0% found this document useful (0 votes)
177 viewsThe Eye and Vision
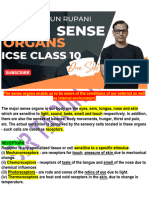
The eye functions similarly to a camera, with light passing through the cornea, pupil, and lens before hitting the retina. The iris controls the size of the pupil to regulate the amount of light. On the retina are light-sensitive rods and cones which allow vision. The lens focuses light onto the fovea for sharp central vision. Night vision relies more on rods, while cones provide color vision and are used in bright light. The eye continuously adapts between light and dark conditions for optimal vision.
Uploaded by
Ledkos SLCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as PDF, TXT or read online on Scribd
0% found this document useful (0 votes)
177 viewsThe Eye and Vision
The eye functions similarly to a camera, with light passing through the cornea, pupil, and lens before hitting the retina. The iris controls the size of the pupil to regulate the amount of light. On the retina are light-sensitive rods and cones which allow vision. The lens focuses light onto the fovea for sharp central vision. Night vision relies more on rods, while cones provide color vision and are used in bright light. The eye continuously adapts between light and dark conditions for optimal vision.
Uploaded by
Ledkos SLCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as PDF, TXT or read online on Scribd
/ 70