2019 Nug
2019 Nug
Download as pdf or txt
You might also like
- Schoenbaum Implant Prosthetics in The Aesthetic Zone Science Protocol TechniquesDocument24 pagesSchoenbaum Implant Prosthetics in The Aesthetic Zone Science Protocol TechniquesЮля Колмакова100% (1)
- Biologically Oriented Preparation Technique (BOPT) : A Ne/a/ Approach For Prosthetic Restoration of Periodontically Healthy TeethDocument15 pagesBiologically Oriented Preparation Technique (BOPT) : A Ne/a/ Approach For Prosthetic Restoration of Periodontically Healthy TeethDr. Marica Ramona Elena100% (2)
- Tonetti Et Al-2018-Journal of Periodontology TDocument14 pagesTonetti Et Al-2018-Journal of Periodontology TJonathan Meza MauricioNo ratings yet
- Maintenance Therapy For Teeth and ImplantsDocument10 pagesMaintenance Therapy For Teeth and Implantspatricia sotoNo ratings yet
- Jurnal 1Document5 pagesJurnal 1iska yuliaNo ratings yet
- NUG Case Report UnlockedDocument10 pagesNUG Case Report UnlockedJohanNo ratings yet
- Kelompok 3 Prof SriDocument27 pagesKelompok 3 Prof SriKarma YogaNo ratings yet
- Artículo Perio InglésDocument9 pagesArtículo Perio InglésSteven TorresNo ratings yet
- Doença Periodontal e Saúde Sistêmica Uma Atualização para MédicosDocument8 pagesDoença Periodontal e Saúde Sistêmica Uma Atualização para Médicos8cv9jx4h8rNo ratings yet
- 1 s2.0 S0020653920322723 MainDocument6 pages1 s2.0 S0020653920322723 MainMarco Antonio García LunaNo ratings yet
- Enf Periondoltal 2017 PDFDocument15 pagesEnf Periondoltal 2017 PDFyenny2No ratings yet
- Treatment of Plaque-Induced Gingivitis, Chronic Periodontitis, and Other Clinical ConditionsDocument10 pagesTreatment of Plaque-Induced Gingivitis, Chronic Periodontitis, and Other Clinical ConditionsLeony RicciNo ratings yet
- Gingivitis: An Overall View For Undergraduate: November 2018Document12 pagesGingivitis: An Overall View For Undergraduate: November 2018Sannia SalsabilaNo ratings yet
- J Clinic Periodontology - 2018 - Chapple - Periodontal Health and Gingival Diseases and Conditions On An Intact and ADocument10 pagesJ Clinic Periodontology - 2018 - Chapple - Periodontal Health and Gingival Diseases and Conditions On An Intact and AAndreaNo ratings yet
- Lo 1 Pengaruh Penyakit Sistemik Terhadap Kesehatan Gigi Dan MulutDocument5 pagesLo 1 Pengaruh Penyakit Sistemik Terhadap Kesehatan Gigi Dan MulutTrie Andini ArianiNo ratings yet
- 7-Muller. 2019. Risk Factors For Recurrence of Periodontal Disease in Patients in Maintenance CareDocument9 pages7-Muller. 2019. Risk Factors For Recurrence of Periodontal Disease in Patients in Maintenance CarePaula YunesNo ratings yet
- Chapple Et Al-2018-Journal of Clinical Periodontology Grupo 1Document10 pagesChapple Et Al-2018-Journal of Clinical Periodontology Grupo 1Genesis Lopez torresNo ratings yet
- Ilovepdf Merged CompressedDocument99 pagesIlovepdf Merged CompressedCarina AidetNo ratings yet
- Gingivitis: November 2018Document14 pagesGingivitis: November 2018RamonaNo ratings yet
- Fdmed 03 994442Document7 pagesFdmed 03 994442ardanhehe9No ratings yet
- Periodontitis Classification and Staging PDFDocument9 pagesPeriodontitis Classification and Staging PDFAnonymous 7YkiHucQlONo ratings yet
- The Effect of Injectable Platelet-Rich Fibrin Use in TheDocument6 pagesThe Effect of Injectable Platelet-Rich Fibrin Use in TheNurul Fajriah YunitaNo ratings yet
- Treatment of Stage I-III Periodontitis-The EFP S3 Level Clinical Practice GuidelineDocument57 pagesTreatment of Stage I-III Periodontitis-The EFP S3 Level Clinical Practice GuidelinePaulina Müller100% (1)
- Gjermo 2009 Cost Effectiveness of Various TreatDocument7 pagesGjermo 2009 Cost Effectiveness of Various TreatSebastián BernalNo ratings yet
- Journal of Periodontology - ChappleDocument11 pagesJournal of Periodontology - ChapplelotblgxyvbzlunwvogNo ratings yet
- 2017 Chapple Periodontal Health and Gingival Diseases and Conditions On An Intact and A Reduced Periodontium Consensus ReportDocument10 pages2017 Chapple Periodontal Health and Gingival Diseases and Conditions On An Intact and A Reduced Periodontium Consensus ReportSANTIAGO URIBE GOMEZNo ratings yet
- Geriatrics and Periodontics: A Review: QR CodeDocument4 pagesGeriatrics and Periodontics: A Review: QR CodeDwi Septia RiniNo ratings yet
- Mucogingival Conditions in The Natural DentitionDocument9 pagesMucogingival Conditions in The Natural Dentitionclaudyedith197527No ratings yet
- Treatment guide_ periodontitis I-IIIDocument57 pagesTreatment guide_ periodontitis I-IIIPatapum125No ratings yet
- Case ReportDocument5 pagesCase ReportginNo ratings yet
- Parameters of Care Supplement: Parameter On "Refractory" PeriodontitisDocument2 pagesParameters of Care Supplement: Parameter On "Refractory" PeriodontitisEllis E. RamadianNo ratings yet
- Interactions Between Neutrophils and Periodontal Pathogens in Late-Onset PeriodontitisDocument11 pagesInteractions Between Neutrophils and Periodontal Pathogens in Late-Onset PeriodontitisAdriana NoelNo ratings yet
- Caso de Gingivitis - Diagnóstico AAP y FEPDocument24 pagesCaso de Gingivitis - Diagnóstico AAP y FEPCarina AidetNo ratings yet
- Diagnosis of Periodontal DiseasesDocument11 pagesDiagnosis of Periodontal Diseasesphoenix0471No ratings yet
- Ijd2021 2810264Document12 pagesIjd2021 2810264KarthikaNo ratings yet
- Critical Review of 2017 Classification of Periodontal and Peri-Implant Diseases and ConditionsDocument8 pagesCritical Review of 2017 Classification of Periodontal and Peri-Implant Diseases and ConditionsKarthikaNo ratings yet
- Periodontal Disease FKG Unissula 2011Document2 pagesPeriodontal Disease FKG Unissula 2011claudianrjNo ratings yet
- Efficacy of Photodynamic Therapy and Periodontal TDocument10 pagesEfficacy of Photodynamic Therapy and Periodontal Thafizhuddin muhammadNo ratings yet
- Article 1443719054Document11 pagesArticle 1443719054antariksha DodNo ratings yet
- Tonetti Et Al-2015-Journal of Clinical PeriodontologyDocument7 pagesTonetti Et Al-2015-Journal of Clinical PeriodontologyDiana IorgulescuNo ratings yet
- Journal of Controlled ReleaseDocument14 pagesJournal of Controlled ReleaseRachmawati Dian PuspitasariNo ratings yet
- 2 ND JC PDF - SindhuDocument8 pages2 ND JC PDF - SindhuDadi SindhuNo ratings yet
- Jper 17-0733Document12 pagesJper 17-0733Jonathan Meza MauricioNo ratings yet
- 259acf9f83366abf511adcab54088a39Document13 pages259acf9f83366abf511adcab54088a39alfasrasimp123No ratings yet
- Step 1 for the Treatment of Periodontal DiseasesDocument7 pagesStep 1 for the Treatment of Periodontal DiseasesMohamed YousryNo ratings yet
- Current Concepts in The Management of Periodontitis: Concise Clinical ReviewDocument15 pagesCurrent Concepts in The Management of Periodontitis: Concise Clinical ReviewAlexandru Codrin-IonutNo ratings yet
- Terapia Periodontal No QuirúrgicaDocument6 pagesTerapia Periodontal No QuirúrgicaMaria Paula Vanegas ForeroNo ratings yet
- Oral and Dental HealthDocument10 pagesOral and Dental HealthannisaramadantiNo ratings yet
- Distribusi Gingivitis Pada Pasien SkizofreniaDocument6 pagesDistribusi Gingivitis Pada Pasien SkizofreniafaniaNo ratings yet
- Relationship Between Diabetes and Periodontal Infection: DOI: 10.4239/wjd.v6.i7.927 ISSN 1948-9358 (Online)Document10 pagesRelationship Between Diabetes and Periodontal Infection: DOI: 10.4239/wjd.v6.i7.927 ISSN 1948-9358 (Online)Luthfi PrimadaniNo ratings yet
- The Prevention of Periodontal Disease-An Overview: Frank A. Scannapieco - Eva GershovichDocument5 pagesThe Prevention of Periodontal Disease-An Overview: Frank A. Scannapieco - Eva GershovichLauraBotnariNo ratings yet
- J Clinic Periodontology - 2020 - Loos - Endpoints of Active Periodontal TherapyDocument11 pagesJ Clinic Periodontology - 2020 - Loos - Endpoints of Active Periodontal Therapy2025mohammadashkananiNo ratings yet
- Jurnal NUPDocument10 pagesJurnal NUPsusi apriliantyNo ratings yet
- Microorganisms 10 00337 1Document16 pagesMicroorganisms 10 00337 1Maysaa mahdiNo ratings yet
- J Clinic Periodontology - 2018 - Trombelli - Plaque Induced Gingivitis Case Definition and Diagnostic ConsiderationsDocument24 pagesJ Clinic Periodontology - 2018 - Trombelli - Plaque Induced Gingivitis Case Definition and Diagnostic Considerationsdaniel15056No ratings yet
- ClassificationDocument43 pagesClassificationsidra malikNo ratings yet
- Periodontitis- Consensus report of workgroup 2 of the 2017 World Workshop on the Classification of Periodontal and Peri‐Implant Diseases and Conditions - Papapanou - 2018 - Journal of Periodontology - Wiley Online LibraryDocument17 pagesPeriodontitis- Consensus report of workgroup 2 of the 2017 World Workshop on the Classification of Periodontal and Peri‐Implant Diseases and Conditions - Papapanou - 2018 - Journal of Periodontology - Wiley Online Libraryandrea guillénNo ratings yet
- Case Report: Generalized Aggressive Periodontitis and Its Treatment Options: Case Reports and Review of The LiteratureDocument18 pagesCase Report: Generalized Aggressive Periodontitis and Its Treatment Options: Case Reports and Review of The LiteratureBlackNo ratings yet
- Clasificacion de Enf 2017Document10 pagesClasificacion de Enf 2017Jonathan Meza MauricioNo ratings yet
- Understanding Periodontitis: A Comprehensive Guide to Periodontal Disease for Dentists, Dental Hygienists and Dental PatientsFrom EverandUnderstanding Periodontitis: A Comprehensive Guide to Periodontal Disease for Dentists, Dental Hygienists and Dental PatientsNo ratings yet
- Periodontal Health and Implantology: A Comprehensive Guide to Diagnosis, Treatment, and InnovationsFrom EverandPeriodontal Health and Implantology: A Comprehensive Guide to Diagnosis, Treatment, and InnovationsNo ratings yet
- Role of Genetic in Periodontal Disease PDFDocument6 pagesRole of Genetic in Periodontal Disease PDFkhairunnisa ANo ratings yet
- Jurnal Om AccDocument8 pagesJurnal Om Acckhairunnisa ANo ratings yet
- Lateral Luxation of A Permanent Mature Incisor in A Thirteen Year Old Male Patient A Case ReportDocument5 pagesLateral Luxation of A Permanent Mature Incisor in A Thirteen Year Old Male Patient A Case Reportkhairunnisa ANo ratings yet
- Slob RuleDocument31 pagesSlob Rulekhairunnisa ANo ratings yet
- 1 s2.0 S1013905219305280 MainDocument5 pages1 s2.0 S1013905219305280 Mainkhairunnisa ANo ratings yet
- Bio Mechanics of Tooth PreparationDocument151 pagesBio Mechanics of Tooth PreparationJasbrinder Singh TejaNo ratings yet
- 001 - 01 - DR Michael Melkers - Occlusion in Everyday PracticeDocument32 pages001 - 01 - DR Michael Melkers - Occlusion in Everyday PracticeMinh ThongNo ratings yet
- Inflamatory Periaical Cyst Formation and ManagementDocument25 pagesInflamatory Periaical Cyst Formation and ManagementL C K GokuNo ratings yet
- Stratos 300Document104 pagesStratos 300Scott O'HaraNo ratings yet
- GD Comparison of Profile Attractiveness Between Class III Orthodontic Camouflage and Predictive Tracing of Orthognathic Surgery, Wadi 2020Document9 pagesGD Comparison of Profile Attractiveness Between Class III Orthodontic Camouflage and Predictive Tracing of Orthognathic Surgery, Wadi 2020GeromelNo ratings yet
- A Comparison of One Versus Two Appointment EndodonticDocument6 pagesA Comparison of One Versus Two Appointment EndodonticShurinam Zaidel Sinain MadariagaNo ratings yet
- 6Laboratory Procedures Of Removable Partial Dentures-1Document44 pages6Laboratory Procedures Of Removable Partial Dentures-1mustafa.selim98No ratings yet
- Lec 17 04/06/2020 Prosthetic Dentistry DR Farah NabeelDocument11 pagesLec 17 04/06/2020 Prosthetic Dentistry DR Farah NabeelSilva ZikroNo ratings yet
- International Association of Pediatric Dentistry - Children 0-2 Years of AgeDocument14 pagesInternational Association of Pediatric Dentistry - Children 0-2 Years of AgeMafe SalazarNo ratings yet
- Freedom in CentricDocument6 pagesFreedom in CentricTarannum Jindal100% (1)
- Patient Instructions IDDocument2 pagesPatient Instructions IDGabriel SciberrasNo ratings yet
- Hayrax Con Mascara Facial PDFDocument8 pagesHayrax Con Mascara Facial PDFSantos LopNo ratings yet
- PedoDocument14 pagesPedoHarjotBrarNo ratings yet
- Mcqsperiodontology Gingivitis 180129101534Document15 pagesMcqsperiodontology Gingivitis 180129101534Asad Khan5556No ratings yet
- Article On Functional ApplianceDocument10 pagesArticle On Functional Applianceaddy yNo ratings yet
- Section 014 Functionally Generated PathDocument7 pagesSection 014 Functionally Generated PathAmar Bhochhibhoya100% (1)
- Mouth Care After Stroke: Oral HealthDocument5 pagesMouth Care After Stroke: Oral HealthYuganya SriNo ratings yet
- Maxillary Canine - First Premolar Transposition, Associated Dental Anomalies and Genetic BasisDocument11 pagesMaxillary Canine - First Premolar Transposition, Associated Dental Anomalies and Genetic BasisMartha Lia Castaño EcheverryNo ratings yet
- Kanika Album CasesDocument55 pagesKanika Album Casesmahima gupta100% (1)
- The Development of The Endodontic Complexity Assessment Tool (E-CAT) - 2018Document193 pagesThe Development of The Endodontic Complexity Assessment Tool (E-CAT) - 2018bogdimNo ratings yet
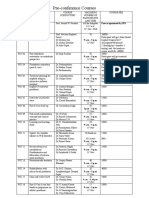
- Pre-Conference Courses: Free As Sponsored by IPSDocument2 pagesPre-Conference Courses: Free As Sponsored by IPSShria DhaonNo ratings yet
- Long-Term Stability Postretention Changesof The Mandibular Anterior TeethDocument10 pagesLong-Term Stability Postretention Changesof The Mandibular Anterior Teethyerly ramirezNo ratings yet
- Tokuyama Clinical CasesDocument170 pagesTokuyama Clinical CasesEdson HoribeNo ratings yet
- Dr/Ahmed Yehia: Personal InformationDocument3 pagesDr/Ahmed Yehia: Personal Informationlaura cebucNo ratings yet
- A Facially Driven Complete-Mouth Rehabilitation With Ultrathin CAD CAM Composite Resin Veneers For A Patient With Severe Tooth Wear A Minimally Invasive ApproachDocument11 pagesA Facially Driven Complete-Mouth Rehabilitation With Ultrathin CAD CAM Composite Resin Veneers For A Patient With Severe Tooth Wear A Minimally Invasive ApproachAlex Gutierrez AcostaNo ratings yet
- DENTAL CEMENTS (Silicate & Zinc Phosphate)Document4 pagesDENTAL CEMENTS (Silicate & Zinc Phosphate)JEANASHLEY PUNZALANNo ratings yet
- Jones 1997 Chlorhexidine: Is It Still The Gold Standard?Document8 pagesJones 1997 Chlorhexidine: Is It Still The Gold Standard?Phuong ThaoNo ratings yet
- Physiology of Tooth Form: FunctionDocument1 pagePhysiology of Tooth Form: FunctionTayyuba AslamNo ratings yet