Human Eye: General Properties
Human Eye: General Properties
Download as pdf or txt
At a glance
Powered by AI
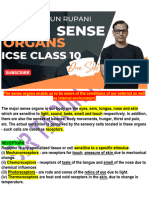
The key takeaways are that the human eye is made up of multiple parts that work together to allow vision. It has a cornea, iris, pupil, lens, retina and other components that help with light perception, depth perception, and color differentiation.
The main components of the human eye are the cornea, iris, pupil, lens, vitreous body, retina, aqueous humour and choroid.
The three coats that make up the eye are the outer fibrous tunic, middle vascular tunic and inner retina.
You might also like
- Azure - and Azure Government SOC 2 Type II ReportDocument225 pagesAzure - and Azure Government SOC 2 Type II ReportVijay RajendiranNo ratings yet
- Walter - Russel - Home Study Course (En)Document64 pagesWalter - Russel - Home Study Course (En)stban murillo100% (1)
- Azure-Planning and Finding Solutions For Migration - MOPDocument7 pagesAzure-Planning and Finding Solutions For Migration - MOPVijay RajendiranNo ratings yet
- Glaucoma 180813151731Document24 pagesGlaucoma 180813151731malathiNo ratings yet
- Potential Acuity Meter 16Document8 pagesPotential Acuity Meter 16Lavanya Madabushi100% (2)
- Human EyeDocument6 pagesHuman EyeclubsanatateNo ratings yet
- A Project On " Human Eye": Submitted To-Submitted byDocument13 pagesA Project On " Human Eye": Submitted To-Submitted byaman199075% (4)
- Sense Organ Eye Vision Rod Cone Retina: Citation NeededDocument11 pagesSense Organ Eye Vision Rod Cone Retina: Citation NeededPriyanshu MadanNo ratings yet
- Assessment of The EyeDocument4 pagesAssessment of The EyeAira Nicole ROMASNo ratings yet
- Dr. Olasupo S. AdeniyiDocument89 pagesDr. Olasupo S. AdeniyiUloko ChristopherNo ratings yet
- Human EyeDocument12 pagesHuman Eyeanu rettiNo ratings yet
- Introduction To Eye Disorders-1Document11 pagesIntroduction To Eye Disorders-1bhavani G100% (1)
- Human EyeDocument4 pagesHuman EyeLit Central DreamsNo ratings yet
- Section 13 - Chapter 6 Anatomy and Structure of The EyeDocument12 pagesSection 13 - Chapter 6 Anatomy and Structure of The EyeMosteanu IulianNo ratings yet
- Topic Presentation CataractDocument11 pagesTopic Presentation Cataractjyoti singh100% (1)
- Introduction To Ophthalmology: by DR - Bakhtiar Q. JafDocument41 pagesIntroduction To Ophthalmology: by DR - Bakhtiar Q. JafChristian JaraNo ratings yet
- Occupational Health Tips On Eye Protection For Good Visual HealthFrom EverandOccupational Health Tips On Eye Protection For Good Visual HealthNo ratings yet
- Group 3: 1. Yuni Wulandari 2. Choirun Nisa Putri A. 3. Faitul Romela 4. Nurroddin FaridohDocument23 pagesGroup 3: 1. Yuni Wulandari 2. Choirun Nisa Putri A. 3. Faitul Romela 4. Nurroddin FaridohberbiallNo ratings yet
- Visual SystemDocument6 pagesVisual SystemJobelle Acena100% (1)
- Notes On EyesDocument6 pagesNotes On EyesSashoy AustinNo ratings yet
- Biology Investigatory Project: Samiksha Subhashish SarkarDocument35 pagesBiology Investigatory Project: Samiksha Subhashish SarkarSamiksha SarkarNo ratings yet
- Everyday Science NotesDocument46 pagesEveryday Science NotesGul JeeNo ratings yet
- Ocular Trauma: State of Illinois Trauma Nurse Specialist ProgramDocument38 pagesOcular Trauma: State of Illinois Trauma Nurse Specialist ProgramMayuha SaidNo ratings yet
- Jarvis: Physical Examination & Health Assessment, 3rd Canadian EditionDocument3 pagesJarvis: Physical Examination & Health Assessment, 3rd Canadian EditionkekeNo ratings yet
- Parts of The Human Eye With DefinitionDocument4 pagesParts of The Human Eye With DefinitionStarsky Allence Puyoc0% (1)
- WPR 2Document5 pagesWPR 2ishika mohanNo ratings yet
- ROLE OF EYE - A CRUCIAL PATH IN HUMAN LIFE Divya Jonnala, D. Navya, D. Eswar TonyDocument4 pagesROLE OF EYE - A CRUCIAL PATH IN HUMAN LIFE Divya Jonnala, D. Navya, D. Eswar TonyiajpsNo ratings yet
- Cross Section Drawing of The Eye - (Side View) With Major Parts LabeledDocument7 pagesCross Section Drawing of The Eye - (Side View) With Major Parts LabeledCamille ReneeNo ratings yet
- CSS Everyday Science Notes PDFDocument50 pagesCSS Everyday Science Notes PDFWaqas Gul100% (1)
- Anatomy and Physiology of The EyeDocument22 pagesAnatomy and Physiology of The EyeBalkos 61No ratings yet
- Sense OrgansDocument12 pagesSense Organsriwisi2139No ratings yet
- Anterior Chamber Aqueous HumorDocument6 pagesAnterior Chamber Aqueous HumorY D Amon GanzonNo ratings yet
- Errors of RefractionDocument27 pagesErrors of RefractionAminaNo ratings yet
- Low Vision: Assessment and Educational Needs: A Guide to Teachers and ParentsFrom EverandLow Vision: Assessment and Educational Needs: A Guide to Teachers and ParentsNo ratings yet
- Special Sense EYEDocument74 pagesSpecial Sense EYEprekshya shresthaNo ratings yet
- The Physics of Light and Color - Human Vision and Color Perception - Olympus LSDocument14 pagesThe Physics of Light and Color - Human Vision and Color Perception - Olympus LSmarialopezmartinez424No ratings yet
- 23 Facts About Your EyesDocument6 pages23 Facts About Your EyesRatnaPrasadNalamNo ratings yet
- Eye DisorderDocument14 pagesEye DisorderhuehueNo ratings yet
- Eye Diseases: An Investigatory Project by Shrikanth Pillai XII BDocument11 pagesEye Diseases: An Investigatory Project by Shrikanth Pillai XII BCR7STUDIO 7100% (1)
- Study Guide 11 Eye and Visual Disorders (For Studens)Document14 pagesStudy Guide 11 Eye and Visual Disorders (For Studens)Patricia EspirituNo ratings yet
- Macula Degeneration RlatedDocument12 pagesMacula Degeneration RlatedMuktha BpNo ratings yet
- Sense OrgansDocument11 pagesSense OrgansSusan FNo ratings yet
- Chapter 2Document12 pagesChapter 2basraawi379No ratings yet
- BIO-Project InvestigatoryDocument83 pagesBIO-Project InvestigatoryAyush BhattNo ratings yet
- Physics of Eyes and Vision Dentistry College Medical Physics Physics of Eyes and VisionDocument11 pagesPhysics of Eyes and Vision Dentistry College Medical Physics Physics of Eyes and VisionNIKHILA RAKESHNo ratings yet
- Pig EyeDocument6 pagesPig Eyeaims_sluNo ratings yet
- Chapter 11 Sense OrgansDocument5 pagesChapter 11 Sense Organszuni2008siddiquiNo ratings yet
- TBL 1 - Refractive Error SlidesDocument66 pagesTBL 1 - Refractive Error SlidesAmirah Azman100% (4)
- Two Major FormsDocument5 pagesTwo Major FormsKath CuevasNo ratings yet
- Blinking: A Slow-Motion Example of A Blinking Human EyeDocument4 pagesBlinking: A Slow-Motion Example of A Blinking Human EyeLando ParadaNo ratings yet
- Physiology of EyelidsDocument27 pagesPhysiology of EyelidsX And ZNo ratings yet
- The Eye 1Document42 pagesThe Eye 1Aunties Hyd Kka DeewanaNo ratings yet
- OCULAR PHYSIOLOGY 2021 Section B 2Document46 pagesOCULAR PHYSIOLOGY 2021 Section B 2Divine OkolieNo ratings yet
- Investrigatory Project (Term I) : Subject - BIOLOGYDocument20 pagesInvestrigatory Project (Term I) : Subject - BIOLOGYRehan RazaNo ratings yet
- Patho-II Lecture-IV Disorders of Special Senses (Eye & Ear)Document80 pagesPatho-II Lecture-IV Disorders of Special Senses (Eye & Ear)Muhammad ShayanNo ratings yet
- CHAPTER5 Form2Document14 pagesCHAPTER5 Form2basraawi379No ratings yet
- Physics Project: To Study The Optical Lens of A Human EyeDocument14 pagesPhysics Project: To Study The Optical Lens of A Human EyeAkash DhingraNo ratings yet
- Seminar On GlaucomaDocument26 pagesSeminar On GlaucomaPriya A100% (1)
- Biology Investigatory Project On Eye DiseasesDocument18 pagesBiology Investigatory Project On Eye DiseasesBHALAJI KARUNANITHI100% (1)
- Acknowledgement 3Document12 pagesAcknowledgement 3dankymemey96No ratings yet
- Visual-and-Auditory-FunctionDocument49 pagesVisual-and-Auditory-FunctionFAYE MITZI DELA FUENTENo ratings yet
- Most Frequently Asked Azure Data Factory Interview QuestionsDocument5 pagesMost Frequently Asked Azure Data Factory Interview QuestionsVijay Rajendiran0% (1)
- Top Kubernetes Interview Questions and AnswersDocument26 pagesTop Kubernetes Interview Questions and AnswersVijay RajendiranNo ratings yet
- 1691979146950Document10 pages1691979146950Vijay RajendiranNo ratings yet
- Annexure 2 - HL Joint Account DeclarationDocument1 pageAnnexure 2 - HL Joint Account DeclarationVijay RajendiranNo ratings yet
- Nokia Journey Management Guide EBrochure enDocument11 pagesNokia Journey Management Guide EBrochure enVijay RajendiranNo ratings yet
- Annexure 1 - TEMPLATE - RENT RECEIPTDocument1 pageAnnexure 1 - TEMPLATE - RENT RECEIPTVijay RajendiranNo ratings yet
- Country Health and Safety ManualDocument26 pagesCountry Health and Safety ManualVijay RajendiranNo ratings yet
- Azure Data Factory Interview Questions: Click HereDocument28 pagesAzure Data Factory Interview Questions: Click HereVijay RajendiranNo ratings yet
- Annexure 3 - Claiming Both HRA Exemption and Loss On House PropertyDocument1 pageAnnexure 3 - Claiming Both HRA Exemption and Loss On House PropertyVijay RajendiranNo ratings yet
- Balance Sheet UpdatedDocument4 pagesBalance Sheet UpdatedVijay RajendiranNo ratings yet
- Support in Planning DB MigrationDocument3 pagesSupport in Planning DB MigrationVijay RajendiranNo ratings yet
- How To Setup JmeterDocument9 pagesHow To Setup JmeterVijay RajendiranNo ratings yet
- Terraform Vs AnsibleDocument2 pagesTerraform Vs AnsibleVijay RajendiranNo ratings yet
- SQL Managed InstanceDocument3 pagesSQL Managed InstanceVijay RajendiranNo ratings yet
- Case Study - 2Document12 pagesCase Study - 2Vijay RajendiranNo ratings yet
- Case Study 1Document1 pageCase Study 1Vijay RajendiranNo ratings yet
- SQL Server Monitoring MetricsDocument2 pagesSQL Server Monitoring MetricsVijay RajendiranNo ratings yet
- Kidney: PDF Generated At: Sun, 26 Jan 2014 03:55:26 UTCDocument15 pagesKidney: PDF Generated At: Sun, 26 Jan 2014 03:55:26 UTCVijay RajendiranNo ratings yet
- DBMS Case Study IPL Pie in The Sky v2Document8 pagesDBMS Case Study IPL Pie in The Sky v2Vijay RajendiranNo ratings yet
- Bharat RatnaDocument6 pagesBharat RatnaVijay RajendiranNo ratings yet
- Saz3cDocument4 pagesSaz3cVijay RajendiranNo ratings yet
- Saz3cDocument4 pagesSaz3cVijay RajendiranNo ratings yet
- Parts of An Incandescent LampDocument7 pagesParts of An Incandescent Lamparchi.anne27No ratings yet
- Wave and Sond MCQ QuestionsDocument5 pagesWave and Sond MCQ Questionsmairaj24800100% (2)
- Class 5 Science 6 - Light and Sound NotesDocument2 pagesClass 5 Science 6 - Light and Sound NotesAnkur Kumar50% (2)
- Pysical Science: Group 4Document20 pagesPysical Science: Group 4Hanes PaulaNo ratings yet
- Colour Theory - SubhashiniDocument20 pagesColour Theory - Subhashinidineshduke678No ratings yet
- Direct OphthalmoscopeDocument16 pagesDirect OphthalmoscopeMuhammed AbdulmajeedNo ratings yet
- CRIMINALISTICS EditedDocument70 pagesCRIMINALISTICS EditedOnin RelacionNo ratings yet
- Science: Detailed Lesson Plan (DLP) FormatDocument11 pagesScience: Detailed Lesson Plan (DLP) FormatMaylord BonifacioNo ratings yet
- Comunications FundamentalsDocument271 pagesComunications FundamentalsDiego100% (1)
- Enhanced Science 10 Quarter 2 Chapter Test 1 - KEYDocument4 pagesEnhanced Science 10 Quarter 2 Chapter Test 1 - KEYMaam Katryn TanNo ratings yet
- ARRI Lighting Handbook EnglishDocument56 pagesARRI Lighting Handbook EnglishZiyahan ÇetinNo ratings yet
- Dual Nature of Radiation and Matter NewDocument10 pagesDual Nature of Radiation and Matter NewvjaNo ratings yet
- Dialux Project ReportDocument13 pagesDialux Project Reportvishwa9No ratings yet
- Physics - Unit Review Key TermsDocument4 pagesPhysics - Unit Review Key TermsJonny JiangNo ratings yet
- Ass 1 Robotics LecDocument6 pagesAss 1 Robotics Lec:PNo ratings yet
- Biomedical Photonics Handbook Volume 1 2nd Edition Vo-Dinh 2024 Scribd DownloadDocument70 pagesBiomedical Photonics Handbook Volume 1 2nd Edition Vo-Dinh 2024 Scribd Downloadpokalagashua100% (12)
- Physics Mcqs For Competitive Exams Part 1: ExamraceDocument3 pagesPhysics Mcqs For Competitive Exams Part 1: ExamraceFazlul RahmanNo ratings yet
- Kim Lighting B30 Series Bollard Brochure 1978Document20 pagesKim Lighting B30 Series Bollard Brochure 1978Alan MastersNo ratings yet
- Cie DS 014-4.3Document12 pagesCie DS 014-4.3Domenico AzzolliniNo ratings yet
- Bajaj LED Price List Jan 2019Document26 pagesBajaj LED Price List Jan 2019Iam VinitNo ratings yet
- Notes: Introduction To Light - Reflection & RefractionDocument10 pagesNotes: Introduction To Light - Reflection & RefractionShardul SumantNo ratings yet
- LED T8 Type B Spec SheetDocument5 pagesLED T8 Type B Spec SheetSERGIO ERIC RODRIGUEZNo ratings yet
- Secom Lighting New Products 2021Document29 pagesSecom Lighting New Products 2021amadbaeedlightingNo ratings yet
- Examination of The Patient - StereopsisDocument10 pagesExamination of The Patient - StereopsisJLoNo ratings yet
- Lesson Plan PhysicsDocument8 pagesLesson Plan PhysicsxoxkakidoxoxNo ratings yet
- MCQ For Fiber OpticsDocument4 pagesMCQ For Fiber OpticsMike Posktova100% (1)
- Choose The Best Options To Complete The Following SentencesDocument15 pagesChoose The Best Options To Complete The Following SentencesChang minNo ratings yet