Effectiveness of Speech Therapy in The Treatment of Vocal Fold Polyps
Effectiveness of Speech Therapy in The Treatment of Vocal Fold Polyps
Download as pdf or txt
You might also like
- An Eclectic Voice Therapy Program For The Treatment of Hyperfunctional Voice Disorders (HFVD)Document21 pagesAn Eclectic Voice Therapy Program For The Treatment of Hyperfunctional Voice Disorders (HFVD)daniel morenoNo ratings yet
- Treatment of Wernicke'S Aphasia With Jargon: A Case StudyDocument11 pagesTreatment of Wernicke'S Aphasia With Jargon: A Case StudyIvanaNo ratings yet
- 1 s2.0 S0892199723002138 MainDocument8 pages1 s2.0 S0892199723002138 MainKübra YelgeçNo ratings yet
- 2017 Vasconcelos Et Al Treatment For Vocal Polyps Lips and Tongue Trill J VoiceDocument10 pages2017 Vasconcelos Et Al Treatment For Vocal Polyps Lips and Tongue Trill J VoiceFlor SilvaNo ratings yet
- Voice TherapybookwebDocument23 pagesVoice TherapybookwebPola Constanza100% (2)
- Artigo 20 - Quantifying Component Parts of Indirect and Direct Voice Therapy Related To Different Voice DisordersDocument7 pagesArtigo 20 - Quantifying Component Parts of Indirect and Direct Voice Therapy Related To Different Voice DisordersAna Carolina MachucaNo ratings yet
- Treatment For Vocal Polyps Lips and Tongue TrillDocument11 pagesTreatment For Vocal Polyps Lips and Tongue TrillJulia GavrashenkoNo ratings yet
- Does A Specialist Voice Clinic Change ENT Clinic Diagnosis?Document4 pagesDoes A Specialist Voice Clinic Change ENT Clinic Diagnosis?sibel yıldırımNo ratings yet
- Does Voice Therapy Cure All Vocal Fold Nodules?: Ijopl IjoplDocument5 pagesDoes Voice Therapy Cure All Vocal Fold Nodules?: Ijopl IjoplDesi Ratnasari EndangNo ratings yet
- Strech and Flow TherapyDocument9 pagesStrech and Flow TherapysopranopatriciaNo ratings yet
- 1 s2.0 S0892199714000654 MainDocument4 pages1 s2.0 S0892199714000654 MainakhileshNo ratings yet
- Effects of Voice Therapy Using The Lip Trill Technique in P - 2019 - Journal ofDocument9 pagesEffects of Voice Therapy Using The Lip Trill Technique in P - 2019 - Journal ofJulia GavrashenkoNo ratings yet
- Cia 14 453Document19 pagesCia 14 453soriamartinpaulaNo ratings yet
- Speech Language Pathology RehabilitationDocument14 pagesSpeech Language Pathology RehabilitationFelipe UrbanoNo ratings yet
- Professional Voices and Functional FrenuloplastyDocument10 pagesProfessional Voices and Functional FrenuloplastyBella 234No ratings yet
- 2016, Pedrosa Et Al, The Effectiveness of Comprehensive Voice, J VoiceDocument9 pages2016, Pedrosa Et Al, The Effectiveness of Comprehensive Voice, J VoiceCarol PaesNo ratings yet
- Lms DLSDLDocument9 pagesLms DLSDLllllllllNo ratings yet
- Gie Rut 2001Document13 pagesGie Rut 2001vrtdpgbbhxNo ratings yet
- Simic 2020 Anomia Treatment OutcomesDocument23 pagesSimic 2020 Anomia Treatment OutcomesMiniNo ratings yet
- Voice Therapy Does Science Support The ArtDocument1 pageVoice Therapy Does Science Support The ArtEvelyn Bernardita Avello CuevasNo ratings yet
- Voice Therapy Does Science Support The ArtDocument5 pagesVoice Therapy Does Science Support The ArtYurleidys ZapaNo ratings yet
- Efficacy of Doctorvox On Mutational FalsettoDocument8 pagesEfficacy of Doctorvox On Mutational FalsettoANA CRISTINA MENDEZ DIAZNo ratings yet
- Efectos de La Terapia en Disfonia Musculotensional.2017Document7 pagesEfectos de La Terapia en Disfonia Musculotensional.2017Jenith Karem Paredes GonzalezNo ratings yet
- Da Cunha Pereira 2017Document7 pagesDa Cunha Pereira 2017Pablo Andrés Sánchez MonsalveNo ratings yet
- LKSV LksDocument8 pagesLKSV LksllllllllNo ratings yet
- W ' E O M T ?: HAT S The Vidence For RAL Otor HerapyDocument2 pagesW ' E O M T ?: HAT S The Vidence For RAL Otor HerapyAdrian UluNo ratings yet
- Effectiveness of Semi-Occluded Vocal Tract Exercises (Sovtes) in Patients With Dysphonia: A Systematic Review and Meta-AnalysisDocument19 pagesEffectiveness of Semi-Occluded Vocal Tract Exercises (Sovtes) in Patients With Dysphonia: A Systematic Review and Meta-AnalysisDANIELA IGNACIA FERNÁNDEZ LEÓNNo ratings yet
- Text 2. White Carding 2020 - Pre and Post-TherapyDocument9 pagesText 2. White Carding 2020 - Pre and Post-Therapyjulyamacedo2020No ratings yet
- Retraining Speech Production and Fluency in Non Fluent-Agrammatic Primary Progressive Aphasia.Document16 pagesRetraining Speech Production and Fluency in Non Fluent-Agrammatic Primary Progressive Aphasia.MiniNo ratings yet
- 1 s2.0 S0892199723002643 MainDocument12 pages1 s2.0 S0892199723002643 MaincdNo ratings yet
- Efficacy of Conversation Training TherapyDocument18 pagesEfficacy of Conversation Training Therapyjulyamacedo2020No ratings yet
- Acoustic Analysis of Four Common Voice Diagnoses Moving Toward Disorder Specific Assessment - 2014 - Journal of VoiceDocument7 pagesAcoustic Analysis of Four Common Voice Diagnoses Moving Toward Disorder Specific Assessment - 2014 - Journal of VoicericardobuhrerNo ratings yet
- Effectiveness of Sound Production Treatment Nicole PoundsDocument5 pagesEffectiveness of Sound Production Treatment Nicole Poundsthe chichNo ratings yet
- Manejo de La Tos CronicaDocument6 pagesManejo de La Tos CronicaThomasMáximoMancinelliRinaldoNo ratings yet
- Long-Term Maintenance of Anomia Treatment Effects inDocument26 pagesLong-Term Maintenance of Anomia Treatment Effects inHarumy NakayamaNo ratings yet
- 2 VIM - in - Voice - TherapyDocument7 pages2 VIM - in - Voice - TherapyLaura MontenegroNo ratings yet
- 2016 1221451Document16 pages2016 1221451童ㄊㄊNo ratings yet
- 2020) Transcutaneous Electrical Nerve Stimulation in Dysphonic Patients A Systematic ReviewDocument10 pages2020) Transcutaneous Electrical Nerve Stimulation in Dysphonic Patients A Systematic ReviewFlga Claudia ZúñigaNo ratings yet
- Vocal Improvement After Voice Therapy in Unilateral Vocal Fold ParalysisDocument6 pagesVocal Improvement After Voice Therapy in Unilateral Vocal Fold ParalysisAngela Lleuful ToledoNo ratings yet
- Voice Therapy OutcomeDocument10 pagesVoice Therapy Outcomemajid mirzaeeNo ratings yet
- Roles of Speech-Language Pathologists in Swallowing and Feeding DisordersDocument31 pagesRoles of Speech-Language Pathologists in Swallowing and Feeding DisordersAgostina MaggiNo ratings yet
- 10 1016@j Jvoice 2006 09 009 PDFDocument5 pages10 1016@j Jvoice 2006 09 009 PDFfcabelloluqueNo ratings yet
- Dreyer Et Al 2020 Increased Recruitment of Domain General Neural Networks in Language Processing Following IntensiveDocument11 pagesDreyer Et Al 2020 Increased Recruitment of Domain General Neural Networks in Language Processing Following Intensivekailaiii626No ratings yet
- Effects of Vocal Exercises On The Treatment of Dysphagia - Integrative ReviewDocument9 pagesEffects of Vocal Exercises On The Treatment of Dysphagia - Integrative ReviewESTEFANIA GEOVANNA MEJIA MACASNo ratings yet
- Relationship Between Fatigue, Perfectionism, and Functional DysphoniaDocument6 pagesRelationship Between Fatigue, Perfectionism, and Functional DysphoniaMuhamad AriefNo ratings yet
- Intensive Versus Traditional Voice Therapy For VocalDocument14 pagesIntensive Versus Traditional Voice Therapy For VocalAnonymous xvlg4m5xLXNo ratings yet
- Effectiveness of Voice Therapy in Patients With Vocal Fold Nodules - A Systematic Search and Narrative ReviewDocument16 pagesEffectiveness of Voice Therapy in Patients With Vocal Fold Nodules - A Systematic Search and Narrative Reviewdaniel morenoNo ratings yet
- Efficacy of Myofunctional Therapy Associated With Voice Therapy in The Rehabilitation of Neurogenic Oropharyngeal Dysphagia: A Pilot StudyDocument6 pagesEfficacy of Myofunctional Therapy Associated With Voice Therapy in The Rehabilitation of Neurogenic Oropharyngeal Dysphagia: A Pilot StudyÁnyela H. Merchán MendozaNo ratings yet
- Carroll 2Document19 pagesCarroll 2Anonymous JonAFVUi4100% (1)
- Chewing Technique in Phonation of SLP StudentsDocument5 pagesChewing Technique in Phonation of SLP Studentsmajid mirzaeeNo ratings yet
- Acquired Apraxia of Speech Treatment Overview PDFDocument12 pagesAcquired Apraxia of Speech Treatment Overview PDFHaroun Krilov-Egbert100% (1)
- PeterDocument5 pagesPeterErsya MuslihNo ratings yet
- Vocal Fold MassesDocument18 pagesVocal Fold Massesapi-19500641No ratings yet
- Singing Exercises For Speech and Vocal AbilitiesDocument10 pagesSinging Exercises For Speech and Vocal Abilitiesapi-538965270No ratings yet
- Motor-Learning-Based Adjustment of AmbulatoryDocument9 pagesMotor-Learning-Based Adjustment of AmbulatoryHectorMoNo ratings yet
- Logopedia Post QXDocument6 pagesLogopedia Post QXlogopedamlsNo ratings yet
- jcm-10-04135Document30 pagesjcm-10-04135xpv88f496kNo ratings yet
- AfasiaDocument14 pagesAfasiaPilar Araya JofréNo ratings yet
- Physiologic Voice Rehabilitation BasedDocument10 pagesPhysiologic Voice Rehabilitation BasedESTEFANIA GEOVANNA MEJIA MACASNo ratings yet
- Black Beans PowerpointDocument16 pagesBlack Beans Powerpointk_drew210No ratings yet
- The Different Standard Hospital Diet Activity No. 17Document4 pagesThe Different Standard Hospital Diet Activity No. 17Luis WashingtonNo ratings yet
- AP DSC Pet Syllabus 2015Document4 pagesAP DSC Pet Syllabus 2015Mruthyunjay100% (2)
- Lung Radiotherapy General Guidelines CRT ServiceDocument3 pagesLung Radiotherapy General Guidelines CRT ServicebigskyNo ratings yet
- Buffering Systems Major UrinaryDocument4 pagesBuffering Systems Major UrinaryAllan Takudzwa MpeperekiNo ratings yet
- Kerdal's Paper 1 PractcieDocument9 pagesKerdal's Paper 1 PractcieKerdal MathurinNo ratings yet
- Acute Neuropsychiatric Disorders in Adolecenst and Young Adults With Down Syndrome: Japanese Case ReportsDocument7 pagesAcute Neuropsychiatric Disorders in Adolecenst and Young Adults With Down Syndrome: Japanese Case ReportsPar DoNo ratings yet
- Get The Code Stroke Handbook: Approach to the Acute Stroke Patient Andrew Micieli PDF ebook with Full Chapters NowDocument65 pagesGet The Code Stroke Handbook: Approach to the Acute Stroke Patient Andrew Micieli PDF ebook with Full Chapters Nowteslaezraehd100% (5)
- Ys Eng June 2013Document68 pagesYs Eng June 2013Bheemesh GudelliNo ratings yet
- Heart Attack and Cardiac ArrestDocument2 pagesHeart Attack and Cardiac ArrestCarlos Alberto Cabezas GuerreroNo ratings yet
- Benazepril Hydro ChlorideDocument3 pagesBenazepril Hydro Chlorideapi-3797941No ratings yet
- Knowledge, Attitudes, and Practices (Kap) Surveys During Cholera Vaccination Campaigns: Guidance For Oral Cholera Vaccine Stockpile CampaignsDocument41 pagesKnowledge, Attitudes, and Practices (Kap) Surveys During Cholera Vaccination Campaigns: Guidance For Oral Cholera Vaccine Stockpile CampaignsmadhavNo ratings yet
- 11 Tips To Treat InsomniaDocument7 pages11 Tips To Treat Insomniashivaniikumarii7889No ratings yet
- Biology Notes IB Free ResponseDocument26 pagesBiology Notes IB Free ResponseLarry LohNo ratings yet
- Bull Cat 3Document45 pagesBull Cat 3totochakrabortyNo ratings yet
- 12 Strongmen in the Bible 1Document2 pages12 Strongmen in the Bible 1hzzz74mvx5No ratings yet
- TeleTech HMO Coverage Summary UPDATED 10-01-15Document12 pagesTeleTech HMO Coverage Summary UPDATED 10-01-15Ricardo MagnoNo ratings yet
- E 'Marea Bourke The Ageing Angel' Presented To Angelman Syndrome Conference 2018 by Judy BourkeDocument24 pagesE 'Marea Bourke The Ageing Angel' Presented To Angelman Syndrome Conference 2018 by Judy BourkeIan KirkwoodNo ratings yet
- Health - LP For CotDocument4 pagesHealth - LP For CotHoney JinNo ratings yet
- Drug Study - DexamethasoneDocument2 pagesDrug Study - DexamethasoneCarla Tongson Maravilla100% (3)
- Anti 10 PDFDocument5 pagesAnti 10 PDFTetteh JudeNo ratings yet
- Hospitalisation Claim FormDocument2 pagesHospitalisation Claim Formsujay13780No ratings yet
- Hcin 545 Residency JournalDocument6 pagesHcin 545 Residency Journalapi-408487557No ratings yet
- Poison ReviewerDocument2 pagesPoison ReviewerMarilyn-Arlet EpiscopeNo ratings yet
- Arogya Dhama BrochireDocument4 pagesArogya Dhama Brochiresai priyathamNo ratings yet
- Peta Persebaran Asf Di Indonesia: 1. Medan 2. Lampung 3. Pontianak 4. Jawa 5. Bali 6. NTT 7. Manado 8. PapuaDocument3 pagesPeta Persebaran Asf Di Indonesia: 1. Medan 2. Lampung 3. Pontianak 4. Jawa 5. Bali 6. NTT 7. Manado 8. PapuaCt ZahraNo ratings yet
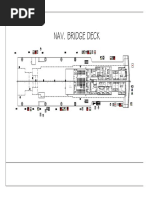
- Fire Control Plan - Nav - Bridge DeckDocument1 pageFire Control Plan - Nav - Bridge DeckJephthah Jude Tadeo GaleosNo ratings yet
- Niosome Final...Document9 pagesNiosome Final...Ajma LineNo ratings yet
- Latihan USBNDocument5 pagesLatihan USBNbilly jordiNo ratings yet
- Acute Lymphoblastic Leukemia (ALL)Document21 pagesAcute Lymphoblastic Leukemia (ALL)Moayd M. ShakhelNo ratings yet