Case of Ben Case Pre
Case of Ben Case Pre
Download as doc, pdf, or txt
You might also like
- Bipolar Disorder Mixed Episode Case StudyDocument14 pagesBipolar Disorder Mixed Episode Case Studyapi-658874568No ratings yet
- Psychiatric Mental Health Comprehensive Case Study 1Document11 pagesPsychiatric Mental Health Comprehensive Case Study 1api-402950137No ratings yet
- Mental Health Nursing Case StudyDocument11 pagesMental Health Nursing Case Studyapi-402957584100% (1)
- Psychiatric Mental Health Comprehensive Case StudyDocument12 pagesPsychiatric Mental Health Comprehensive Case Studyapi-593213381No ratings yet
- Psychiatric Mental Health Comprehensive Case StudyDocument10 pagesPsychiatric Mental Health Comprehensive Case Studyapi-526815418No ratings yet
- Case Study-1Document11 pagesCase Study-1Aysha KabeerNo ratings yet
- Case StudyDocument10 pagesCase Studyapi-453119244No ratings yet
- Case StudyDocument12 pagesCase Studyapi-447634418No ratings yet
- 1.A Ndera CaseDocument13 pages1.A Ndera CaseNsengimana Eric MaxigyNo ratings yet
- Psych Case StudyDocument11 pagesPsych Case Studyapi-663879907No ratings yet
- A Case Study of A Patient Suffering From Major Depressive DisorderDocument5 pagesA Case Study of A Patient Suffering From Major Depressive Disorderdennis ndegeNo ratings yet
- Case StudyDocument10 pagesCase Studyapi-508559825No ratings yet
- Case Study BipolarDocument22 pagesCase Study BipolarRobert de Guzman Jr.93% (29)
- CWU Psychiatry 1.1Document8 pagesCWU Psychiatry 1.1Codillia CheongNo ratings yet
- Major Depression Case 2Document14 pagesMajor Depression Case 2Mahnoor Malik100% (1)
- Schizophrenia NCMH Case StudyDocument45 pagesSchizophrenia NCMH Case StudyHomework PingNo ratings yet
- Major Depressive DisorderDocument5 pagesMajor Depressive DisorderAreej IdreesNo ratings yet
- Cases from the Psychiatry Letter - I: Cases from the Psychiatry Letter, #1From EverandCases from the Psychiatry Letter - I: Cases from the Psychiatry Letter, #1Rating: 5 out of 5 stars5/5 (1)
- Mental Health Case StudyDocument9 pagesMental Health Case Studyapi-400421073No ratings yet
- Mental Health Case StudyDocument12 pagesMental Health Case Studyapi-546884730No ratings yet
- Untitled Document-15Document12 pagesUntitled Document-15api-740900940No ratings yet
- Psychiatric Mental Health Case StudyDocument11 pagesPsychiatric Mental Health Case Studyapi-546332329No ratings yet
- Case Presentation SchizoDocument13 pagesCase Presentation SchizoBarbara Detaro100% (1)
- Clinical ReportDocument54 pagesClinical Reportlabiqakhawaja123No ratings yet
- Case 2Document7 pagesCase 2Muhammad Usman Bin TahirNo ratings yet
- CaseDocument5 pagesCaseFOM SEGi KDNo ratings yet
- Case Study BipolarDocument12 pagesCase Study Bipolarapi-353954238No ratings yet
- Case Analysis SchizoDocument4 pagesCase Analysis SchizoiamELHIZANo ratings yet
- Mental Health Recovery Book: An expose by the mother of a son with schizophrenia including care, nutrition and living within the family unitFrom EverandMental Health Recovery Book: An expose by the mother of a son with schizophrenia including care, nutrition and living within the family unitNo ratings yet
- Schizophrenia NCMH Case StudyDocument45 pagesSchizophrenia NCMH Case StudyNickale Peralta100% (1)
- Nurse's Notes: Significant AMSIT Data, Relevant Interview Information, Therapeutic Interventions Day 1 Day 2Document4 pagesNurse's Notes: Significant AMSIT Data, Relevant Interview Information, Therapeutic Interventions Day 1 Day 2ddelarosa29No ratings yet
- Experience With Mental IllnessDocument5 pagesExperience With Mental IllnessMARZIA MUNIRNo ratings yet
- John Sales ScsDocument12 pagesJohn Sales ScsRomeo Avecilla CabralNo ratings yet
- Case Study PsychDocument49 pagesCase Study PsychMonique Reyes100% (1)
- Positive Psychotherapy AssignmentsDocument9 pagesPositive Psychotherapy AssignmentsAyushi GargNo ratings yet
- Psych Case StudyDocument10 pagesPsych Case Studyapi-455759072No ratings yet
- Bipolar Affective DisorderDocument51 pagesBipolar Affective DisorderJazper Ian SorianoNo ratings yet
- Case No.7 SchizopherniaDocument18 pagesCase No.7 SchizopherniaAlyna QureshiNo ratings yet
- New Case StudyDocument15 pagesNew Case Studyapi-507336246No ratings yet
- Psychiatric Mental Health Comprehensive Case StudyDocument14 pagesPsychiatric Mental Health Comprehensive Case Studyapi-662323379100% (1)
- Case-Study-On-Schizophrenia Tacalan John VincentDocument4 pagesCase-Study-On-Schizophrenia Tacalan John VincentJayvee CornelioNo ratings yet
- Love Over LimbsDocument9 pagesLove Over LimbsGene Espino TrajecoNo ratings yet
- Drug AddictDocument17 pagesDrug AddictNoormah SaghirNo ratings yet
- PsychologyDocument40 pagesPsychologyDezalyn Mae CuteroNo ratings yet
- Case ReportDocument17 pagesCase ReportLai BaNo ratings yet
- Case StudyDocument10 pagesCase Studyapi-503254508No ratings yet
- NHHDocument30 pagesNHHRuth Jazelle MendozaNo ratings yet
- Grand Case PresentationDocument28 pagesGrand Case PresentationRae Marie AquinoNo ratings yet
- 3 Cases About Personality DisorderDocument8 pages3 Cases About Personality DisorderJeane Rose MacauyagNo ratings yet
- Case Study On PARANOID SCHIZOPHRENIA Melisa 19Document29 pagesCase Study On PARANOID SCHIZOPHRENIA Melisa 19MELISA ELEUTHERE100% (1)
- 2.B .Ndera CaseDocument9 pages2.B .Ndera CaseNsengimana Eric MaxigyNo ratings yet
- Case Study Caitlyn HoweDocument11 pagesCase Study Caitlyn Howeapi-738778945No ratings yet
- Mental Health Case StudyDocument10 pagesMental Health Case Studyapi-401649778No ratings yet
- Case AnalysisDocument6 pagesCase AnalysisEileen CeloricoNo ratings yet
- Case No 1:-Bio DataDocument8 pagesCase No 1:-Bio DataSarah Saqib Ahmad100% (1)
- Case StudyDocument15 pagesCase StudyRachel Frances SorillaNo ratings yet
- BSN 3Y2-2B Clinical Instructor: Aida I Bautista RN, MANDocument103 pagesBSN 3Y2-2B Clinical Instructor: Aida I Bautista RN, MANLara DollesinNo ratings yet
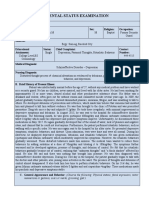
- Mental Status Examination: A. Baseline DataDocument5 pagesMental Status Examination: A. Baseline DataTherese MargaretNo ratings yet
- Psychiatric Comprehensive Case StudyDocument12 pagesPsychiatric Comprehensive Case Studyapi-544878035No ratings yet