Abcs of Trauma Care
Abcs of Trauma Care
Download as pdf or txt
You might also like
- Warm Up Questions and Answers Oet MaterialsDocument3 pagesWarm Up Questions and Answers Oet Materialsjijo kurian mathew100% (10)
- Designing Your Ultimate Life - Masterclass Workbook (Editable PDF)Document18 pagesDesigning Your Ultimate Life - Masterclass Workbook (Editable PDF)Beaulah Hunidzarira100% (7)
- Physical Examination IPPA CHECKLISTDocument1 pagePhysical Examination IPPA CHECKLISTJewel Ann NuñezNo ratings yet
- Arizona Paramedic Scope of Practice PDFDocument4 pagesArizona Paramedic Scope of Practice PDFapi-2631808990% (1)
- Case Studies For PharmacyDocument3 pagesCase Studies For PharmacyMahima Sindhi75% (4)
- MCQ - AyurvedaDocument4 pagesMCQ - AyurvedaAmacus Nirvana100% (4)
- Initial Assessment and ManagementDocument8 pagesInitial Assessment and ManagementAlvin De LunaNo ratings yet
- ICU Assessment Powerpoit Tuts1Document25 pagesICU Assessment Powerpoit Tuts1Sharom Salas100% (1)
- Relias Dysrhythmia Basic Test 35 Questions and Answers 2024Document5 pagesRelias Dysrhythmia Basic Test 35 Questions and Answers 2024muthiimorris68No ratings yet
- Nursing CS End of Shift Checklist 03Document1 pageNursing CS End of Shift Checklist 03Ciara GonzalezNo ratings yet
- NURS FPX 4000 Assessment 2Document8 pagesNURS FPX 4000 Assessment 2BSN Writing ServicesNo ratings yet
- Med ReconDocument17 pagesMed ReconStephanie Camille SamonteNo ratings yet
- Acute Respiratory Distress: Section I: Scenario DemographicsDocument6 pagesAcute Respiratory Distress: Section I: Scenario DemographicsharasthaNo ratings yet
- Emergency Nurse Protocol Back PainDocument2 pagesEmergency Nurse Protocol Back PainSimon S. KledenNo ratings yet
- By Accident and Emergency Specialist Dr. Mahmoud Al-Jama'einDocument25 pagesBy Accident and Emergency Specialist Dr. Mahmoud Al-Jama'einHussein Qunash-JordanNo ratings yet
- OMM MidtermDocument24 pagesOMM MidtermBhumiShah100% (1)
- Induced HPDocument4 pagesInduced HPmaddythedocNo ratings yet
- Jarvis Complete Phys ExamDocument9 pagesJarvis Complete Phys ExamYadile D BenoitNo ratings yet
- Algorithm For Helping With Cardiac ArrestDocument52 pagesAlgorithm For Helping With Cardiac ArrestOlga GoryachevaNo ratings yet
- Approach in Trauma Patient - OrthopaedicDocument91 pagesApproach in Trauma Patient - OrthopaedicBesi Tua100% (1)
- Capstone Nursing PaperDocument6 pagesCapstone Nursing Paperapi-505543314No ratings yet
- Best Vasopressor For Advanced Vasodilatory Shock Should Vasopressin Be Part of The MixDocument4 pagesBest Vasopressor For Advanced Vasodilatory Shock Should Vasopressin Be Part of The MixSurachai PraimaiNo ratings yet
- ATLSDocument92 pagesATLSRendi MuflihNo ratings yet
- Epworth Richmond - Agency Staff Orientation Booklet MAY 2016Document33 pagesEpworth Richmond - Agency Staff Orientation Booklet MAY 2016Anonymous BaD9jQNo ratings yet
- Final Emergency Medicine En-1Document2 pagesFinal Emergency Medicine En-1Wen Jie LauNo ratings yet
- Cor PulmonaleDocument8 pagesCor PulmonaleAymen OmerNo ratings yet
- Eusem Epi Guidelines March 2020 PDFDocument92 pagesEusem Epi Guidelines March 2020 PDFАлекс КейNo ratings yet
- RECMOD2 Primary and Secondary SurveyDocument56 pagesRECMOD2 Primary and Secondary Surveydragon66100% (1)
- 02 The Abdominal Exam Lab - CopDocument6 pages02 The Abdominal Exam Lab - CopBhumiShahNo ratings yet
- Venous ThromboembolismDocument49 pagesVenous Thromboembolismadamu mohammadNo ratings yet
- 4 PT Report SheetDocument1 page4 PT Report SheetAneesNo ratings yet
- Sedation & General Anesthesia: SMF Anestesiologi & Reanimasi, Intensive Care Rsud JayapuraDocument50 pagesSedation & General Anesthesia: SMF Anestesiologi & Reanimasi, Intensive Care Rsud JayapuraubayyumrNo ratings yet
- Aldrete Discharge Scoring - Appropriate For Post Anesthesia Phase PDFDocument29 pagesAldrete Discharge Scoring - Appropriate For Post Anesthesia Phase PDFSurya BugisNo ratings yet
- Nationalsnakebitemanagementprotocol PDFDocument66 pagesNationalsnakebitemanagementprotocol PDFDeep ShahNo ratings yet
- 2.criticalcare29 7 MinDocument63 pages2.criticalcare29 7 MinSAUMOJIT MAJUMDERNo ratings yet
- ACLS ACS Algorithm NewDocument3 pagesACLS ACS Algorithm Newsambo100% (1)
- Triage in Polytauma: Prof. Dr. A. Chandrasekaran M.S., PH.D.Document73 pagesTriage in Polytauma: Prof. Dr. A. Chandrasekaran M.S., PH.D.ShrutiNo ratings yet
- Nsg241 Study Guide Exam 5Document76 pagesNsg241 Study Guide Exam 5NatalieAndersonNo ratings yet
- Initial Assessment and ManagementDocument13 pagesInitial Assessment and ManagementterriNo ratings yet
- Module E Shock, MODS Roy Model-Oxygenation-Perfusion Required Readings (See Syllabus For Detailed Reading)Document7 pagesModule E Shock, MODS Roy Model-Oxygenation-Perfusion Required Readings (See Syllabus For Detailed Reading)Jeff ZhouNo ratings yet
- Trauma Nursing Core Course: Preparation PacketDocument13 pagesTrauma Nursing Core Course: Preparation PacketJimmy NaglesNo ratings yet
- Perioperative Pre-Class Mini-Lecture - CH 17-19Document22 pagesPerioperative Pre-Class Mini-Lecture - CH 17-19Marcel YoungNo ratings yet
- ECG Interpretation and Dysrhythmias: Karen L. O'Brien MSN, RN JAN 07Document60 pagesECG Interpretation and Dysrhythmias: Karen L. O'Brien MSN, RN JAN 07ampogison08No ratings yet
- Cardiac Monitor, ECG and CauterizationDocument28 pagesCardiac Monitor, ECG and CauterizationGlaiza Mae Olivar-ArguillesNo ratings yet
- Acls TachiDocument1 pageAcls TachiratnawkNo ratings yet
- 15Document21 pages15Tyson Easo JonesNo ratings yet
- Pals Prep MaterialsDocument20 pagesPals Prep MaterialshckuserNo ratings yet
- Malignant Hyperthermia Fact SheetDocument2 pagesMalignant Hyperthermia Fact Sheetapi-301819201No ratings yet
- Chapter 5: Analyzing A Rhythm StripDocument7 pagesChapter 5: Analyzing A Rhythm StriptellyNo ratings yet
- Emergency Severity Index Guidelines For Triage CeuDocument71 pagesEmergency Severity Index Guidelines For Triage Ceuani mulyani100% (1)
- ABCs of Thoracic TraumaDocument5 pagesABCs of Thoracic TraumaAlice S ChangNo ratings yet
- IV Access and Medication AdministrationDocument47 pagesIV Access and Medication AdministrationbrentupdegraffNo ratings yet
- Traum ManagementDocument7 pagesTraum Managementchinthaka18389021No ratings yet
- Atsp Book 2011Document24 pagesAtsp Book 2011Chengyuan ZhangNo ratings yet
- Ventricular Tachycardia Bsn3b-Grp1Document35 pagesVentricular Tachycardia Bsn3b-Grp1Jessica RamosNo ratings yet
- Acls 30-10-23Document63 pagesAcls 30-10-23lakshmiNo ratings yet
- Critical Care Nurse Skills ChecklistDocument4 pagesCritical Care Nurse Skills Checklistspartacuslives100% (1)
- Revisions To The Canadian Emergency Department Triage and Acuity Scale Implementation GuidelinesDocument8 pagesRevisions To The Canadian Emergency Department Triage and Acuity Scale Implementation GuidelinesTiti Multi SaariNo ratings yet
- Shockable and Unshockable RhytmDocument39 pagesShockable and Unshockable Rhytmariahenkus100% (1)
- Test - TNCC TraumaDocument12 pagesTest - TNCC Traumaleonardo orozcoNo ratings yet
- Chapter 26 Management of Patients With Dysrhythmias and Conduction ProblemsDocument22 pagesChapter 26 Management of Patients With Dysrhythmias and Conduction ProblemsAbel C. Idusma Jr.No ratings yet
- Step Down RN or Progressive Care Skills ChecklistDocument4 pagesStep Down RN or Progressive Care Skills Checklisthealth careNo ratings yet
- Algo Bradycardia DikonversiDocument5 pagesAlgo Bradycardia DikonversiDaniel SitungkirNo ratings yet
- Pan London Major Trauma System Management of Older Trauma. Third Editionapril 2021Document31 pagesPan London Major Trauma System Management of Older Trauma. Third Editionapril 2021Beaulah HunidzariraNo ratings yet
- 2018 - 06 - 18 BMJ The Trauma CallDocument8 pages2018 - 06 - 18 BMJ The Trauma CallBeaulah HunidzariraNo ratings yet
- SD502 (V22) 05.2021Document4 pagesSD502 (V22) 05.2021Beaulah HunidzariraNo ratings yet
- Aintree Application FormDocument1 pageAintree Application FormBeaulah HunidzariraNo ratings yet
- Clinical Audit in Ophthalmology The Why and HowDocument4 pagesClinical Audit in Ophthalmology The Why and HowBeaulah HunidzariraNo ratings yet
- Lower Back Exercise Guide by Dr. Walter SalubroDocument37 pagesLower Back Exercise Guide by Dr. Walter SalubroBeaulah Hunidzarira100% (1)
- Antrim Handbook-2018Document223 pagesAntrim Handbook-2018Beaulah HunidzariraNo ratings yet
- High Yield Plab TopicsDocument20 pagesHigh Yield Plab TopicsBeaulah HunidzariraNo ratings yet
- Standards, Principles and Approaches in Occupational Health ServicesDocument24 pagesStandards, Principles and Approaches in Occupational Health ServicesBeaulah HunidzariraNo ratings yet
- 19 July - Workers Compensation and Rehabilitation Coal Workers Pneumoconiosis and Other Legislation Amendment Bill 2017Document5 pages19 July - Workers Compensation and Rehabilitation Coal Workers Pneumoconiosis and Other Legislation Amendment Bill 2017Beaulah HunidzariraNo ratings yet
- AFP Nonmelanoma Skin CancersDocument5 pagesAFP Nonmelanoma Skin CancersBeaulah HunidzariraNo ratings yet
- Racgp Floaters and Flashes OpthalmologyDocument3 pagesRacgp Floaters and Flashes OpthalmologyBeaulah HunidzariraNo ratings yet
- ENT MCQsDocument13 pagesENT MCQsSheikha100% (2)
- Drug Study - MONTELUKASTDocument3 pagesDrug Study - MONTELUKASTCHRISTINE GRACE ELLONo ratings yet
- OET Discharge Letter - Sample Letter For Doctors and NursesDocument5 pagesOET Discharge Letter - Sample Letter For Doctors and NursesClassNo ratings yet
- BreastfeedingDocument30 pagesBreastfeedingqueennita69100% (6)
- UK Foundation Programme Sample Questions (Final Oct 2021)Document9 pagesUK Foundation Programme Sample Questions (Final Oct 2021)chehjuanNo ratings yet
- Birthing Homes ReqDocument10 pagesBirthing Homes ReqMi Lagro100% (2)
- ANTITUSSIVESDocument5 pagesANTITUSSIVESJane IjeNo ratings yet
- Tema PediDocument9 pagesTema PediClaudiu Andrei MunteanuNo ratings yet
- Adult Class LLL Treatment Using A J-Hook Headgear To The Mandibular ArchDocument8 pagesAdult Class LLL Treatment Using A J-Hook Headgear To The Mandibular ArchRocioNo ratings yet
- Summary Suspension of Dr. Anthony FarinaDocument21 pagesSummary Suspension of Dr. Anthony FarinaNBC 10 WJARNo ratings yet
- Format For Medical Reimbursement-1Document5 pagesFormat For Medical Reimbursement-1hemantaduttaghy1No ratings yet
- PC Metabolic AcidosisDocument4 pagesPC Metabolic AcidosisErine Emmanuelle Cawaling Hetrosa50% (2)
- Analysis of Nidana, Lakshana, Chikitsha of Dosha Vriddhi, Kshaya and PrakopaDocument10 pagesAnalysis of Nidana, Lakshana, Chikitsha of Dosha Vriddhi, Kshaya and PrakopaSwagath N75% (4)
- Damage Control Orthopaedics (DC O: Presented by Specialist of Orthopedic& Traumatology Al-Mahmoudia General HospitalDocument52 pagesDamage Control Orthopaedics (DC O: Presented by Specialist of Orthopedic& Traumatology Al-Mahmoudia General HospitalpaswordnyalupaNo ratings yet
- Immunizations Health TeachingDocument9 pagesImmunizations Health TeachingClaudine Jo B. TalabocNo ratings yet
- AMOS Revision PaedsDocument2 pagesAMOS Revision PaedsDeborah AnneNo ratings yet
- Caton Et Al-2018-Journal of Clinical PeriodontologyDocument8 pagesCaton Et Al-2018-Journal of Clinical PeriodontologyWirajulay Pratiwi SanusiNo ratings yet
- Generan Anaesthesia For DentistryDocument13 pagesGeneran Anaesthesia For DentistrynissadhaniaNo ratings yet
- Loa LoaDocument2 pagesLoa LoaShvan EzatNo ratings yet
- Central Library Books & JournalslDocument201 pagesCentral Library Books & Journalslsunil kumarNo ratings yet
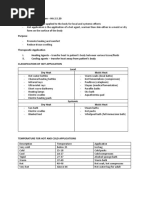
- Heat and Cold ApplicationDocument5 pagesHeat and Cold ApplicationBern NerquitNo ratings yet
- PROJECT IN MAPEH FIRST AID KIT (AutoRecovered)Document17 pagesPROJECT IN MAPEH FIRST AID KIT (AutoRecovered)Abigail Lim BarbosaNo ratings yet
- Lyme NeurotoxinsDocument46 pagesLyme NeurotoxinsJohnny Atman100% (1)
- Daftar Pustaka KtiDocument6 pagesDaftar Pustaka KtiayuNo ratings yet
- Abstract BookDocument28 pagesAbstract BookParjanya ShuklaNo ratings yet
- Ayano G. Bipolar Disorder: A Concise Overview of Etiology, Epidemiology Diagnosis and Management: Review of Literatures. Ethiopia: Symbiosis. 2016Document2 pagesAyano G. Bipolar Disorder: A Concise Overview of Etiology, Epidemiology Diagnosis and Management: Review of Literatures. Ethiopia: Symbiosis. 2016boomNo ratings yet