Assignment ON Advanced Cardiac Life Support: Submitted To: Submitted by
Assignment ON Advanced Cardiac Life Support: Submitted To: Submitted by
Download as docx, pdf, or txt
You might also like
- Booty by Bret Month 62Document6 pagesBooty by Bret Month 62moniquesmith90100% (1)
- Seminar On PacemakerDocument14 pagesSeminar On Pacemakerjyothi50% (4)
- Peripheral Artery Disease: Nikhil Vaishnav M.Sc. (Nursing)Document70 pagesPeripheral Artery Disease: Nikhil Vaishnav M.Sc. (Nursing)Dimpal ChoudharyNo ratings yet
- Cardio Pulmonary ResuscitationDocument13 pagesCardio Pulmonary Resuscitationaparna100% (1)
- Endotracheal IntubationDocument4 pagesEndotracheal Intubationrupali gahalianNo ratings yet
- Abg AnalysisDocument9 pagesAbg AnalysisLakshmi RjNo ratings yet
- ETT IntubationDocument10 pagesETT IntubationPoova RagavanNo ratings yet
- Arterial CatheterizationDocument5 pagesArterial CatheterizationSREEDEVI T SURESHNo ratings yet
- Pulse Oximetry IDocument4 pagesPulse Oximetry IFriends Forever100% (1)
- Assignment ON: TOPIC: PTCA (Percutaneous Transluminous Coronary Angioplasty)Document7 pagesAssignment ON: TOPIC: PTCA (Percutaneous Transluminous Coronary Angioplasty)soniya josephNo ratings yet
- Pulse OximetryDocument10 pagesPulse OximetryR.vijay100% (1)
- Endotracheal IntubationDocument11 pagesEndotracheal Intubationanon_784834955100% (1)
- Assignment On TRACHEOSTOMYDocument12 pagesAssignment On TRACHEOSTOMYPrasann Roy100% (2)
- Assignment On Radiation TherapyDocument16 pagesAssignment On Radiation TherapyAxsa AlexNo ratings yet
- Seminar On CV Thoracic SurgeriesDocument81 pagesSeminar On CV Thoracic SurgeriesMegha lakraNo ratings yet
- ENDOTRACHEAL INTUBATIOn SandeepDocument17 pagesENDOTRACHEAL INTUBATIOn SandeepSimran JosanNo ratings yet
- Endotracheal Tube IntubationDocument5 pagesEndotracheal Tube IntubationKim Kristine D. GuillenNo ratings yet
- Coronary Care Unit/ Cardiac Care Unit: Patient MonitorsDocument3 pagesCoronary Care Unit/ Cardiac Care Unit: Patient MonitorsPhoebe Kyles Camma100% (1)
- PainDocument20 pagesPainvinnu kalyanNo ratings yet
- Mechanical VentilationDocument16 pagesMechanical VentilationBhawna JoshiNo ratings yet
- Endotracheal IntubationDocument17 pagesEndotracheal IntubationShiwangi Sharma100% (2)
- Cardiomyopathy SeminarDocument17 pagesCardiomyopathy SeminarJyoti SinghNo ratings yet
- CVP MonitoringDocument7 pagesCVP Monitoringgurneet kourNo ratings yet
- Lumber Puncture ProcedureDocument8 pagesLumber Puncture ProcedureDimpal ChoudharyNo ratings yet
- Assisting With Abdominal ParacentesisDocument14 pagesAssisting With Abdominal ParacentesisMegha lakra100% (1)
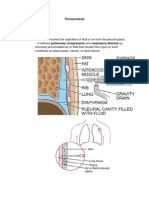
- ThoracentesisDocument9 pagesThoracentesisPatricia G ChiuNo ratings yet
- Clinical Presentation On PnemoniaDocument37 pagesClinical Presentation On PnemoniasreekalaNo ratings yet
- Advanced Cardiac ProcedureDocument9 pagesAdvanced Cardiac ProcedureSachin DwivediNo ratings yet
- Central Venous Line CareDocument13 pagesCentral Venous Line CarePaul Henry RoxasNo ratings yet
- Pulseoxymeter: College of Nursing Madurai Medical College Madurai-20 Procedure Demonstration ONDocument16 pagesPulseoxymeter: College of Nursing Madurai Medical College Madurai-20 Procedure Demonstration ONValarmathi100% (7)
- TRACHEOSTOMY CARE (Repaired) (Repaired)Document18 pagesTRACHEOSTOMY CARE (Repaired) (Repaired)DhAiRyA ArOrANo ratings yet
- TracheostomyDocument6 pagesTracheostomynamithaNo ratings yet
- Assignment On DislysisDocument10 pagesAssignment On DislysisSanhati Ghosh Banerjee100% (1)
- 07.04.05 Venturi Face MaskDocument2 pages07.04.05 Venturi Face MaskRosintchi MirsalNo ratings yet
- Pulse OximetryDocument3 pagesPulse OximetryJanna Favila100% (3)
- CPCRDocument36 pagesCPCRapi-1991639933% (3)
- Lesson Plan On Cor PulmonaleDocument49 pagesLesson Plan On Cor PulmonaleRadha Sri50% (2)
- Bharati Vidyapeeth College of Nursing Navi Mumbai: Assignment On MriDocument6 pagesBharati Vidyapeeth College of Nursing Navi Mumbai: Assignment On MriKhirabdhi Tanaya SahuNo ratings yet
- Endotracheal IntubationDocument7 pagesEndotracheal Intubationsimonjosan75% (4)
- Equipment EditedDocument6 pagesEquipment EditedCHRISTINE JOY. MOLINANo ratings yet
- Assignment ON Tracheostom Y Care: Submitted To: Submitted byDocument5 pagesAssignment ON Tracheostom Y Care: Submitted To: Submitted byAnanthibala100% (1)
- Arterial Blood Gas (Abg) Analysis: Submitted ToDocument5 pagesArterial Blood Gas (Abg) Analysis: Submitted ToRumela ChakrabortyNo ratings yet
- Assignment On CT, MRI, EEGDocument14 pagesAssignment On CT, MRI, EEGManisha Samson100% (3)
- Cardiac CatheterizationDocument25 pagesCardiac CatheterizationQueeny Anne ApilNo ratings yet
- Care of Client in Mechanical VentilatorDocument11 pagesCare of Client in Mechanical VentilatorVignesh Viggy100% (4)
- Thoracocentasis: INTRODUCTION:-Thoracentasis Also Known As The Thoracocentasis or Plural Tap Is AnDocument7 pagesThoracocentasis: INTRODUCTION:-Thoracentasis Also Known As The Thoracocentasis or Plural Tap Is AnaparnaNo ratings yet
- Sub - Medical Surgical Nursing: Assignment On CVP MonitoringDocument11 pagesSub - Medical Surgical Nursing: Assignment On CVP Monitoringkamini ChoudharyNo ratings yet
- Assignment ON MyelographyDocument12 pagesAssignment ON MyelographyDiana CharaNo ratings yet
- Hemodynamic Monitoring 1Document10 pagesHemodynamic Monitoring 1Savita HanamsagarNo ratings yet
- Mechanical VentilationDocument9 pagesMechanical VentilationFriends ForeverNo ratings yet
- Haemodynamic MonitoringDocument6 pagesHaemodynamic MonitoringAnusha Verghese100% (1)
- Defibrillation TypedDocument8 pagesDefibrillation TypedValarmathiNo ratings yet
- Adrenal Crisis FinalDocument10 pagesAdrenal Crisis FinalAmanda Scarlet100% (1)
- PacemakerDocument26 pagesPacemakerAswathy RCNo ratings yet
- Assignment On Abdominal ParacentesisDocument9 pagesAssignment On Abdominal ParacentesisAxsa AlexNo ratings yet
- Abdominal ParacentesisDocument14 pagesAbdominal ParacentesisManisha Thakur100% (1)
- SUBMITTED TO - Resp. Mr. Somorjit SinghDocument8 pagesSUBMITTED TO - Resp. Mr. Somorjit SinghSimran JosanNo ratings yet
- Caring For Your Jejunostomy Feeding Tube - Feb22Document6 pagesCaring For Your Jejunostomy Feeding Tube - Feb22Buvana VigneshNo ratings yet
- Cardio Pulmonary Resuscitation and End of Life CareDocument22 pagesCardio Pulmonary Resuscitation and End of Life CareAnitha sujithNo ratings yet
- CVP Line CareDocument37 pagesCVP Line CareArvindJoshiNo ratings yet
- Econdary ABCD (Airway, Breathing, Circulation, Differential Diagnosis)Document20 pagesEcondary ABCD (Airway, Breathing, Circulation, Differential Diagnosis)Nikol NataliaNo ratings yet
- Health Assessment ON Gastro Intestinal System: Submitted To: Submitted byDocument13 pagesHealth Assessment ON Gastro Intestinal System: Submitted To: Submitted byAnanthibalaNo ratings yet
- Assignment ON Tracheostom Y Care: Submitted To: Submitted byDocument5 pagesAssignment ON Tracheostom Y Care: Submitted To: Submitted byAnanthibala100% (1)
- Health Assessment ON Genito Urinary System: Submitted To: Submitted byDocument16 pagesHealth Assessment ON Genito Urinary System: Submitted To: Submitted byAnanthibalaNo ratings yet
- Game (Ballon Game)Document3 pagesGame (Ballon Game)AnanthibalaNo ratings yet
- Specific Objevtive Content AV Aids Time Teachin G Learnin G Activit Y Evaluatio NDocument25 pagesSpecific Objevtive Content AV Aids Time Teachin G Learnin G Activit Y Evaluatio NAnanthibalaNo ratings yet
- Cholecystitis Cholelithiasis-PresentationDocument1 pageCholecystitis Cholelithiasis-PresentationAnanthibalaNo ratings yet
- Alinhamento Inferior Arcos JulioDocument6 pagesAlinhamento Inferior Arcos JulioDiego Andres Hincapie HerreraNo ratings yet
- Child Nursing CareDocument3 pagesChild Nursing Carelina solihanNo ratings yet
- SITHKOP012 Dietary Requirements Lifestyle 2Document5 pagesSITHKOP012 Dietary Requirements Lifestyle 2Ankit BhattraiNo ratings yet
- Susi Sa PagwawastoDocument2 pagesSusi Sa PagwawastoMarylove Beb EloniaNo ratings yet
- hw420 Unit 9 AssignmentDocument12 pageshw420 Unit 9 Assignmentapi-569132011No ratings yet
- Module 7 STSDocument9 pagesModule 7 STSJan Marvin AclanNo ratings yet
- US Army Boxing - West Point Trainers Manual 51pDocument51 pagesUS Army Boxing - West Point Trainers Manual 51pLo Shun Fat100% (1)
- RolesDocument117 pagesRolesMarycon DuldulaoNo ratings yet
- Master List MaxicareDocument12 pagesMaster List Maxicareprincess1309No ratings yet
- Sample Test 1Document12 pagesSample Test 1Bünyamin EmerNo ratings yet
- High An Low Fidelity Simulation For Clinical Skill in Paramedic Students in Resource Limited SettingsDocument11 pagesHigh An Low Fidelity Simulation For Clinical Skill in Paramedic Students in Resource Limited SettingsVictoriano MendezNo ratings yet
- Boehringer Ingelheim - Project Manager - Making More HealthDocument1 pageBoehringer Ingelheim - Project Manager - Making More HealthMoses MosesNo ratings yet
- ENGLISH-10 Q3 Mod1.1 USLeM-RTPDocument9 pagesENGLISH-10 Q3 Mod1.1 USLeM-RTPMikaella Jade MempinNo ratings yet
- Ibrahim Rawhi Ayasreh - Case PresentationDocument41 pagesIbrahim Rawhi Ayasreh - Case PresentationIbrahim R. AyasrehNo ratings yet
- FOS Lesson PlanDocument6 pagesFOS Lesson PlanReymond SumayloNo ratings yet
- Visa 1 - Study Habits QuestionnaireDocument7 pagesVisa 1 - Study Habits Questionnairejane austin lynn rebancos100% (1)
- BSN 1 Procedure ChecklistDocument25 pagesBSN 1 Procedure ChecklistSteve EstebanNo ratings yet
- (5A) RA 4688 - Clinical Laboratory Act of 1966Document2 pages(5A) RA 4688 - Clinical Laboratory Act of 1966ella hullezaNo ratings yet
- Jurnal Bing 3Document11 pagesJurnal Bing 3Abangnya Dea AmandaNo ratings yet
- Modified Internal Medicine History Taking and Physical Examinations TemplateDocument5 pagesModified Internal Medicine History Taking and Physical Examinations Templatemotasem.med120No ratings yet
- Afaq EngineeringDocument17 pagesAfaq EngineeringHardesinah Habdulwaheed HoluwasegunNo ratings yet
- MuscleBlaze - Bright Life Care PVT LTDDocument14 pagesMuscleBlaze - Bright Life Care PVT LTDAlisha AnandNo ratings yet
- Personality and PerceptionDocument30 pagesPersonality and PerceptionUmar Shabir BaigNo ratings yet
- Principles of Bach Flower Remedies (Stefan Ball)Document138 pagesPrinciples of Bach Flower Remedies (Stefan Ball)Rita Gomes100% (2)
- Mental Health - FL - 530 - Factsheet - SI - enDocument2 pagesMental Health - FL - 530 - Factsheet - SI - eneanahanaNo ratings yet
- Konten Layanan BLDocument6 pagesKonten Layanan BLAria WibowoNo ratings yet
- Ai 9 SCDocument288 pagesAi 9 SCsaksham3.14159piNo ratings yet
- Paket APP, HERNIA Dan WIDE (Ada Harga Per Tindakan)Document54 pagesPaket APP, HERNIA Dan WIDE (Ada Harga Per Tindakan)Bagus TriagungNo ratings yet
- Certification Exam Candidate HandbookDocument44 pagesCertification Exam Candidate HandbookNazmul IslamNo ratings yet