Assessment of An ICU Patient
Assessment of An ICU Patient
Download as pdf or txt
You might also like
- E-Pass: COVID - 19Document2 pagesE-Pass: COVID - 19Midhila GOPINATHNo ratings yet
- Integrated Cath Lab Safety ChecklistDocument2 pagesIntegrated Cath Lab Safety Checklistwenhal100% (1)
- Guided Meditation ScriptDocument2 pagesGuided Meditation Scriptnerea_giordano80% (5)
- Perioperative RN Basic Skills Self AssessmentDocument17 pagesPerioperative RN Basic Skills Self AssessmentAndre James VelascoNo ratings yet
- Naqshbandi Sufi MeditationDocument75 pagesNaqshbandi Sufi MeditationAbdul Faheem88% (8)
- Respiratory Therapist Skills ChecklistDocument3 pagesRespiratory Therapist Skills Checklisthealth careNo ratings yet
- ICU Note Writing GuidelinesDocument2 pagesICU Note Writing GuidelinesMohammedNo ratings yet
- Intra Operative MonitoringDocument4 pagesIntra Operative MonitoringEsamNo ratings yet
- Preoperative Checklist-1Document10 pagesPreoperative Checklist-1June Faith HacheroNo ratings yet
- Extention PDF Cath Lab TechDocument2 pagesExtention PDF Cath Lab TechChrisNo ratings yet
- NURSING CARE PLAN For Myocardial InfarctionDocument13 pagesNURSING CARE PLAN For Myocardial Infarctionbanyenye2593% (14)
- ICU Assessment Powerpoit Tuts1Document25 pagesICU Assessment Powerpoit Tuts1Sharom Salas100% (1)
- ICU WHO Safety Checklist v5Document2 pagesICU WHO Safety Checklist v576gnw5bkn2No ratings yet
- Management of The Critically Ill PatientDocument2 pagesManagement of The Critically Ill PatientLilay Makulay100% (1)
- ICU AssessmentDocument70 pagesICU AssessmentPraneetha100% (2)
- Manual IcuDocument229 pagesManual IcuMauricio Pinneapar100% (1)
- Discharge Summary FormatDocument14 pagesDischarge Summary Formatenumula kumarNo ratings yet
- 5 Reducing Time To Analgesia in The Emergency Department Using ADocument10 pages5 Reducing Time To Analgesia in The Emergency Department Using AMegaHandayaniNo ratings yet
- Emergency Severity Index: Adlyn Bea A. Bernaldez, MD Second Year Family Medicine BihmiDocument35 pagesEmergency Severity Index: Adlyn Bea A. Bernaldez, MD Second Year Family Medicine BihmiAdlyn Bea Albesa-BernaldezNo ratings yet
- Post Operative HemorrhageDocument16 pagesPost Operative Hemorrhagenishimura89No ratings yet
- Daily Assessment Chart ICUDocument16 pagesDaily Assessment Chart ICUaiman abushahma100% (1)
- OPD GuideDocument1 pageOPD GuideAbdul BasitNo ratings yet
- Recovery Room NurseDocument5 pagesRecovery Room NurseChristin 'Kirei' AndoloNo ratings yet
- File ChecklistDocument2 pagesFile ChecklistNoor ButtNo ratings yet
- Critical Care Skills Check ListDocument3 pagesCritical Care Skills Check Listhemarani60605582100% (1)
- Anesthesiology Pre-Op Evaluation: ExovsrtsDocument1 pageAnesthesiology Pre-Op Evaluation: Exovsrtssabbo morsNo ratings yet
- Initial Assessment and ManagementDocument8 pagesInitial Assessment and ManagementAlvin De LunaNo ratings yet
- Emergency Ward PDFDocument30 pagesEmergency Ward PDFdolar buhaNo ratings yet
- By Accident and Emergency Specialist Dr. Mahmoud Al-Jama'einDocument25 pagesBy Accident and Emergency Specialist Dr. Mahmoud Al-Jama'einHussein Qunash-JordanNo ratings yet
- NABH IntroductionDocument12 pagesNABH IntroductionKrishna100% (1)
- Apache ScoreDocument36 pagesApache ScoreSugianto Parulian SimanjuntakNo ratings yet
- ATT 1 Guidelines For ICU Admission-Discharge-And-TriageDocument3 pagesATT 1 Guidelines For ICU Admission-Discharge-And-TriageEmad Zakaria Sayed100% (1)
- INOTROPIC SUPPORT (Autosaved)Document23 pagesINOTROPIC SUPPORT (Autosaved)Bindhu Rani100% (1)
- Perioperatif Nursing PDFDocument93 pagesPerioperatif Nursing PDFNurvanny HusnaNo ratings yet
- Necrotizing Otitis 2022Document20 pagesNecrotizing Otitis 2022asmashNo ratings yet
- Assessment of Critically Ill PatientsDocument4 pagesAssessment of Critically Ill PatientsAa Aa100% (1)
- Intraoperative CareDocument5 pagesIntraoperative CareraffineeNo ratings yet
- Protocol Needlestick InjuriesDocument1 pageProtocol Needlestick InjuriesMrLarry Dolor100% (1)
- Nursing Cares For Hemodialysis Patient: Hemodialysis Vascular Access: Assess TheDocument34 pagesNursing Cares For Hemodialysis Patient: Hemodialysis Vascular Access: Assess TheEDz Delica SandovalNo ratings yet
- Airway Obstruction - Types, Causes, and SymptomsDocument6 pagesAirway Obstruction - Types, Causes, and SymptomsGilbertLiem100% (1)
- Please Read The Entire Form Carefully Before SigningDocument2 pagesPlease Read The Entire Form Carefully Before SigningKoh LudzNo ratings yet
- TraumaDocument12 pagesTraumagibreilNo ratings yet
- Ward Round Checklist v4 1Document1 pageWard Round Checklist v4 1Phanindra KazipetaNo ratings yet
- Recovery Room Transfer Sheet44Document1 pageRecovery Room Transfer Sheet44Dr. Sumit Kumbhar0% (1)
- CvicuDocument2 pagesCvicuapi-401768894No ratings yet
- Siyu 2Document4 pagesSiyu 2siti nur asiahNo ratings yet
- Infection Control Care BundlesDocument41 pagesInfection Control Care BundlesGrace AngelinaNo ratings yet
- BMC Cath Lab Fellow Manual 2013Document25 pagesBMC Cath Lab Fellow Manual 2013anshashamsuthottathilNo ratings yet
- Opd ScheduleDocument14 pagesOpd ScheduleRamananda BaikadyNo ratings yet
- General Information 3.fluid-Remobilization PhaseDocument4 pagesGeneral Information 3.fluid-Remobilization Phasejulie-pearl-632967% (3)
- Abcs of Trauma CareDocument65 pagesAbcs of Trauma CareBeaulah HunidzariraNo ratings yet
- CCN Course Grid 2024Document38 pagesCCN Course Grid 2024neelumshaukatNo ratings yet
- Preprocedure Check-In Sign-In Time-Out Sign-OutDocument2 pagesPreprocedure Check-In Sign-In Time-Out Sign-OutSyahri DzikriNo ratings yet
- Initial Assessment and ManagementDocument13 pagesInitial Assessment and ManagementterriNo ratings yet
- Critical Care Lecture NotesDocument10 pagesCritical Care Lecture Notesapi-280066855No ratings yet
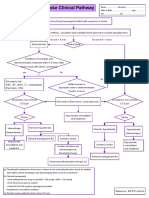
- Stroke Clinical PathwayDocument1 pageStroke Clinical PathwayKanoknun PisitpatcaragulNo ratings yet
- Adult Emergency Nurse Protocol HEAD INJURY (Closed)Document3 pagesAdult Emergency Nurse Protocol HEAD INJURY (Closed)widyadariNo ratings yet
- Sedation & General Anesthesia: SMF Anestesiologi & Reanimasi, Intensive Care Rsud JayapuraDocument50 pagesSedation & General Anesthesia: SMF Anestesiologi & Reanimasi, Intensive Care Rsud JayapuraubayyumrNo ratings yet
- Assessment of bleeding Shock in a Politraumatized PatientFrom EverandAssessment of bleeding Shock in a Politraumatized PatientNo ratings yet
- Peppermint (Mentha Piperita) : Paula Gardiner, MDDocument22 pagesPeppermint (Mentha Piperita) : Paula Gardiner, MDnuraji090689No ratings yet
- 5090 w12 QP 11Document20 pages5090 w12 QP 11mstudy123456No ratings yet
- Megabrain Software HutchisonDocument26 pagesMegabrain Software HutchisonAlexandre BatissouNo ratings yet
- Meditation Guide: I Focus and WriteDocument2 pagesMeditation Guide: I Focus and WriteEmmanuel GoldsteinNo ratings yet
- Nursing Fundamental Q&ADocument26 pagesNursing Fundamental Q&ALinjumol T GNo ratings yet
- Testosterone Optimisation NewDocument15 pagesTestosterone Optimisation NewWillNo ratings yet
- ISO 10651 Part 6Document38 pagesISO 10651 Part 6omkar daveNo ratings yet
- D 5001 - 90a R95 Ball-on-Cylinder Lubricity EvaluatorDocument6 pagesD 5001 - 90a R95 Ball-on-Cylinder Lubricity Evaluatoreduardoperez.uniNo ratings yet
- Nebulization Therapy ProcedureDocument8 pagesNebulization Therapy ProcedureMohamed Hamdy100% (1)
- Complications Part B: Aaahhh The Pain, The Pleasure A Confusing Mixture. Hastily, I Retreated To TheDocument7 pagesComplications Part B: Aaahhh The Pain, The Pleasure A Confusing Mixture. Hastily, I Retreated To TheJennica Monique Tiu CequinaNo ratings yet
- Emergency ScenarioDocument4 pagesEmergency ScenarioArjuna BuduhNo ratings yet
- Respiratory Physiology Lab ReportDocument15 pagesRespiratory Physiology Lab ReportThalia PacamalanNo ratings yet
- Vital Signs LectureDocument67 pagesVital Signs LectureJayrelle D. Safran100% (2)
- Spherical Breathing by Drunvalo MelchizedekDocument8 pagesSpherical Breathing by Drunvalo MelchizedekDavid Jose Lopez Wong0% (1)
- VBT Translation WALLIS-2Document28 pagesVBT Translation WALLIS-2Padmakumar KarthikNo ratings yet
- Hide and Drink by SavageDocument405 pagesHide and Drink by SavageLheinrich2100% (1)
- PASSAGES EditedDocument56 pagesPASSAGES EditedNIZA GALLEGOSNo ratings yet
- Skill 20: Bag-Valve-Mask Ventilation Task:: ChecklistDocument3 pagesSkill 20: Bag-Valve-Mask Ventilation Task:: ChecklistThulasi tootsie100% (3)
- Invest in The Now - Jordan KimmelDocument106 pagesInvest in The Now - Jordan Kimmela.ar.us.ho.wen93.0No ratings yet
- Vocal LessonDocument61 pagesVocal LessonLonnie Marlin100% (1)
- List of Affirmations To Calm FearsDocument2 pagesList of Affirmations To Calm FearsRomina RomanNo ratings yet
- Licensure Examination For BSC Nursing Graduates Prepared by Fmoh, June 2019Document17 pagesLicensure Examination For BSC Nursing Graduates Prepared by Fmoh, June 2019Nebaw100% (1)
- Module 08: Respiration Assessment and Management: TCCC Tier 4 TCCC Tier 1 TCCC Tier 3Document24 pagesModule 08: Respiration Assessment and Management: TCCC Tier 4 TCCC Tier 1 TCCC Tier 3Luis-alfredo Perez Bolde HernandezNo ratings yet
- What Is Overthinking?Document3 pagesWhat Is Overthinking?salmaan khawerNo ratings yet
- Defend Tartar+ Stain Remover MSDS 1-1-2011Document1 pageDefend Tartar+ Stain Remover MSDS 1-1-2011M. White DentalNo ratings yet
- The Dynamics of BreathingDocument5 pagesThe Dynamics of BreathingChris McCulloch100% (1)
- Government of The People's Republic of Bangladesh Sample Question Bank For Certificate of Proficiency (COP) MCQ ExamDocument17 pagesGovernment of The People's Republic of Bangladesh Sample Question Bank For Certificate of Proficiency (COP) MCQ ExamMd.Iskender MirjaNo ratings yet