: Photo - Ginger Crop (Left) and Ginger Rhizome (Right) Soil and ClimateLucky TraderNo ratings yet
- Groundnut PDFDocument9 pagesGroundnut PDFLucky TraderNo ratings yet
- BUCKWHEAT (Fagopyrum SPP.) Buckwheat A Nutri-CerealDocument8 pagesBUCKWHEAT (Fagopyrum SPP.) Buckwheat A Nutri-CerealLucky TraderNo ratings yet
- Maize PDFDocument10 pagesMaize PDFLucky TraderNo ratings yet
- Organic Agriculture PDFDocument14 pagesOrganic Agriculture PDFLucky TraderNo ratings yet
- Pineapple PDFDocument9 pagesPineapple PDFLucky TraderNo ratings yet
- 9 IJEP November 2017 Barik PDFDocument8 pages9 IJEP November 2017 Barik PDFLucky TraderNo ratings yet
- Rice PDFDocument20 pagesRice PDFLucky TraderNo ratings yet
- Environmental Control Inside Poly House PDFDocument2 pagesEnvironmental Control Inside Poly House PDFLucky TraderNo ratings yet
- Carrot: Soil and ClimateDocument2 pagesCarrot: Soil and ClimateLucky TraderNo ratings yet
- Soybean PDFDocument5 pagesSoybean PDFLucky TraderNo ratings yet
- Guidance Compost and Vermicompost in Organic Crop ProductionDocument4 pagesGuidance Compost and Vermicompost in Organic Crop ProductionLucky TraderNo ratings yet
- Vegetable Cultivation With Pandals-APDocument7 pagesVegetable Cultivation With Pandals-APLucky TraderNo ratings yet
- Organic Horticulture in India: HorticulturaeDocument6 pagesOrganic Horticulture in India: HorticulturaeLucky TraderNo ratings yet
- Concept On Organic Vegetable Production: Odisha Review August - 2013Document10 pagesConcept On Organic Vegetable Production: Odisha Review August - 2013Lucky TraderNo ratings yet
- Saveer Root Trainer CatalougeDocument16 pagesSaveer Root Trainer CatalougeLucky TraderNo ratings yet
- Types, Components and Features of Polyhouse PDFDocument4 pagesTypes, Components and Features of Polyhouse PDFLucky TraderNo ratings yet
- Irjet V7i4185 PDFDocument4 pagesIrjet V7i4185 PDFLucky TraderNo ratings yet
- Saveer Lab Furniture Catalogue PDFDocument20 pagesSaveer Lab Furniture Catalogue PDFLucky TraderNo ratings yet
- Palram SolarSmart Technology Brochure (En) PDFDocument2 pagesPalram SolarSmart Technology Brochure (En) PDFLucky TraderNo ratings yet
- Noveltech - Annual Return - 2022Document15 pagesNoveltech - Annual Return - 2022Thanda UpenderNo ratings yet
- LIC's Jeevan Labh (Plan No. 936) : Benefit IllustrationDocument3 pagesLIC's Jeevan Labh (Plan No. 936) : Benefit IllustrationAtish SinghNo ratings yet
- The Six Principles in InsuranceDocument10 pagesThe Six Principles in InsuranceSonu KumarNo ratings yet
- BIKE INSURANCE - PDF - Deductible - InsuranceDocument6 pagesBIKE INSURANCE - PDF - Deductible - InsuranceDhatri ReddyNo ratings yet
- IFM12e Ch19Document12 pagesIFM12e Ch19jjxxhh888No ratings yet
- Life Contingencies II & III Formulas Analysis of Benefit ReservesDocument14 pagesLife Contingencies II & III Formulas Analysis of Benefit Reservesdavid AbotsitseNo ratings yet
- Currency Risk ManagementDocument52 pagesCurrency Risk ManagementWatan YarNo ratings yet
- Derivative Market Dealer Module Practice Book SampleDocument35 pagesDerivative Market Dealer Module Practice Book SampleMeenakshi0% (1)
- __SAMRAKSHANE-KARNATAKA __ Crop Insurance Application - NIC-BangaloreDocument1 page__SAMRAKSHANE-KARNATAKA __ Crop Insurance Application - NIC-BangaloreA RNo ratings yet
- IRDAN115RP0007V01201819: IRDA Registration No: 150 Bundled-Two Wheeler Policy (1 Yr Od + 5 Yrs TP) Cum ReceiptDocument1 pageIRDAN115RP0007V01201819: IRDA Registration No: 150 Bundled-Two Wheeler Policy (1 Yr Od + 5 Yrs TP) Cum ReceiptVeera KarthickNo ratings yet
- Types of Funding SourcesDocument20 pagesTypes of Funding SourcessmjohnsonNo ratings yet
- SuzlonDocument7 pagesSuzlonprajwalsacharya1996No ratings yet
- Surrender or Chargee Form PDFDocument1 pageSurrender or Chargee Form PDFSherlyn PhoonNo ratings yet
- Valuation Measuring and Managing The Value of Companies by Tim Koller, Marc Goedhart, David Wessels-Página888Document1 pageValuation Measuring and Managing The Value of Companies by Tim Koller, Marc Goedhart, David Wessels-Página888franzmartiniiNo ratings yet
- Health Insurance Policy Certificate Section80DDocument1 pageHealth Insurance Policy Certificate Section80DDebosmita DasNo ratings yet
- Chapter 2Document29 pagesChapter 2Moh'ed Crc QaajeNo ratings yet
- Black BookDocument35 pagesBlack Bookmansi berdeNo ratings yet
- ACE AMERICAN INSURANCE COMPANY v. LACARUBBA Et Al Yachtsman PolicyDocument24 pagesACE AMERICAN INSURANCE COMPANY v. LACARUBBA Et Al Yachtsman PolicyACELitigationWatchNo ratings yet
- List of Insurance Companies in IndiaDocument11 pagesList of Insurance Companies in IndiaSushil GuptaNo ratings yet
- General AnnuityDocument22 pagesGeneral AnnuityJomel RositaNo ratings yet
- Banking Awareness Quiz - Letter of CreditDocument5 pagesBanking Awareness Quiz - Letter of CreditPRIYA RANANo ratings yet
- Life Contingencies Study Note For CAS Exam SDocument14 pagesLife Contingencies Study Note For CAS Exam SJaswanth ChinnuNo ratings yet
- Nism 9Document19 pagesNism 9newbie1947No ratings yet
- Project On DerivatiesDocument84 pagesProject On DerivatiesNeeraj HotwaniNo ratings yet
- Startup Valuation ApproachesDocument15 pagesStartup Valuation Approachesguptaparag305No ratings yet
- Part 2 Risk and Return Raising Capital Corporate Restructuring and Bankruptcy - Sol 20 Jan 2024Document63 pagesPart 2 Risk and Return Raising Capital Corporate Restructuring and Bankruptcy - Sol 20 Jan 2024Tess PetancioNo ratings yet
- PrmPayRcpt 65962196Document1 pagePrmPayRcpt 65962196Divya KumaresanNo ratings yet
- Welcome To The World of Aditya Birla Capital!Document3 pagesWelcome To The World of Aditya Birla Capital!INSURANCE POINTNo ratings yet
- Moraboju: Single Candle PatternsDocument5 pagesMoraboju: Single Candle PatternsPhani TeeswaraNo ratings yet